Insulin
Mechanism of Action of Insulin
What is insulin? (Slide 2–3)
hormone produced by pancreatic beta cells.
Promotes glucose uptake for energy or storage as glycogen.
Regulates glucose homeostasis and prevents hyperglycemia/hypoglycemia.
Mechanism of action (Slides 4–6)
Insulin binds to insulin receptor (a tyrosine kinase receptor).
Stimulates GLUT-4 translocation → increased glucose entry into muscle and fat cells.
Promotes:
Glucose ➝ glycogen (liver, muscle).
Glucose ➝ fatty acids (adipose tissue).
Glucose ➝ pyruvate (glycolysis).
Key outcome: control of postprandial blood glucose.
2. Characteristics of Different Classes of Insulin
Types (Slide 7):
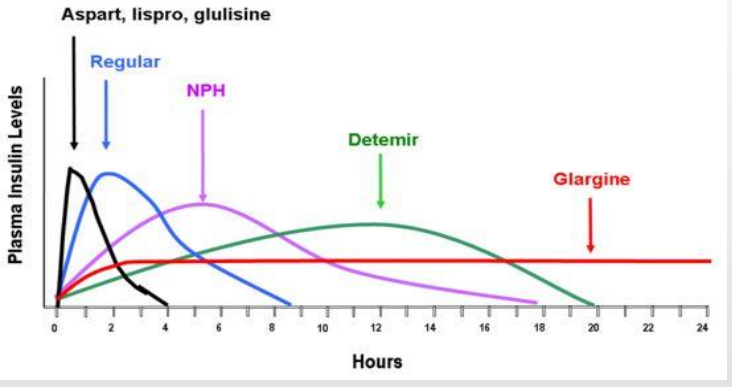
Rapid acting (lispro, aspart, glulisine). black
Short acting (regular). blue
Intermediate (NPH, mixes). pink
Long acting (detemir, glargine, degludec). green
Concentrated (U-500, U-200).
Inhaled (Afrezza).
the longer they last in body more risk for hyperglycemia
Rapid-acting Insulin (Slides 8–22)
Examples - Lispro (Humalog®, Admelog® biosimilar, Lyumjev®)
comes in U-100 and U-200 forms as pen and vials
Aspart (Novolog®, Fiasp®), Glulisine (Apidra®) all considered medically equivalent and interchangeable but still need new Rx to switch
Onset: ~15 min - 30 (Lyumjev/Fiasp slightly faster 12–13 min)
Peak: 1–3 hours. Duration: 3–5 hours.
Use: Bolus (mealtime); only class used in insulin pumps.
Special: U-200 lispro available 200 units/mL rest the same less volume less discomfort ; Fiasp contains nicotinamide (Vit B3 aka niacin) for faster absorption
Short-acting Insulin (Slides 23–25)
Regular insulin (Humulin R, Novolin R).
Onset: ~30 min. Peak: 2.5–5 h. Duration: 4–12 h.
Uses - IV infusion for diabetic emergencies DKA, HHS, TPN
less used outpatient due to slow onset and long duration vs. rapid-acting.
Intermediate-acting Insulin (Slides 26–30)
NPH (Neutral Protamine Hagedorn).
Cloudy suspension — must roll gently to mix (not shake).
Onset: 1–2 h. Peak: 4–12 h. Duration: 14–24 h.
Use - for cost-sensitive patients and in premixed products to cover liver glucose
Pre-mixed Insulin (Slides 31–34)
Combination of NPH + rapid/regular.
Examples: Humalog Mix 25/50, Novolog Mix 70/30, Novolin 70/30.
Onset: 15–30 min, Peak: 2–4 h, Duration: 14–24 h.
Reduces injections but less flexibility for individualized dosing.
Mixing Insulin (Slides 29–30)
Only mix rapid/short-acting + NPH. Do NOT mix with long-acting.
Steps:
Add air to NPH vial.
Add air to rapid/short-acting vial.
Draw rapid/short-acting first.
Then draw NPH.
Reason: Rapid/short-acting is clear; NPH is cloudy. NPH contamination would distort dosing.
Long-acting Insulin (Slides 35–46)
Detemir (Levemir®): 6–23 h, albumin binding, expected withdrawal 2026.
Glargine (Lantus®, Basaglar®, Semglee® U-100; Toujeo® U-300): 24 h or longer, peakless, forms micro precipitates that dissolve based on pH
Degludec (Tresiba®): >42 h duration, flat absorption, U-100/U-200, long stability (8 weeks after opening).
same pen but have different max, units/pen, dose settings, concentration
injected as long chains that dissociate from the ends
Typically once-daily, but some require BID.
Concentrated Insulin (Slides 47–49)
U-500 Regular: onset ~30 min, peak ~2–5 h, duration 12–24 h.
Used for insulin-resistant patients needing large doses.
onset like regular but duration of NPH
Inhaled Insulin (Afrezza®, Slides 50–53)
Onset: 12–15 min, Peak: ~1 h, Duration: 3 h.
Delivered via inhaler with cartridges (4, 8, 12 units).
Alternative to injections; not suitable in asthma or COPD.
units of 4 on the cartridges blue 4 green 8 yellow 12
3. Biosimilar Insulin (Slides 44–46)
Since March 2020, insulin regulated as biologic, allowing biosimilars.
Highly similar to approved biologic, with no meaningful clinical difference.
Can be interchanged at the pharmacy if designated as interchangeable.
Examples:
Semglee (glargine) biosimilar to Lantus.
Admelog (lispro) biosimilar to Humalog.
Basaglar (glargine) – similar but not technically a biosimilar at approval (now under biologic framework).
5. Choosing Appropriate Insulin for Therapy
Depends on patient characteristics, cost, timing of meals, lifestyle:
Rapid-acting ➝ mealtime coverage, flexible eating habits.
Regular ➝ inpatient use.
NPH ➝ cost-effective, 1–2 daily injections (but higher hypoglycemia risk).
Premix ➝ fewer injections but less flexibility.
Long-acting ➝ stable basal levels; fewer hypoglycemic events (esp. with degludec).
U-500 ➝ for insulin resistance with very high daily dose needs.
Afrezza ➝ needle-free bolus option (but restricted in lung disease).
6. Novel Insulins (Slides 47, 54)
Investigational pipeline (Slide 54):
Insulin icodec (weekly basal) — once-weekly dosing, improves adherence.
Insulin icosema (icodec + semaglutide dual agent).
Eli Lilly also testing weekly formulations.
Current innovations:
Longest-acting currently approved = degludec (>42h).
Weekly administration may significantly reduce injection burden, especially for type 2 diabetes.