Depressive Disorders Lecture Review
Epidemiology of Major Depressive Disorder (MDD)
Major Depressive Disorder is recognized as one of the most common psychiatric disorders.
Lifetime Prevalence: The lifetime prevalence is estimated at .
Average Onset: Typically occurs during late adolescence to early adulthood.
Gender Distribution: Women are affected twice as often as men, reflecting a ratio.
Course: The disorder is often recurrent.
Comorbidities: MDD is frequently comorbid with anxiety disorders and substance use disorders.
Depression vs Normal Sadness
Feature | Depression | Normal Sadness |
|---|---|---|
Duration | Lasts for weeks or months | Transient, resolves as life improves |
Intensity | Overwhelming and pervasive | Mild and manageable |
Impact on Functioning | Significant impairment in daily activities | No significant impairment |
Loss of Interest | Disinterest in previously enjoyed activities | May still engage in activities |
Physical Symptoms | Changes in appetite, sleep disturbances, fatigue | Typically none or mild physical symptoms |
Cognitive Symptoms | Severe issues with concentration and memory | Brooding thoughts, but less severe |
Suicidal Thoughts | May have thoughts of self-harm or suicide | absent |
Diagnosis Criteria | Symptoms must persist for at least two weeks | No diagnosis required; is a normal emotion |
MDD Prognosis and Recurrence
MDD is characterized by an extremely high rate of recurrence.
Early Recurrence: Following a single episode, the rate of recurrence over the next months is >40\%.
Long-term Recurrence: Within years, the rate of recurrence is >75\%.
Risk Factors: Incomplete remission of the initial episode is strongly associated with a higher risk of subsequent recurrence.
Etiology and Neurobiology of Depressive Disorders
Key Neurotransmitters:
Serotonin (): Influences mood, anxiety, sleep, appetite, and pain perception. Pathways originate in the raphe nuclei and project throughout the brain to regulate emotions.
Norepinephrine (): Influences alertness, energy, focus, and the stress response. Pathways originate in the locus coeruleus and project to the cortex to influence attention and motivation.
Dopamine (): Supports motivation, reward, pleasure, movement, and learning. Pathways originate in the ventral tegmental area () and substantia nigra, projecting to the limbic system and frontal cortex.
Additional Biological Factors:
Genetics.
Neuroinflammation.
Chronic stress.
Neuroplasticity changes.
Hypothalamic-Pituitary-Adrenal () axis dysfunction.
The Monoamine Hypothesis:
Theory: This theory suggests that a deficiency in monoamines (serotonin, norepinephrine, and dopamine) contributes directly to depression.
Mechanism: When monoamines are deficient, monoamine receptors upregulate.
Evidence: While direct evidence is lacking and the pathophysiology is recognized as a complex heterogeneous mix of inflammatory, excitotoxic, and endocrine factors, all available antidepressants act on the monoamine system.
Depression = "Bio + Psycho + Social"
Bio: Genes, neurotransmitters, cortisol
Psycho: Negative thoughts, helplessness
Social: Stress, trauma, isolation
Monoamine Hypothesis: ↓ Serotonin + ↓ Norepinephrine + ↓ Dopamine → Depressive symptoms.
Screening and Diagnosis of MDD
Diagnostic Tools: Clinical interviews, discussions with friends/family, laboratory work, review of prior treatment records, and the Patient Health Questionnaire ().
Screening Guidelines for Adults ( years): Annual screening is recommended using either the or .
Screening Guidelines for Adolescents: Annual screening starting at age using the (modified for ages ).
The PHQ-9 Questionnaire: Assesses symptoms over the past weeks:
Little interest or pleasure in doing things.
Feeling down, depressed, or hopeless.
Trouble falling/staying asleep or sleeping too much.
Feeling tired or having little energy.
Poor appetite or overeating.
Feeling bad about oneself or failing the family.
Trouble concentrating.
Psychomotor retardation or agitation (moving slowly or being fidgety).
Suicidal ideation or thoughts of self-harm.
PHQ-9 Scoring and Proposed Treatment:
: None-minimal severity; no treatment required.
: Mild severity; watchful waiting and repeat at follow-up.
: Moderate severity; treatment plan considering counseling, follow-up, and/or pharmacotherapy.
: Moderately severe severity; active treatment with pharmacotherapy and/or psychotherapy.
: Severe severity; immediate initiation of pharmacotherapy and expedited referral to a mental health specialist if impairment is severe.
Mimics of Depressive Disorders
Condition | Symptoms Similarity | Distinction |
|---|---|---|
Anxiety Disorders | Fatigue, irritability, concentration difficulties | Primary symptoms involve excessive worry or fear. |
Bipolar Disorder | Depressed episodes resemble major depressive disorder | Presence of manic or hypomanic episodes; more pronounced mood fluctuations. |
Adjustment Disorders with Depressed Mood | Low mood in response to identifiable stressors | Symptoms arise within three months of the stressor and are not as persistent or severe. |
Post-Traumatic Stress Disorder (PTSD) | Mood changes, irritability, concentration issues | Triggered by traumatic events; includes re-experiencing trauma and avoidance behavior. |
Schizophrenia or Schizoaffective Disorder | Depressive symptoms can be present alongside psychotic features | Involves hallucinations or delusions not present in depressive disorders. |
Thyroid Dysfunction (Hypothyroidism) | Fatigue, weight gain, depressive symptoms can appear | Will have physical manifestations and laboratory findings (e.g., abnormal thyroid hormone levels). |
Chronic Illnesses (e.g., cancer, heart disease) | Persistent fatigue, pain, emotional distress can mimic depression |
Anemia
Sleep Apnea
Vitamin Deficiency: Low levels of certain vitamins, such as B12 and D, can contribute to depressive symptoms and affect energy levels.
Chronic Illness
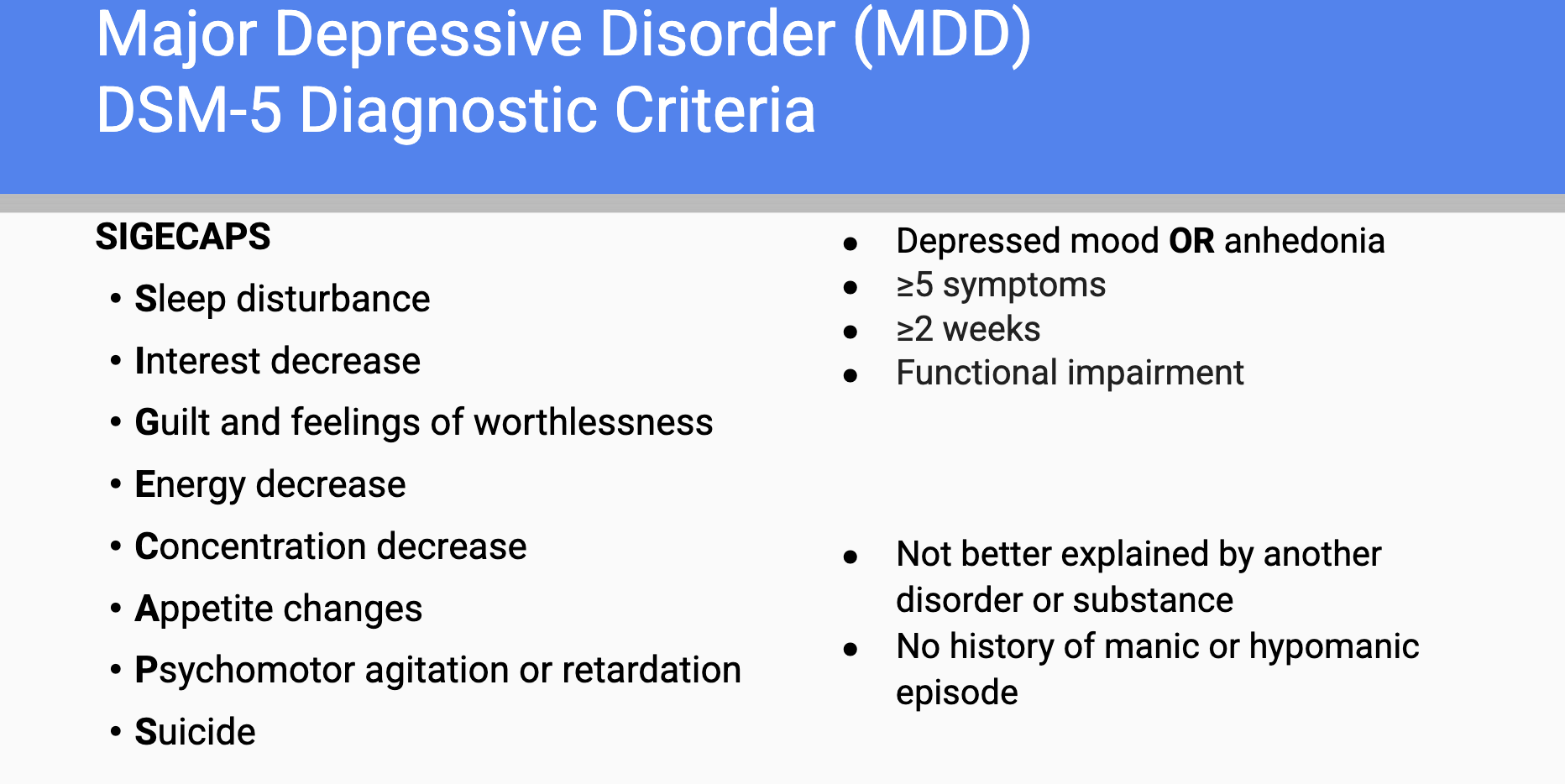
DSM 5 Criteria for Major Depression Disorder vs. Major Depressive Episode
Major Depressive Disorder: A persistent low mood lasting at least two weeks with symptoms affecting daily functioning, including loss of interest or pleasure, significant weight change, insomnia or hypersomnia, psychomotor agitation or retardation, fatigue, feelings of worthlessness or excessive guilt, difficulty concentrating, and recurrent thoughts of death. Patient have a history of at least 1 major depressive episode and there is no history of mania or hypomania.
Major Depressive Episode: A shorter duration diagnosis characterized by the same symptom criteria but does not necessarily recur, and can occur in the context of other mood disorders. It can occur in bipolar disorder, schizoaffective disorder and substance abuse depression.
MDD Clinical Specifiers
Specifiers are descriptive modifiers added to a diagnosis to describe the clinical presentation (e.g., Major Depressive Disorder, recurrent, severe, with anxious distress).
List of Specifiers:
With anxious distress.
With mixed features.
With melancholic features.
With atypical features.
With mood-congruent psychotic features.
With mood-incongruent psychotic features.
With catatonia.
With peripartum onset.
With seasonal pattern.
Peripartum Onset Specifier:
Affects of women during pregnancy or in the weeks/months following delivery.
of postpartum episodes actually begin prior to delivery.
Can be applied up until year postpartum.
Catatonia Specifier:
Characterized by mutism (no interaction), negativism (resistance to movement), posturing, waxy flexibility, and echolalia (repeating words).
Treatment: Lorazepam ().
Depressive Disorder Specifiers and Special Populations
DSM-5-TR allows clinicians to add specifiers to Major Depressive Disorder (MDD) to describe important symptom patterns, prognosis, and treatment considerations.
Specifier | Key Features | Clinical Pearls |
|---|---|---|
Peripartum Onset | Depression develops during pregnancy or within 4 weeks postpartum | Increased risk of maternal and infant complications |
Seasonal Pattern | Depressive episodes occur during a specific season (usually fall/winter) | Associated with reduced sunlight exposure |
Psychotic Features | Depression accompanied by delusions and/or hallucinations | Severe depression requiring urgent treatment |
Melancholic Features | Severe loss of pleasure and inability to feel better even with positive events | Often associated with biologic symptoms |
Atypical Features | Mood improves in response to positive events | Increased sleep and appetite are common |
Mixed Features | Depression with some symptoms of mania/hypomania | May indicate risk for bipolar disorder |
Remission and Severity Definitions
In Partial Remission: A period lasting less than months without significant symptoms following an episode.
In Full Remission: During the past months, no significant signs or symptoms of the disturbance were present ( months).
Severity Levels:
Mild: Symptoms are present but manageable, with only minor impairment in social/occupational functioning.
Moderate: Symptom count and intensity fall between mild and severe.
Severe: Numerous, unmanageable symptoms that markedly interfere with functioning.
Persistent Depressive Disorder (Dysthymia)
Diagnostic Criteria:
Depressed mood for most of the day, for more days than not, for at least years (at least year for children/adolescents).
During the -year period, the individual has never been without symptoms for more than months at a time.
Criteria for MDD may be present continuously for the years.
No history of manic or hypomanic episodes; criteria for cyclothymic disorder have never been met.
Comparison of MDD vs. PDD:
MDD: Episodic, lasts weeks, often more severe, may fully remit.
PDD: Chronic, lasts years, often milder, persistent symptoms.
MDD vs. Persistent Depressive Disorder vs. Premenstrual Dysphoric Disorder
Feature | Major Depressive Disorder (MDD) | Persistent Depressive Disorder (PDD/Dysthymia) | Premenstrual Dysphoric Disorder (PMDD) |
|---|---|---|---|
Definition | Episodic depressive disorder characterized by one or more major depressive episodes | Chronic, persistent depressed mood that is less severe but lasts much longer | Cyclical mood disorder related to the menstrual cycle |
Duration Requirement | At least 2 weeks | At least 2 years in adults (1 year in children/adolescents) | Symptoms occur during the final week before menses, improve within a few days after onset of menses, and become minimal after menstruation |
Core Mood Symptom | Depressed mood and/or anhedonia | Depressed mood most days, for most of the day | Marked mood changes associated with menstrual cycle |
Number of Symptoms Required | ≥ 5 of 9 depressive symptoms | Depressed mood plus ≥ 2 associated symptoms | ≥ 5 symptoms with at least one mood symptom |
Pattern of Symptoms | Distinct depressive episodes | Chronic, ongoing low mood | Cyclical and predictable with menstrual periods |
Mood Severity | Moderate to severe | Mild to moderate but persistent | Moderate to severe during luteal phase |
Anhedonia | Common | May occur | May occur |
Functional Impairment | Significant impairment during episodes | Chronic impairment over time | Significant impairment during symptomatic phase |
Periods Without Symptoms | May have complete remission between episodes | Symptoms never absent for >2 months at a time | Symptoms largely absent after menstruation |
Age of Onset | Any age, commonly late adolescence to early adulthood | Often begins in childhood, adolescence, or early adulthood | Reproductive-age females |
Relationship to Menstrual Cycle | None | None | Directly related to menstrual cycle |
Risk of Suicide | Increased | Increased, especially if MDD develops ("double depression") | Increased during symptomatic periods |
Treatment | Psychotherapy, antidepressants, lifestyle modifications | Psychotherapy, antidepressants, lifestyle modifications | SSRIs, hormonal therapy, CBT, lifestyle changes |
Suicide Risk Assessment and Safety Planning
Columbia Severity Suicide Rating Scale ():
Differentiates between active and passive suicidal ideation ().
Questions: Inquire about wishing to be dead, thoughts of killing oneself, methods, intention, and specific plans.
Evaluation: Assess onset, frequency, duration, prior attempts, and access to lethal means (guns, knives, medications).
Safety Plan Components:
Warning signs.
Coping strategies.
Support contacts.
Crisis numbers (e.g., Suicide & Crisis Lifeline).
Restricting lethal means.
Category | High-Yield Factors | Why It Matters |
|---|---|---|
Risk Factors | Previous suicide attempt, depression, bipolar disorder, substance use disorder, chronic medical illness, chronic pain, family history of suicide, social isolation, unemployment, financial stress | Increase the likelihood of suicidal thoughts, attempts, or completion |
Warning Signs (Acute Risk) | Suicidal ideation, specific suicide plan, intent to act, access to lethal means, giving away possessions, writing a suicide note, making final arrangements, increased substance use, social withdrawal, hopelessness, sudden calmness after severe depression | Suggest immediate or near-term suicide risk and require urgent assessment |
Protective Factors | Strong family/social support, access to mental health care, effective coping skills, religious/cultural beliefs discouraging suicide, future goals, responsibility to children/family, therapeutic alliance, treatment adherence | Reduce suicide risk and promote resilience |
Questions to Ask | "Are you thinking about suicide?" "Do you have a plan?" "Do you intend to act on it?" "Do you have access to the means?" "Have you attempted before?" "What keeps you from acting on these thoughts?" | Helps determine severity of risk and identify protective factors |
Low Risk | Passive thoughts only, no plan, no intent, strong protective factors | Usually manageable with close outpatient follow-up |
Moderate Risk | Suicidal ideation with some planning but limited intent or uncertain access to means | Requires urgent mental health evaluation and safety planning |
High Risk | Specific plan, intent, access to means, previous attempts, severe hopelessness | Requires immediate psychiatric intervention |
Imminent Risk | Active suicidal intent, lethal plan, available means, unable to contract for safety | Psychiatric emergency; hospitalization may be necessary |
Pearl | Importance |
|---|---|
Previous suicide attempt = strongest predictor of future suicide attempt/completion | Most commonly tested risk factor |
Hopelessness = strongest psychological predictor of suicide | Highly associated with suicide risk |
Plan + Intent + Means = High Risk | Indicates need for immediate intervention |
Protective factors lower but do not eliminate risk | Always assess both risk and protective factors |
Asking about suicide does NOT increase suicidal thoughts | Essential part of every depression evaluation |
Treatment Principles for MDD
Goals: Sustained remission (defined as PHQ-9 < 5) and improved social/occupational functioning.
Response: Defined as a reduction in symptom score of that remains above the remission threshold.
Settings: Use the least restrictive setting: Outpatient < Intensive Outpatient < Inpatient.
Treatment by Severity:
Mild: Psychotherapy first.
Moderate-Severe: Combination of medication and psychotherapy.
Severe/Suicidal/Psychotic: Urgent psychiatric intervention.
Prescribing Guidelines:
Choice is based on side effect profiles and comorbidities, as most antidepressants have similar efficacy.
"Start low and go slow."
Meds take weeks for full effect, though mild changes may be seen at weeks.
Black Box Warning: All antidepressants carry a warning for increased suicidal ideation in patients under years old.
Serotonin Syndrome
Definition: Life-threatening excess of serotonergic activity.
Classic Triad:
Mental status changes (agitation, confusion).
Autonomic instability (hypertension, tachycardia, hyperthermia, diaphoresis).
Neuromuscular hyperactivity (tremor, clonus, hyperreflexia, muscle rigidity).
SHIVERS Mnemonic: Shivering, Hyperreflexia/myoclonus, Increased temperature, Vital sign instability, Encephalopathy, Restlessness, Sweating.
Treatment: Stop all serotonergic agents, supportive care (IV fluids), sedation with benzodiazepines. Severe cases require cooling and Cyproheptadine.
TCA Overdose
TCA overdose is a medical emergency because it can rapidly cause life-threatening cardiac arrhythmias, seizures, and hypotension.
Tri-Cyclic Antidepressants (TCAs) can cause significant toxicity, presenting with anticholinergic symptoms, CNS depression, and cardiovascular complications.
Management includes ensuring a clear airway, providing IV fluids, administering activated charcoal if within 1 hour of ingestion, and cardiac monitoring.
Classic Clinical Presentation
"3 C's of TCA Toxicity"
Finding | Manifestation |
|---|---|
Cardiotoxicity | Wide QRS, arrhythmias, hypotension |
Coma | Altered mental status, CNS depression |
Convulsions | Seizures |
Discontinuation Syndrome
Advise patients to NEVER abruptly stop medications
Typically will taper off medications over several weeks or cross taper onto new medication
FINISH Acronym (Flu Like Symptoms, Insomnia, Nausea, Imbalance, Sensory Disturbances, and Hyperarousal)
Symptoms | Description |
|---|---|
Flu-like Symptoms | Fatigue, muscle aches, and chills. |
Gastrointestinal Distress | Nausea, vomiting, diarrhea. |
Neurological Symptoms | Dizziness, headaches, and sensory disturbances (e.g., brain zaps). |
Mood Changes | Increased anxiety, irritability, or depressive symptoms. |
Sleep Disturbances | Insomnia or vivid dreams. |
Timeframe | Symptoms typically begin within a few days of stopping the medication and may last for weeks. |
Management | - Gradual Tapering: Gradually reducing the dose under medical supervision to minimize withdrawal symptoms. |
Supportive Care: Providing supportive management through hydration, rest, and, if necessary, adjunctive medications to alleviate symptoms. | | Prevention | Gradual tapering of medications instead of stopping abruptly, particularly for those known to cause discontinuation syndrome.
Postpartum Depression Specific Treatments
Brexanolone (): Neuroactive steroid ( modulator). Administered as a -hour continuous IV infusion. Requires continuous pulse-ox monitoring due to risk of sudden loss of consciousness.
Zuranolone (): Oral version of brexanolone. Dose daily for days. Works quickly (approx. days). Cost is approximately for the course.
Non-Medication Treatments
CBT: Just as effective as antidepressants; best results when combined with medication.
Light Box Therapy: Used for Seasonal Affective Disorder. Intensity should be . Reduces melatonin production.
Electroconvulsive Therapy (ECT): Most effective treatment for depression. Induces a generalized seizure. Requires maintenance to prevent relapse.
Transcranial Magnetic Stimulation (TMS): Modulates cortical regions (left dorsolateral prefrontal cortex). Used for depression unresponsive to prior antidepressants.
Anti-Depressants & Special Patient Populations
Geriatrics
Category
Key Points
Prevalence of Depression in the Elderly
Depression is common among geriatric populations, often exacerbated by comorbid medical conditions, loss of loved ones, and social isolation.
Pharmacokinetics Changes
Aging affects drug metabolism, leading to altered pharmacokinetics. Drugs may have prolonged half-lives, increasing the risk for adverse effects.
Commonly Used Antidepressants
SSRIs (Selective Serotonin Reuptake Inhibitors): Generally preferred due to their favorable side effect profile, e.g., sertraline, escitalopram. Do NOT use Paroxetine!
Avoid using Bupropion if they have a history of seizures.
SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors): Can be effective but may cause increased blood pressure, e.g., venlafaxine.
Avoiding Tricyclic Antidepressants (TCAs): Due to anticholinergic effects which can lead to confusion, urinary retention, and cardiotoxicity.
Potential Side Effects
Increased risk of falls due to dizziness or sedation.
Monitor for hyponatremia (especially in SSRI use).
Watch for serotonin syndrome, especially when used with other serotonergic drugs.
Drug Interactions
Geriatric patients frequently take multiple medications, increasing the risk for drug-drug interactions. For instance, SSRIs can interact with anticoagulants, increasing bleeding risk.
Dosing Considerations
Start at lower doses and titrate slowly due to sensitivity in this population. “Start slow, go low”
Regular monitoring of renal
Pregnancy
Category
Key Points
Prevalence of Depression
Depression can occur during pregnancy and may affect about 10-20% of pregnant women.
Risks of Untreated Depression
Untreated depression during pregnancy is associated with complications such as preterm birth, low birth weight, and increased risk of postpartum depression.
Commonly Used Antidepressants
SSRIs (e.g., fluoxetine, sertraline) and SNRIs (e.g., venlafaxine) are often prescribed during pregnancy due to their safer profile compared to other medications. DO NOT prescribe Paroxetine and avoid SNRIs!
Potential Risks
Some studies suggest a small increased risk of congenital malformations, particularly with paroxetine. Long-term exposure has been associated with neonatal adaptation syndrome.
Monitoring
Close monitoring of maternal mental health and fetal development is essential, including risks and benefits of continuing or discontinuing medication during pregnancy.
Postpartum Considerations
Women with a history of depression are at higher risk for postpartum depression, requiring potential continuation of antidepressant therapy during the breastfeeding period.