TV4101 - SAM - Upper Airway Disease
Two broad presentations - coughing and dyspnoea
In contrast to lower airway disease - wet productive cough
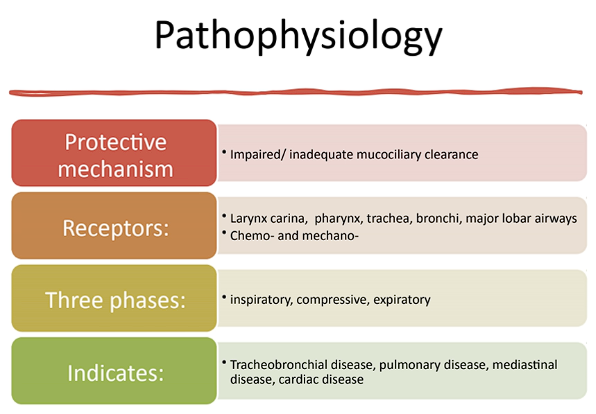
Cough is usally a protective mechanism to protect airway
Phases
Short sharp inspiration
Compressive phase against closed epiglottis
Mediastinal disease - could put pressure on airways
Physical exam - abnormal sounds, dyspnoea, trachea irritation?
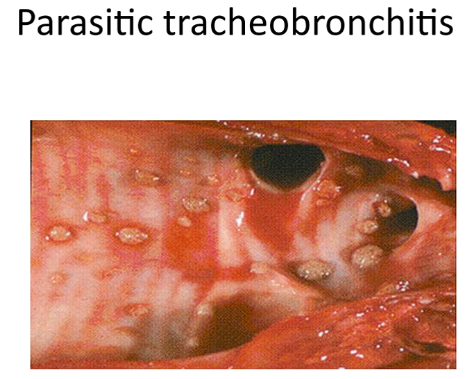
Faecal flotation e.g. con sider it if there is high worm burden i.e. larval migrans or area endemic to lung worms
Blood smear - neutrophilia, evidence of infection
Radiograph is our bitch
CT increased prevalence
mri not really used - movement of airways in breathing makes it blurry so eh
bronchoscopy - flexible scope to look at trachea and airways
blood gas analysis - used when concern with chronic hypoxia rarely used
cardiac evaluation - to look for pulmonary hypertension or consequences of lung diseases causing cardiac issues
FNA - better than biopsy as biopsy is open chest procedure
Risk of lung rupture
We stick needle into solid lesion that we saw on US
May stick needle into actual lung if we need dx of pneumonia
Bronchoalveolar lavage - 2ml per kg of saline given - don’t usually give that entire amount rather give in 2-5 ml minute amounts one syringe at a time then percuss
Relatively low risk procedure
If pulmonary bullous or moving tube and back forth could rupture ariway but very rare

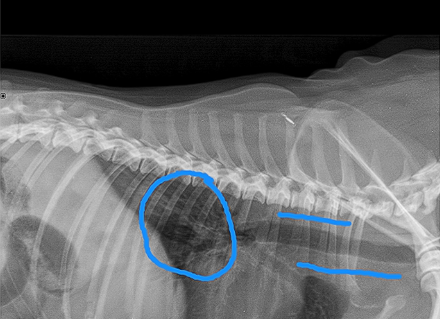
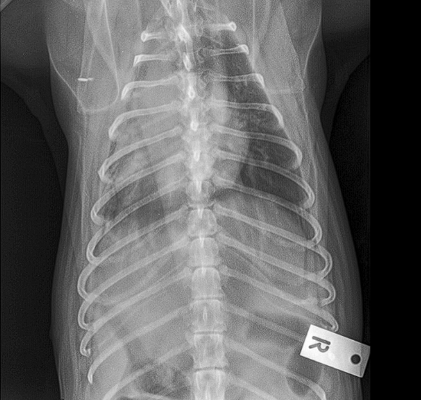
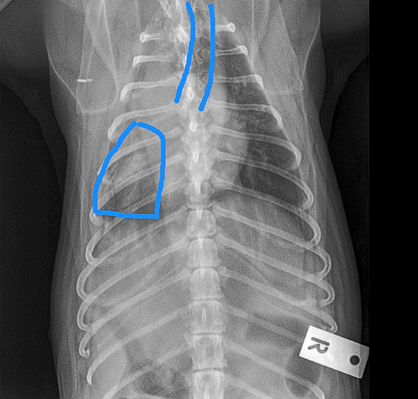
Little area of consolidation but nothing else significant
DX - chronic cough suspicions for airaway disease due to chronic unproductive cough
On left hand side (actually right ariway) airway is compressed
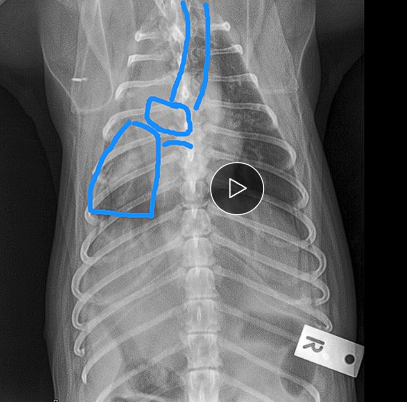
Wouldn’t be ablse to see mass on radiograph as heart borders block ti
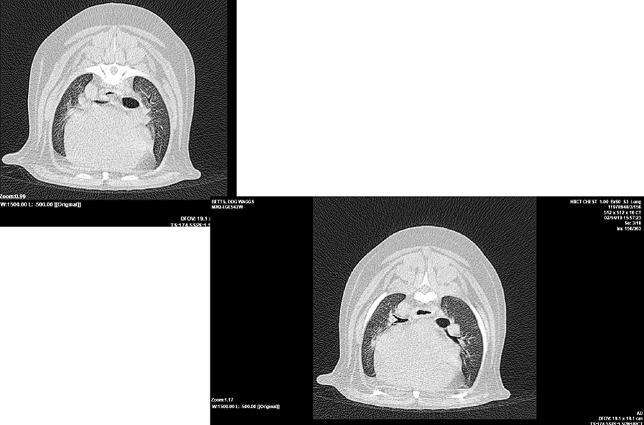
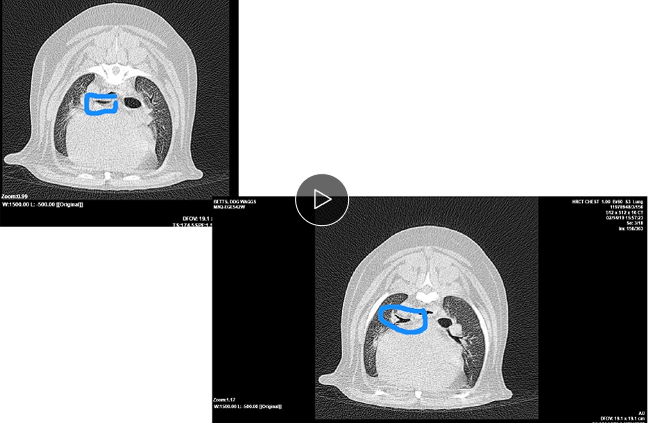
Bronchoscopy - wouldn’t be able to see the mass - only see the collapse but not what caused it
CT is our bitch
Common cause of cough
Breed and size predisposition implies genetic component
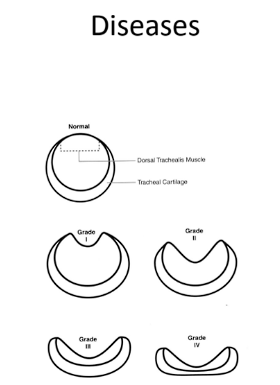
Weakening of trach rings → trache a collapse → activate mechanoreceptors → dry harsh cough
Tracheal stenting isn’t usually used, the above medications and weight loss aids enough to not need it
Tracheal stenting - to prevent life threatening airway obst
will continue to cough even if stented
Infectious - adeno, parainfulenza, boradtella
Non-infectious - separation anxiety barking lots → tracheitis
Compression of trachea → tracheitis
Infectious cases usually cough goes away on its own
May also use a nebuliser
Short term corticosteroids 5-7 d tx won’t cause immunosuppression
Immunity is not long lived
More in youngins
Most vax don’t prevent transmission
If cough is still there after 21 days - consider doxycycline to battle bordatella
Obesity a complication for resp pathology due to pigwiggian? syndrome → big belly push on diaphragm → extra layer of insulation and requires more air to cool down → more constriction of airway which is bad with resp pathology
Histology - mucus hypersecreion and hypertrophy of goblet cells
Important to rule out other diseases and we are left with chronic lower airway disease
Start with RGs,
Cardiac eval - may be helpful if very large chamber pushing on airway
Insidious - gradual, subtle and progressive
Sometimes cough is productive from increased mucus however hard to tell
TTA: neutrophils seen are non regen neutrophils
Culture for bal - hard to be pure from mouth contamination
Corticosteroids - oral prednisolone is the best
Astham pump - not tolerated very well by lots of dogs
2ndary
e.g. owner reduce smoking
Clean the house
Harness - less psi on cervical trachea
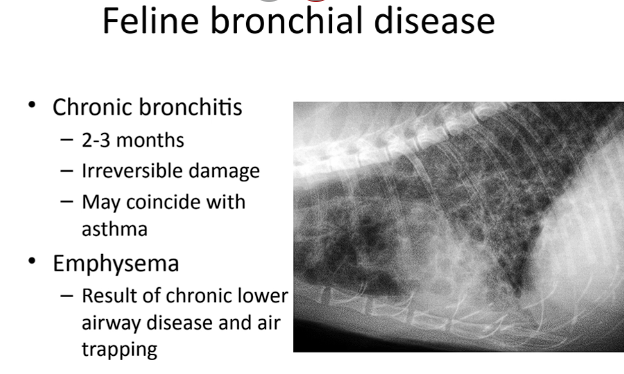
Bronchiectasis probably connected to chronic bronchitis
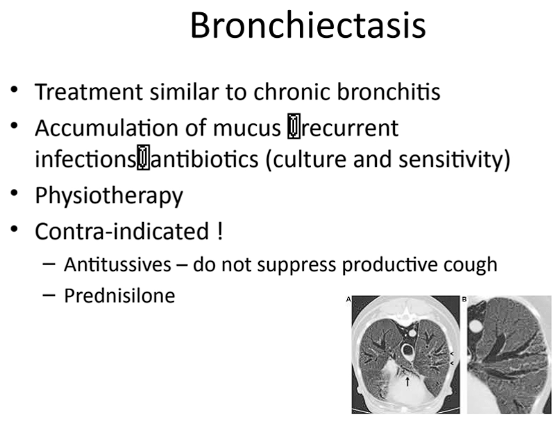
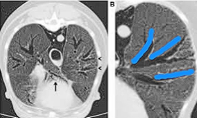
Can follow bronchi to the edge of the lung i.e. cylindrical bronchiestasis
TX - helpful to just treat with ABs
Prednisolone - can be helpful in bronchiestasis with a chronic cough (lots of inflam with no infection indicated) - don’t use long enough to suppress immune sys
Cats
Feline asthma - most common airway issue in feline - constrictive
Dogs have bronchitis as most common - infiltrative
Acute bronchitis - similar to what dogs get
Some cats with airway disease don’t respond well to astham tx → bronchial disease
Oft respond well to corticosteroids
Terbutaline - given as inhaler - already tweaking dyspnoeic cat might not like that very much
Anxiolytics to lower stress and inc resp
Environment - dry air, smoking etc
Experimental - eh
Ant-leukotrine doesn’t work in felines (works in humans)
Can use a pediatric pacer
May also have lung flukes but are uncommon
Dirofilaria immitis i.e. HW → coughing from larvae