chp 17
PERSONALITY DISORDERS
In general, personality disorders are configurations of traits considered “socially undesirable,” which means, very simply, that most people don’t like them. Patterns such as social awkwardness, suspiciousness, arrogance, whininess, and just plain strangeness, when taken to extremes, begin to shade into the range that might reasonably be characterized as a disorder. But it is difficult to specify the point beyond which normal variation in a personality trait becomes pathological. In fact, finding an exact point may well be impossible.
It is difficult to specify the point beyond which normal variation in a personality trait becomes pathological. In fact, finding an exact point may well be impossible.
But this ambiguity does not mean personality disorders are not real and important. They can create severe problems for the affected individual or others who know that person, and it is rather likely that you could name a few people to whom this applies. Indeed, one survey estimates that about 15 percent of all adult Americans have at least one personality disorder (B. F. Grant et al., 2004), and there is no reason to think that the prevalence varies much elsewhere in the world.
PERSONALITY DISORDERS
In general, personality disorders are configurations of traits considered “socially undesirable,” which means, very simply, that most people don’t like them. Patterns such as social awkwardness, suspiciousness, arrogance, whininess, and just plain strangeness, when taken to extremes, begin to shade into the range that might reasonably be characterized as a disorder. But it is difficult to specify the point beyond which normal variation in a personality trait becomes pathological. In fact, finding an exact point may well be impossible.
It is difficult to specify the point beyond which normal variation in a personality trait becomes pathological. In fact, finding an exact point may well be impossible.
But this ambiguity does not mean personality disorders are not real and important. They can create severe problems for the affected individual or others who know that person, and it is rather likely that you could name a few people to whom this applies. Indeed, one survey estimates that about 15 percent of all adult Americans have at least one personality disorder (B. F. Grant et al., 2004), and there is no reason to think that the prevalence varies much elsewhere in the world.
Basically, the battle was between an “old guard” of experienced clinicians who had become comfortable with a long-established standard list of disorders, and a more scientifically oriented group of mostly academic researchers who insisted on a classification system based on empirical data rather than clinical experience. The outcome finally published in the new, improved DSM-52 (American Psychiatric Association, 2013) was an uneasy compromise. The traditional system is still presented in the part of the manual that provides the definitive list of mental disorders. The new system appears, too, but in a separate section near the back of the book. The DSM-5 attempts to reconcile this inconsistency with the rather astonishing statement that “it is hoped that both versions will serve clinical practice and research initiatives, respectively” (p. 645). The word “respectively” seems to imply that clinical practice does not need to be scientifically based; I hope that isn’t really what the writers meant.
In any case, the long-term outcome seems clear. The new system will eventually completely replace the old, in the DSM-6 (whenever that appears) or maybe DSM-7. The old guard will die away sooner or later, as old guards inevitably do. For now, we are left in the awkward position of talking about personality disorders in two ways, (a) a time-honored, traditional way still followed by many clinical practitioners, and (b) a newer way that is more scientifically grounded. Although great efforts have been made to reconcile the two systems, as will be described later, we still have little choice but to consider both.
Purposes of the DSM
The succeeding editions of the DSM have two purposes. The first is to make psychological diagnosis more objective. Two clinical psychologists or psychiatrists cannot even talk about a client or a patient3, much less come to a mutual understanding, unless they have a common vocabulary. The hope of the DSM is that a specific list of criteria for diagnosis will make discussions and analysis clearer and more useful. This goal of objectivity is even more important for research. If a scientist believes that she has developed a promising treatment or a medication for a disorder, then there is no way to test the treatment or medication without some way to identify who has the disorder in the first place. The second purpose for the DSM may sound trivial, but it is not. The DSM gives the psychiatrist or clinical psychologist something to write on the insurance billing form! Go ahead and chuckle, but I am not joking. Insurance providers will not reimburse for the treatment of something that is not specified. Your primary care physician is not permitted to write on your chart that you came in because you were “sick.” A more descriptive label is required. So, too, if psychological treatment is going to be paid for—which is the same as saying, if it is to be offered at all—then categories of psychological disorders must be specified. The DSM can be and has been criticized on many grounds, but lack of comprehensiveness is not usually among them. The 943 pages of the DSM-IV-TR provided a label and a numerical code for a long list of just about everything that could conceivably go wrong with a person, psychologically speaking. I already mentioned that one goal of the revision was to streamline this list but the outcome was not especially successful. The DSM-5 is (exactly) 945 pages long. DEFINING PERSONALITY DISORDERS
The person who has a personality disorder may see it not as a disorder at all, but a basic part of who he or she is.
Personality disorders have five general characteristics. They are (1) unusual and, (2) by definition, tend to cause problems. In addition, most but not quite all personality disorders (3) affect social relations and (4) are stable over time. Finally, (5) in some cases, the person who has a personality disorder may see it not as a disorder at all, but a basic part of who he or she is.
Unusually Extreme and Problematic
The two defining features of personality disorders were described by the pioneering psychiatrist Kurt Schneider (1923). The first is that a person exhibits an unusually extreme degree of one or more attributes of personality. It is important that the variation be not only extreme but also unusual, particularly considering the individual’s cultural context. Thus, cutting somebody off in traffic on a Southern California freeway is an extreme behavior—it can be life-threatening for everyone involved—but it probably does not qualify as a symptom of personality disorder because it is (sadly) much too common. On a deeper level, clinical practice is just beginning to come to terms with the implications of cultural variation (see Chapter 13) for understanding abnormal psychology. Patterns of shy, self-effacing behavior (which is more the norm in interdependent or collectivistic cultures) or loud, aggressive behavior (which is more the norm in individualistic cultures) that otherwise could be viewed as symptoms of personality disorders might, in fact, be typical in context. Similarly, a parenting practice that is normal within one culture may seem harsh, and even draw the attention of the child protection authorities, if the neighbors notice it in a different cultural context. Recall the Danish mother, described in Chapter 13, who left her baby in a stroller parked outside a New York City restaurant and was arrested. Should she seek psychological treatment?4
As we saw in Chapter 10, Freud firmly believed that the extremes on any dimension are pathological and that sanity always lies somewhere in the middle. This idea may offer a way to separate out what is extreme in a pathological way from something that is extreme only in relation to the practices of a particular culture. Extremism requires the denial of reality. We see this frequently in politics, where in order to occupy an extreme position it is necessary to deny any possibility that people who disagree with you could possibly be correct in any way. Similarly, extreme styles of behavior may stem from denying the reality that some people are trustworthy, that other people are worthy of respect, or even that oneself is actually, potentially loveable. So perhaps we can revise this first criterion a bit, to recognize that the extreme behavior is a sign of disorder if it stems, on some level, from a denial or distortion of reality.
The second fundamental criterion for a personality disorder is that the associated extreme behavioral pattern causes major problems for the person or for others. A personality disorder typically—not always—causes some degree of suffering for the person who has it, which may include anxiety, depression, and confusion. But in the case of several disorders, many and perhaps most of the associated problems are suffered not so much by the affected person, but by those—such as spouses, employers, and (former) friends—who must deal with the results (Heim & Westen, 2005; Yudofsky, 2005). For example, an acquaintance with antisocial personality disorder may blithely steal your money, and while this is a problem for you, it is not really a problem for the acquaintance—unless he gets caught.Social, Stable, and Ego-Syntonic
How can you misperceive the intentions of a coconut?
Personality disorders have three other characteristics, which, although not as fundamental as the two just discussed, are generally viewed as part of the pattern. First, personality disorders are social; they manifest in interactions with other people. Alone on a desert island, it would be difficult to exhibit anything symptomatic of a personality disorder. After all, how can you be inflexible in your relations with a palm tree? How can you misperceive the intentions of a coconut? Other people are required for the full expression of many psychological symptoms.
Second, personality disorders are, by the usual definition, stable. They may first become visible in adolescence or even childhood and persist throughout life (DeClercq, 2018). Change can occur, but generally the time scale is years rather than weeks or months (Zanarini, 2008), and improvement, when it happens, is generally associated with increases in psychological maturity (Wright, Pincus, & Lenzenweger, 2011). Personality disorders are about as stable as personality itself which, as we saw in Chapter 7, is pretty stable (Durbin & Klein, 2006; Ferguson, 2010). This stability contrasts with more serious psychiatric disorders, which may come and go through acute phases and stages of remission much like other medical conditions. Less extreme maladaptive patterns of thought, feeling, and behavior that turn out to be temporary—the familiar combination of anxiety and hostility sometimes exhibited in adolescence, for example—also are generally not considered personality disorders. Because personality disorders are stable, they are (pretty much by definition) difficult to change through therapeutic intervention or any other means (Ferguson, 2010).
Third, and relatedly, personality disorders can be ego-syntonic, which means the people who have them do not think anything is wrong. People who suffer from other kinds of mental disorder generally experience their symptoms of confusion, depression, or anxiety as ego-dystonic afflictions of which they would like to be cured. For a surprising number of people with personality disorders, in contrast, their symptoms feel like normal and valued aspects of who they are, and they even may rate disorder-related traits as likable (Lamkin, Maples-Keller & Miller, 2018)!
Individuals with the attributes of the antisocial or narcissistic personality disorders, in particular, typically do not think they have a problem. They are more likely to see a disorder in the people who have problems with them. And the problems they cause for others may be as serious, or even more serious, than the problems they cause for themselves (Yudofsky, 2005).
This last characteristic implies, again, that therapists who treat personality disorders have a tough hill to climb. My university operates an assistance program that is intended, among other purposes, to help employees who have psychological problems that interfere with their work. When I was chair of my department, I went to a presentation by the director of this program. He begged any supervisor making a referral to please call him first and let him know why. He was having difficulties because employees would suddenly appear at his office. He would ask them what the problem was, and they would reply, “I don’t know; everything is fine; for some reason I was sent here.” Individuals with personality disorders say things like that surprisingly often, even while causing havoc for themselves and the people around them.
Glossary
ego-syntonic
Refers to thoughts, feelings, beliefs, or behaviors that one accepts as part of oneself and does not want to be cured of, even if others find them difficult to deal with.
ego-dystonic
Refers to troubling thoughts, feelings, beliefs, or behaviors that one experiences as alien or foreign and would like to be rid of.
THE MAJOR PERSONALITY DISORDERS
The traditional section of DSM-5 (like the previous DSM-IV) lists 10 major disorders that describe patterns of personality so extreme that they can cause serious problems. They are organized into three clusters that are named, not particularly helpfully, Clusters A, B, and C. Cluster A disorders are characterized by odd or eccentric patterns of thinking, including the schizotypal, schizoid, and paranoid personality disorders. Cluster B includes impulsive and erratic patterns of behavior, including the histrionic, narcissistic, antisocial, and borderline personality disorders. These are the disorders that tend to be most stable—that change the least—over time (Durbin & Klein, 2006). Finally, Cluster C comprises disorders characterized by anxious and avoidant emotional styles, including the dependent, avoidant, and obsessive-compulsive personality disorders.
A more useful way to think about personality disorders is in terms of the basic beliefs, attitudes and behaviors associated with each one. The pioneering psychologist Aaron Beck and his colleagues (Beck, Freeman, & Davis, 2004) view most of the disorders as characterized by (1) a fundamentally wrong idea that the person has somehow made the foundation of how he or she views the world, and (2) a strategy or style of behavior for dealing with the world that results from this wrong idea. For example, people suffering from dependent personality disorder hold the basic belief that “I am helpless” and as a result attempt to attach themselves to people they think will take care of them. Two of the disorders are explained a little differently because borderline personality disorder is characterized more by chaotic thinking than by any particular thought and, similarly, schizotypal disorder is associated with peculiar thinking in general rather than any specific idea. A summary of how this approach explains each of the 10 classic disorders is shown in Table 17.1. Cognitive-behavioral therapy is largely based on this system; its goal is to work with the client to change the mistaken core belief or thinking style and thereby improve the pattern of behavior that is causing so many problems.
In the newer, research-based section of the DSM-5, four of the classic disorders have been deleted, along with the clustering scheme. In the views of the researchers who prepared the new list, four previously listed disorders have not proved to be sufficiently coherent, common, or distinct from the other disorders to be useful diagnoses. These are (or were) the schizoid (asocial), histrionic (overly expressive), dependent (overly reliant on others), and paranoid (overly suspicious) personality disorders.
In the sections that follow, I summarize the six remaining disorders that survived this cut. But I still draw on their traditional descriptions, because they are not incompatible with the new descriptions and include more information and vivid detail. The chapter then summarizes the way in which personality disorders can be organized according to relevant personality traits, describes some of the changes in the new approach to psychological diagnosis, and, finally, concludes the discussion by considering the meaning and implications of labeling people with personality disorders.
Schizotypal Personality Disorder
Some people are idiosyncratic; they experience odd thoughts, have seemingly strange ideas, and behave unconventionally. They may have superstitious beliefs; they may actively avoid black cats or believe they have ESP or the ability to see the future. They may wear odd and unkempt clothing, and espouse unique ideologies or “theories of everything.” They may also experience discomfort in relating to other people—their odd actions might be somewhat off-putting, for one thing—and have particular difficulty in close relationships. None of these characteristics is especially rare and, taken one at a time, may not pose serious problems. But when the pattern becomes extreme, the individual may be characterized as having schizotypal personality disorder.
At its extreme, this disorder can dangerously approach schizophrenia, a serious psychotic condition characterized by major distortions of reality, jumbled thinking, and even hallucinations; indeed, some psychologists believe that schizotypal personality disorder should be grouped with it, rather than with the personality disorders.5 According to the DSM-5, schizotypal personality disorder has a prevalence ranging around the world from about 0.6 percent (in a Norwegian sample) to 3.9 percent or 4.6 percent (in two different U.S. surveys). The disorder appears to be slightly more common in men, and tends to be stable throughout life.
Narcissistic Personality Disorder
Narcissism is a special case of a personality trait that shades over into a personality disorder. We saw in Chapter 6 that while people high in this trait are sometimes annoying in the long run, they often make an excellent first impression and come across as extraverted, confident, and even charismatic. Indeed, their exaggerated self-esteem can, within limits, be useful (von Hippel & Trivers, 2011). The personality disorder goes beyond these limits and is much darker, associated not only with a wide range of exploitative and damaging behaviors, but also emotional instability and an unpleasant emotional life (J. D. Miller & Campbell, 2008).
The individual with narcissistic personality disorder (NPD) believes, sometimes against all evidence, that she is a superior being, and expects recognition for this, walking around all day with visions of unlimited wealth, absolute power, flawless beauty, or perfect love. She does not just expect the admiration of others; she needs it; so she may maneuver to evoke it. The tactics are not necessarily subtle. The narcissist may say things like, “Don’t you love my dress?” or “How about my great new car?” or simply brag about her accomplishments, wealth, friends, or appearance. She does not seem to have a clue about how obvious these contrivances generally are, and happily accepts the most transparent kinds of flattery. Tell the person with NPD that her clothes, car, accomplishments, or haircut are the greatest you have ever seen. She will agree; you will not be suspected of insincerity.
The person with NPD expects special treatment. Rules apply to other people, as does the need to stand in line, wait one’s turn, or be judged by consistent standards. Because of this sense of entitlement, he feels justified in taking advantage of others. After all, the purpose is merely to get what he deserves anyway. He may blithely lie, cheat, or simply leave the hard work to be done by other people. If your roommate has NPD, he will expect you to wash the dirty dishes. He has more important things to do. You don’t.
This exploitation is accompanied by a lack of empathy, because he is the only person on Earth who really matters. He assumes that everything about him must be of great interest, and may offer lengthy and inappropriately detailed monologues about his activities or feelings. At the same time, the person with NPD can be shockingly inconsiderate of the feelings of others.
People with NPD are not generally difficult to spot. Their arrogance gives them away. They belittle others and brag about themselves. They are rude to service people, seeming to revel in their small (and temporary) degree of social superiority over waiters and cashiers. They are boastful about small (or nonexistent) accomplishments, and sarcastic and condescending about the virtues or accomplishments of anybody else.
There is something pitiable about people with NPD and the related pattern of traits known as “entitlement” (Grubbs & Exline, 2016). Although they feel they are especially deserving of everything they want, this very feeling can make them vulnerable to disappointment, ego threat, and a sense that people aren’t treating them the way they deserve. This experience, in turn, can make them angry and emotionally upset.
But at the same time, people with NPD can be dangerous. The very characteristics that can make them attractive at first sight are the ones that cause the most problems in the long run6 (Back, Schmukle, & Egloff, 2010; Paulhus, 1998). As one experienced therapist writes,
Sadly, the combination of burning ambition and a willingness to distort the truth in people with narcissistic personality disorder can lead them to acquire substantial power and high position. These individuals harm many innocent people along the route to their personal aggrandizement. (Yudofsky, 2005, p. 126)
A fascinating, recently declassified psychological study of Adolf Hitler, commissioned by the OSS (the precursor to the CIA) during World War II and written by the pioneering personality psychologist Henry Murray (mentioned in Chapters 4 and 6), describes Hitler as a textbook case of narcissistic personality disorder. (Interestingly, this study was written before the formal identification of this disorder in the first DSM.) Apparently, being a narcissist is not a bar to becoming powerful, and other infamous figures such as Mussolini and Stalin have also been characterized by this syndrome. The sense of self-importance and lack of empathy, coupled with impressive political skills, seems to have made these individuals utterly ruthless—and successful—in their drive for power. The results were disastrous for everyone around them (and ultimately, in the cases of Hitler and Mussolini, for themselves).7
Narcissistic personality disorder is infamous among clinical psychologists for being difficult if not impossible to treat because, more than any other personality disorder, it’s ego-syntonic. People with NPD actually have some insight that they come across as arrogant and that people like them less over time (Carlson, Vazire, & Oltmanns, 2011); they still prefer to remain the way they are. Others may wish them to change; they have little or no desire to do so.
Estimates of the prevalence of this disorder are all over the map. The DSM-5 quotes a range somewhere between 0 percent of the population (which seems low to me) and 6.2 percent (which seems awfully high).Antisocial Personality Disorder
Some people are less honest than others, but when deceit and manipulation become core aspects of an individual’s way of dealing with the world, he may be diagnosed with antisocial personality disorder. This dangerous pattern includes behaviors such as vandalism, harassment, theft, and a wide variety of illegal activities such as burglary and drug dealing. People with this disorder are impulsive and engage in risky behaviors such as reckless driving, drug abuse, and dangerous sexual practices. They typically are irritable, aggressive, and irresponsible. The damage they do to others bothers them not one whit; they rationalize (see Chapter 10) that life is unfair; the world is full of suckers; and if you don’t take what you want whenever you can, then you are a sucker, too. Children unlucky enough to come under the care of someone with this disorder are at high risk for neglect or abuse. A wide variety of negative outcomes may accompany this disorder, including unemployment, divorce, drug addiction, imprisonment, murder, and suicide.
Antisocial personality disorder is sometimes confused with the trait of psychopathy, which was mentioned in Chapter 9 (Mealey, 1995), but it’s importantly different (Hare, 1996). Psychopaths are emotionally cold, they disregard social norms, and they are manipulative and often cunning. Most psychopaths meet the criteria for antisocial personality disorder, but the reverse is not true. Antisocial and even criminal behaviors have many sources; psychopathy is only one of them, in some people.When combined with psychopathy, antisocial personality disorder can be especially dangerous. Serial killer Ted Bundy used his clean-cut good looks and well-developed social skills, combined with a fake cast on his arm, to persuade young women near college campuses to help him load a sofa into his van. After his victim climbed inside he would slam the door and drive off to a secluded spot where he could abuse, torture, and eventually kill her. In general, people like this have an eye for people who are “nonsuspicious, kindly, and generous” (Yudofsky, 2005, p. 219), and are ruthless about exploiting them. It can be difficult to protect yourself from antisocial psychopaths, but one experienced therapist recommends that you “pay attention to your feelings,” especially feelings like “At first I felt uncomfortable, but I couldn’t quite figure out why” (Yudofsky, 2005, p. 220, italics in original). In other words, listen to your gut.
The DSM-5’s summary includes an interesting discussion of the apparent association of antisocial personality disorder with low economic status and urban settings—in other words, it’s largely (but not solely) a disorder of the poor and criminal. This observation raises several questions. Is it possible that, when separated from psychopathy, antisocial personality disorder merely describes a behavioral style that is adaptive or even necessary in certain settings? If so, should it still be considered a psychological disorder? Should a person with this disorder who commits a crime be considered not really a criminal but only ill? I will return to this issue near the end of the chapter, but this is a good time to begin thinking seriously about the disadvantages, as well as advantages, of having a psychological label for every pattern of socially undesirable behavior.
Estimates of the prevalence of this disorder range from 0.2 percent to 3.3 percent, and I sincerely hope the lower number is more accurate. By all accounts, antisocial personality disorder is much more common in men than in women.
Borderline Personality Disorder
From day to day with different people, and over time with the same people, most individuals feel and act pretty consistently. This fundamental fact was discussed in detail (and debated, to some extent) in Chapter 4. Predictability makes it possible to deal with others in a reasonable way, and gives each of us a sense of individual identity. But some people are less consistent than others, and have thoughts, emotions, and behaviors that are in flux and unpredictable even to them. When this pattern becomes extreme, a person may be diagnosed with borderline personality disorder, which is the most severe one on the list. It is characterized by unstable and confused behavior, a poor sense of identity, and patterns of self-harm that range from self-defeating behaviors to self-mutilation to suicide. Their chaotic thoughts, emotions, and behaviors make persons suffering from this disorder very difficult for others to “read”—they would be considered very low on the dimension of judgability considered in Chapter 5 (Flury, Ickes, & Schweinle, 2008).
Borderline personality disorder (BPD) entails so many problems for the affected person that nobody doubts that it is, at the very least, on the “borderline” with severe psychopathology.8 Its hallmark is emotional instability. The person’s mood can change rapidly from one moment to the next, and he may seem on the verge of going to pieces (Gunderson, 1984). The foundation of the disorder, according to some writers, is a sort of “emotional hemophilia,” in which a reaction, once stimulated, cannot be stanched—the individual emotionally “bleeds to death” (Kreisman & Straus, 1989, p. 8). Another prominent researcher writes that an individual with this disorder is “the psychological equivalent of [a] third-degree burn patient [with] . . . no emotional skin. Even the slightest touch or movement can cause immense suffering” (Linehan, 1993, p. 69).
According to the DSM-5, suicide attempts are common among people with BPD, and eventually 8 percent to 10 percent do kill themselves (American Psychiatric Association, 2013, p. 664). If this statistic is even close to correct, then BPD is a dangerous affliction indeed, comparable to the most threatening physical diseases. Even among nonsuicidal people with BPD, self-mutilation is common and may include compulsively “cutting”9 (with fingernails or knives) parts of the body including the hands, arms, and even genitals. The reasons for this behavior are far from clear; possibilities range from the rather psychoanalytic-sounding speculation that people with BPD feel guilty and are punishing themselves, to the idea that they are so emotionally disconnected that they must hurt themselves to know they are alive. It might also be a means of socially bonding with friends with similar disorders, communicating distress, or even demonstrating strength (especially in prison populations) (Hooley & Franklin, 2017). Perhaps the most plausible explanation comes from the description of the inner life of persons with this disorder as characterized by “emotional cascades,” which are “vicious cycles of intense rumination and negative affect” that lead to extreme suffering (Selby, Anestis, Bender, & Joiner, 2009, p. 375). Behaviors such as using fingernail clippers to pull off slices of skin (Cloud, 2008) may interrupt the process. Several studies support the conclusion that the main reason people engage in gruesome self-harm is “to alleviate negative emotions” (Klonsky, 2011, p. 1981; see also Klonsky & Muehlenkamp, 2007). Consider what this means: The feelings people with BPD are seeking to avoid must hurt even worse.A major and immediate challenge for a therapist working with someone suffering from BPD is to stop this cycle of self-harm. One suggestion—a serious suggestion!—is to teach patients other means of distraction from their emotional state, such as Sudoku. Other possibly useful therapeutic approaches include drawing the patient’s attention to the physical pain and social disapproval that results from cutting, and discouraging communities of BPD patients from communicating with each other about how and when they harm themselves (Hooley & Franklin, 2017).
Many people with BPD literally do not know who they are. They may have great difficulty understanding how they appear to others, and be confused about their values, career goals, and even sexual identity. They do not understand their own actions—cutters, for example, can say almost nothing meaningful about why they do it—and those with BPD may try to be social chameleons, avoiding behavioral choices and fading into the background by doing what everybody else seems to be doing. Recall from Chapter 15 that one function of the self is to provide a marker on an internal map that says “you are here.” People with BPD have lost the map.
The interpersonal relationships of people with BPD are confusing, chaotic, noisy, unpredictable, and unstable. In part, this is because they are prone to splitting, a term you may recall from object relations theory (described in Chapter 11) that refers to the tendency to view other people as either all good or all bad. Thus, a new relationship may be perceived as perfect, the best ever. Then, the first disappointment leads the person to conclude that the new partner is hopelessly thoughtless and cruel. These two extreme views, as Freud would have noted, have the same underlying dynamic. In both cases, the person with BPD is unable to handle the complex reality that people have a mix of good and bad characteristics, so she oversimplifies by jumping to one extreme evaluation or the other.
The pattern of emotion and behavior of someone with borderline personality disorder is to have no pattern.
All of the personality disorders are rather mixed bags of indicators, and BPD may be the most mixed of all. It is difficult to find a coherent, common thread among its characteristics, which may be why the label “borderline” is so descriptively unhelpful. Some psychologists, indeed, have suggested that this category is too diffuse and should be abandoned. But although other disorders were eliminated in the new system in the DSM-5, as we have seen, this one remains. The confusing and mixed-up nature of BPD may be the whole point. The pattern of emotion and behavior of someone with this disorder is to have no pattern. The personality itself is confused and disorganized, and the results can be disastrous and even fatal.
A huge amount of research attention has been paid to BPD in recent years, and some progress has been made. New theories have been proposed about its origins. One theory is that BPD arises when a genetic risk factor combines with an early family environment that fails to teach children how to understand and regulate their emotions. Children are put at risk when their “expressions of emotion are . . . rejected by the family and life’s problems are oversimplified” (Crowell, Beauchaine, & Linehan, 2009, p. 504). Another promising suggestion is that the disorder stems from problems with the endogenous opioid system, which regulates the body’s natural painkillers (the endorphins described in Chapter 8). “Frantic efforts to avoid abandonment, frequent and risky sexual contacts, and attention-seeking behavior”—all hallmarks of BPD—may be attempts to stimulate this system and thereby feel better (Bandelow, Schmahl, Falkai, & Wedekind, 2010, p. 623).
The most encouraging development is in therapies that might actually help. A technique called dialectical behavioral therapy (Linehan, 1993) teaches skills for emotional self-control. In individual and group sessions, the therapist and client closely examine past episodes of inappropriate emotional reactions and analyze how similar situations could be handled better next time. In a sense, it’s basic training in how to deal with emotions—a skill people with this disorder somehow never learned.
The DSM-5 estimates that about 2 percent of the population has this disorder, and about 75 percent of those diagnosed are women.Avoidant Personality Disorder
Everybody feels inadequate sometimes. Sometimes we do things we shouldn’t, sometimes we fail at what we attempt, and sometimes we are rejected. Moreover, none of these experiences is pleasant, and everybody seeks to avoid them. Fear of failure or rejection can lead to patterns of behavior such as shyness, and, in moderation, such patterns are both common and normal. When taken to an extreme, the result may be avoidant personality disorder. The fundamental problem experienced by individuals with this disorder is that their fear of failure, criticism, or rejection may lead them to avoid normal activities of school, work, and interactions with others. They expect the absolute worst: criticism, contempt, and rejection. They cannot join a group activity or have a relationship without constant reassurance that they will be uncritically accepted, and they may actively inhibit any emotional expression because they fear being mocked and rejected. As a result, others cannot get close to them, and their interpersonal world is constricted. It is safer to stay at home with the blinds pulled and the phone turned off.
This withdrawal from contact with others is very sad because, according to clinical psychologists who have studied people with this disorder, they really have deep cravings for affection and social acceptance, and they may spend much of their solitary time fantasizing about how much fun it would be to have friends or a lover. They may have trouble in their careers as well, because they try to avoid the meetings and social functions that are important for success in the business world.
A recent survey estimates that about 2.4 percent of the population suffer (and here the word suffer does seem appropriate) from this disorder, and its prevalence appears to be about the same in women as in men. In some people, the disorder may begin as severe shyness in childhood and gradually improve as they grow into later adulthood.
Obsessive-Compulsive Personality Disorder
It can be nice when the world is orderly and structured, and everybody follows the rules. Some people feel this need for order and structure more strongly than others (just peek into some of your professors’ offices if you want to see how widely this trait can vary). Within the normal range, being an orderly, structured person is generally a good thing, and this book relates many examples of the advantages of being highly conscientious, which (as we shall see later in this chapter) include good health and long life. But even this trait can go too far (Carter, Guan, Maples, Williamson, & Miller, 2015). The problematic extreme is called obsessive-compulsive personality disorder (OCPD). People with OCPD are bound by rituals and rules, can be severely judgmental of others, and are often miserly and stubborn. The individual who has OCPD resembles, in many ways, the type of person that Freud called the anal character (Chapter 10). Above all else, the person with OCPD lacks a sense of proportion, the big picture that allows one to judge when rules fail to apply to a given situation or when a particular detail just doesn’t matter very much.
People with OCPD are often stereotypical workaholics. They cannot take a weekend or even an evening off because they “have so much to do.” And yet, strangely, they seldom seem to get much done. It does seem that the amount of time people spend working correlates only loosely with how much they accomplish, and while people with OCPD may work long hours, they often don’t have much to show for it.People with OCPD may be compulsively unable to throw anything away, even things that have no possible use or sentimental value. They become anxious about discarding anything because they cannot escape feeling that they might need it someday, no matter how absurd the prospect is. There are famous cases of people with OCPD collecting huge piles of newspapers that fill their homes, unable to throw away even the sports section from 11 years ago, because they haven’t had a chance to read it yet.
This idea of the person with OCPD as a packrat is an interesting characteristic, in part because it seems to contradict some of the others, such as being compulsively neat and clean. This is where Freud comes in, though not through the pages of the DSM, which never mentions him, not in any of its editions. You may recall (from Chapter 10) that Freud believed opposites in character and behavior were always equivalent at a deep level, and the anal character is a good example. Anal characters might be compulsively neat or compulsively messy; the underlying dynamics in both cases are the same. The heaps of junk that fill the houses of some people with OCPD, and the sterile, bare, sparkling surfaces in the nearly empty houses of other people with OCPD may result from the same underlying psychological dynamics.
A major barrier to treatment is that, although people with OCPD are compulsively driven and may suffer from extreme anxiety if things do not go exactly their way, in some cases OCPD may be ego-syntonic. It is true that people with this disorder are—relatively speaking—less impaired in their daily functioning than are people with some of the other personality disorders (Skodol et al., 2002). Indeed, strange as it may sound, some people with OCPD claim they like being that way, and, to a degree, the traits associated with OCPD can be useful. There is something to be said for a surgeon, an accountant, or a data analyst who checks everything several times, whether it is really necessary or not. Certain kinds of mistakes become less likely. On the other hand, some of the compulsions that often go with OCPD—such as obsessive worrying about things that don’t really matter or are highly unlikely to happen, needing to turn back home several times to check whether the stove was left on, and bodily tics and habits such as compulsively picking at one’s scalp—are unpleasant symptoms most people would be happy to get rid of.
Indeed, OCPD is sometimes confused with the similarly labeled obsessive-compulsive disorder (OCD). OCD is a severe anxiety disorder characterized by compulsive behaviors that can range from repetitive hand-washing to bizarre rituals of speech or action (e.g., needing to touch every surface with which one comes into contact exactly 11 times before moving on). People suffering from OCD often have fearful obsessions and need the rituals to quell them. OCPD is different because it generally does not include such specific compulsions, but it can be more far-reaching because it may affect all areas of a person’s life. Interestingly, OCD may actually be more treatable than OCPD (Foa, 2004), in part because people with OCD generally are aware that their fears, unwanted thoughts and uncontrollable actions are unreasonable and would like to get rid of them, whereas people with OCPD are more likely to believe that “their way is the ‘right and best’ way” (Van Noppen, 2010, p. 1).
According to DSM-5, estimates of the prevalence of OCPD range from 2.1 percent to 7.9 percent, making it one of the more common personality disorders. Some studies suggest that antidepressant drugs such as fluoxetine and other specific serotonin reuptake inhibitors (SSRIs) of the sort discussed in Chapter 8 can effectively treat OCPD (Piccinelli, Pini, Bellantuono, & Wilkinson, 1995). This finding hints at the nature of OCPD and the degree to which it may be fundamentally driven by anxiety, depression, and general unhappiness.
Glossary
schizotypal personality disorder
An extreme pattern of odd beliefs and behaviors, and of difficulties relating to others.
narcissistic personality disorder
An extreme pattern of arrogant, exploitative behavior combined with a notable lack of empathy.
antisocial personality disorder
An extreme pattern of deceitful, manipulative, and sometimes dangerous behavior.
borderline personality disorder
An extreme and sometimes dangerous pattern of emotional instability, emotional emptiness, confused identity, and tendencies toward self-harm.
avoidant personality disorder
An extreme pattern of feelings of inadequacy accompanied by fear of social contact.
obsessive-compulsive personality disorder (OCPD)
An extreme pattern of rigidly conscientious behavior, including an anxious and inflexible adherence to rules and rituals, perfectionism, and a stubborn resistance to change.
ORGANIZING AND DIAGNOSING DISORDERS WITH THE DSM-5
The personality disorders just described appear in both the old and new approaches included in the DSM-5. However, an updated method for organizing the disorders has been added, and this new scheme is almost certainly the wave of the future. It varies from the traditional approach in a couple of major ways. First, the list of discrete disorders is shorter by almost half; as we have seen, the new list maintains only the antisocial, avoidant, borderline, narcissistic, obsessive-compulsive, and schizotypal disorders; everything else is categorized as a “personality disorder—trait specified.” But second and more importantly, it tries to move beyond placing disorders into discrete categories, such as the unhelpful “clusters” of the old version, and to instead recognize that psychological maladjustment is more a matter of degree than of kind (Clark & Watson, 1999a; Krueger & Eaton, 2010).
The Bad Five
The new system in the DSM-5 organizes personality disorders in terms of five major domains of traits that are more than reminiscent of the Big Five that we have seen many times in this book. They could be (but aren’t) called the “Bad Five.” Like the original Big Five, each of these trait domains also has facets that generally, but not always, go together (see Table 17.2). The traits are
Negative Affectivity, a tendency to feel negative emotions such as anxiety, depression, and suspicion
Detachment, a tendency to withdraw from and to avoid emotional contacts with other people
Antagonism, including deceitfulness, grandiosity, callousness, and manipulativeness; you may recognize some of the hallmarks of narcissism here.
Disinhibition, characterized by careless and impulsive behavior (the opposite of this trait, compulsivity, involves a kind of rigid overcontrol and perfectionism that can be almost equally maladaptive)
Psychoticism, a tendency to have bizarre thoughts or experiences, and to exhibit eccentric behavior
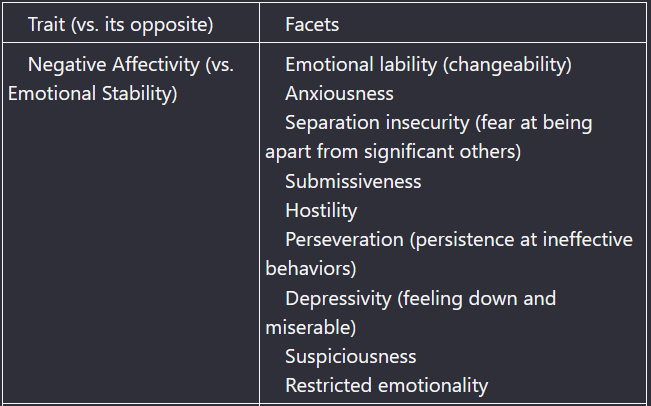
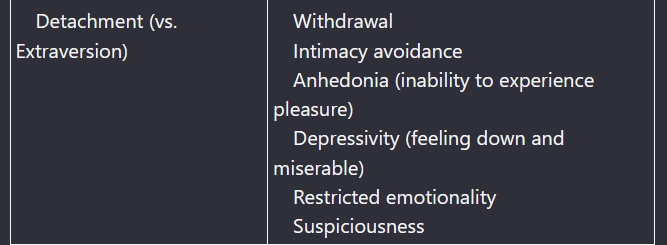
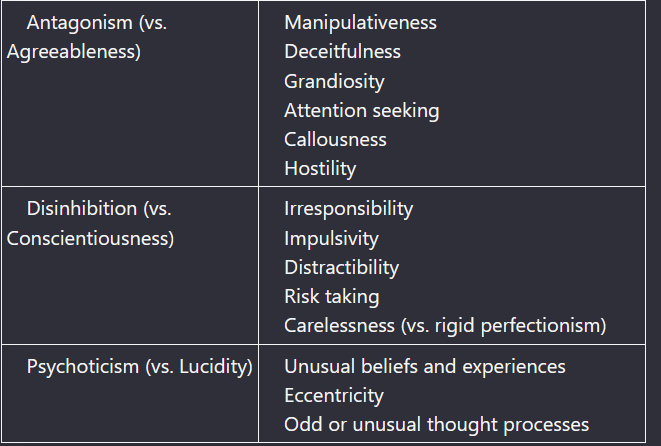 Notice how negative affectivity is akin to neuroticism in the Big Five; detachment is the extreme low end of extraversion; antagonism is the extreme low end of agreeableness; disinhibition is the extreme low end of conscientiousness; and psychoticism is the extreme high end of some aspects of openness to experience. This correspondence highlights the view, becoming ever more widespread in clinical and personality psychology, that the differences between normal and abnormal personality are not sharp or distinct, but lie along a continuum (further implications will be considered later in this chapter).
Notice how negative affectivity is akin to neuroticism in the Big Five; detachment is the extreme low end of extraversion; antagonism is the extreme low end of agreeableness; disinhibition is the extreme low end of conscientiousness; and psychoticism is the extreme high end of some aspects of openness to experience. This correspondence highlights the view, becoming ever more widespread in clinical and personality psychology, that the differences between normal and abnormal personality are not sharp or distinct, but lie along a continuum (further implications will be considered later in this chapter).
Diagnosis
The new section of the DSM-5 also describes a new way to go about psychological diagnosis. Rather than counting up the number of indicators that are present or absent and making a yes or no diagnostic decision, which was the old system, a clinical psychologist or psychiatrist is advised to take the following steps:
Assess whether or not the client’s “personality functioning” is seriously impaired and, if so, rate the degree of dysfunction.
Assess whether or not at least one of the six defined types of personality disorder is present.
Assess the degree to which the client is characterized by each of the five maladaptive personality traits.
This three-step assessment is intended to provide a specific description of the client’s psychological difficulty and the degree to which he is experiencing problems, but avoids sorting him into a single diagnostic bin. Clinical psychologists currently are hotly debating whether this will actually work in daily practice,10 and we probably won’t know until it begins to be tried on a large scale. Many front-line clinicians are already happy with the new system (Morey, Skodol, & Oldham, 2014). The U.S. government is definitely on the side of a more progressive approach. The National Institute of Mental Health, which funds a vast amount of research on psychopathology, has announced that new grant proposals should avoid the traditional categories and use a more dimensional approach, with a particular focus on biological aspects of mental disorder (Kruger, Hopwood, Wright, & Markson, 2014). Money talks, so this statement will be influential. Stay tuned.
Glossary
negative affectivity
One of five trait domains associated with personality disorders in the DSM-5, it is characterized by a tendency to feel negative emotions such as anxiety, depression and suspicion.
detachment
One of five trait domains associated with personality disorders in the DSM-5, it is characterized by a tendency to withdraw from and avoid emotional contacts with other people.
antagonism
One of five trait domains associated with personality disorders in the DSM-5, it is characterized by deceitfulness, grandiosity, callousness, and manipulativeness.
disinhibition
One of five trait domains associated with personality disorders in the DSM-5, it is characterized by a lack of self-control and impulsive behavior.
psychoticism
One of five trait domains associated with personality disorders in the DSM-5, it is characterized by a tendency to have bizarre thoughts or experiences, and to exhibit eccentric behavior.
PERSONALITY AND DISORDER
Amidst much debate, clinical psychology, psychiatry, and the successive editions of the DSM have displayed an increasing amount of insight and imagination as they formulate descriptions of many psychological disorders. This very success and the resulting proliferation of diagnoses raise issues concerning the pitfalls of describing so many behaviors as pathological, the nature of mental health, the pros and cons of labeling in general, and the fine line between normal and abnormal personality.
Pathologizing
Personality disorders describe bad ways to be. Does this mean that bad people have personality disorders, by definition? For example, some psychologists have proposed that “pathological bias,” such as extreme racism, homophobia, or other strong feelings about certain groups, should be defined as a personality disorder. One writer has noted that if this proposal succeeds, “perpetrators of hate crimes could become candidates for treatment, and physicians would become arbiters on how to distinguish ‘ordinary prejudice’ from pathological bias” (Vedantam, 2005, p. A01). Many personality disorders include patterns of socially undesirable, illegal, or immoral behavior. If certain people lie, cheat, steal, or even murder, should we refrain from punishing or perhaps even judging them because they suffer from antisocial personality disorder (which remains in the new system, by the way), and therefore are not accountable for those actions?
If you think I am going to answer this question, you are in for a disappointment. The issue is an eternal conundrum in the foggy area where psychology meets moral reasoning, and has been a long-standing dilemma in philosophy, religion, and law. No resolution is in sight. Some people are sure that the answer to this question is Yes, because it is absurd, pointless, and wrong to punish someone for having a psychological disorder. Others are sure the answer is No, because some behaviors should be punished regardless of their psychological (or even physical) cause. The truth, as always, lies somewhere in between—and, also as always, resists quick summary and easy understanding.
If everything is a mental illness, then nothing is a mental illness.
A further pitfall in pathologizing behaviors—describing them as the result of mental illness—is that it is entirely too easy. Critics of the old DSM-IV enjoyed pointing out that it included a label for everything from compulsive gambling to coffee nerves (Davis, 1997). It described so many behavioral patterns as forms of mental illness that it threatened to undermine the meaning of the concept altogether. If everything is a mental illness, then nothing is a mental illness.
Mental Health
No matter how long and detailed a list of disorders might be, it does not tell us much about the nature of mental health. This omission is precisely what motivates the positive psychology movement, focused on human strengths and virtues, that was discussed in Chapter 12. Positive psychology aims to move beyond an exclusive focus on fixing what’s wrong with people and instead promote meaningful and happy living. One way to define the healthy personality is in terms of the Big Five personality traits and their facets. In one large study, a group of experts agreed that the ideally psychologically healthy person has high levels of openness to feelings, positive emotions, and straightforwardness (non-pretentious and honest). At the same time, the ideally healthy person has low levels of depression and anxiety (neuroticism). In a sample of more than 3,000 individuals, people described in this way were found to be psychologically well-adjusted, optimistic, and self-controlled. They weren’t aggressive, mean, or exploitative, and they handled stress well (Bleidorn et al., 2019). This is useful to know, because improving mental health requires an understanding of normal and adaptive personality, not just mental illness and personality disorders.11
Labeling
Labels are always a little bit misleading, and sometimes they are seriously misleading. For example, it is important to avoid simply describing people we don’t like as having personality disorders, tempting though that may be. Such a description has a very good chance of being unfair. It can shut off rather than promote further understanding, because once a person has been labeled as mentally ill, we may no longer feel that we have to take seriously her feelings, outlook, and even rights, or to empathize with her point of view. A label is not an explanation, and the conclusion that someone has a personality disorder raises more questions than it answers.
On the other hand, the labels can be useful. If you come across someone who exhibits one or more of the characteristics of a personality disorder, it might be wise to consider whether he or she might show some of the other symptoms as well. For example, if someone acts in a grandiose and arrogant manner (a sign of narcissistic personality disorder), it might pay to be wary of the possibility he could seek to take advantage of you. If somebody gives signs of being just a little too impressed by the rule book and unable to adjust for the changing circumstances of real life (signs of obsessive-compulsive personality disorder), I would advise that you avoid at all costs putting her in charge of anything, or putting yourself in a position to take orders from her. And if someone you care about exhibits the emotional instability characteristic of borderline personality disorder, you might want to watch for indications that he might harm himself via drug addiction, eating disorders, cutting, or even suicide.
It might even be advisable to watch for signs of these disorders in yourself (although, as I discuss shortly, some of these attributes might sometimes be advantageous). If you catch yourself acting arrogantly, or following rules without regard to their purpose, or even harming yourself, this could be a warning to prevent further movement in a potentially dangerous direction. Thus, no matter how uncomfortable we may be about labeling people, it is still worthwhile to learn the basic characteristics of the major personality disorders (Yudofsky, 2005).
Finally, it must be acknowledged that, in the end, labels are absolutely necessary. There is simply no escaping them. When a psychiatrist or clinical psychologist records impressions of a patient, she must write something, so the more precise the labels, the better. Research, or even serious discussion, about mental illness would be completely impossible without words—labels—to refer to the different varieties that exist. Remember Funder’s Third Law (Chapter 2), that something usually beats nothing: No matter how flawed they may be—and they are flawed—the labels in the DSM-5 and its subsequent editions will persist until and unless something better comes along.Normal and Abnormal
Although the issue used to be highly controversial, the modern research literature on personality disorders has come close to consensus about one conclusion: There is no sharp dividing line between psychopathology and normal variation (Boudreaux, 2016; L. A. Clark & Watson, 1999a; Furr & Funder, 1998; Hong & Paunonen, 2011; Krueger & Eaton, 2010; Krueger & Tackett, 2003; B. P. O’Connor, 2002; Trull & Durrett, 2005). Normal personality traits are associated with a wide range of psychopathologies (Kotov et al., 2010), and the special tests designed to measure abnormal personality may do no better a job, for this purpose, than the instruments designed for the normal range, such as those surveyed in Chapter 3 (Walton, Roberts, Krueger, Blonigen, & Hicks, 2008). One recent study found that judgments of several personality disorder-related traits made by friends and acquaintances converged nicely with self-reports of the Big Five traits related to the same disorders, as well as with behavior observed directly in the laboratory (Kaurin, Sauerberger & Funder, 2018).
One implication of the continuum between normality and abnormality is that you may have recognized people you know, and even yourself, in parts of the descriptions of personality disorders. Your acquaintances, or even you, may indeed check the stove twice before leaving the house, experience deep hurt when other people don’t recognize an accomplishment, or have strange ideas sometimes. But it is important to remember that having a mild degree of a few characteristics does not imply that someone has a personality disorder.
Moreover, it is possible to think of each personality disorder as an exaggerated version of a trait that in the normal range can have some advantages (Oldham & Morris, 1995). For example, consider the person who is lovably unusual and idiosyncratic, has original, creative ideas, and generally marches to a different drummer: These fine tendencies overlap with elements of schizotypal personality disorder. An individual who is self-confident and proud has attributes that overlap with narcissistic personality, and so on.
An individual’s personality is a complete package that cannot be separated tidily into good and bad parts.12 Indeed, elements of some of the personality disorders may be cherished aspects of yourself! Remember Funder’s First Law (Chapter 1) about great strengths often being great weaknesses, and vice versa? Perhaps your creative spark and original outlook are among the best things about you; it’s just that occasionally this causes you to come off as a bit strange. Maybe you are valued for your perfectionism and attention to detail; only once in a while does this tendency go too far and annoy people. Your weaknesses may be part of your strengths; only when the characteristics are numerous, consistent, severe, and problematic should we speak about personality disorders.
There may be a little—just a little—of the personality disorders in all of us, and even people suffering from severe personality disorders probably have at least some sane, useful, and adaptive traits. This brings us back to the issue of normal behavioral variation and psychopathology. There is a difference, but the dividing line is neither sharp nor easy to find. PHYSICAL HEALTH
The implications of personality for physical health may be even more important than its implications for mental health. After all, nobody ever died of a personality disorder—at least, not directly. But several aspects of personality have important relationships with illness, with healthy functioning, and with that ultimate health outcome, longevity.
Connections between Personality and Health
It is harder to do good research on the connections between personality and health than it might seem at first. One challenge is gathering good data. While assessing personality is not so difficult, thanks to the well-developed technology of testing described in Chapter 3, assessing health is a different matter. Many studies use S-data measures in which people simply report how healthy they are or how good they feel. All the shortcomings of S data summarized in Chapter 2 apply. People may not really know or admit how healthy or unhealthy they are, or be unwilling to answer health questions truthfully on a questionnaire. Even worse, some of the questions on some personality tests also appear on health questionnaires! It is not uncommon to measure neuroticism, for example, with items such as “I feel bad all the time.” Items like this also show up on health questionnaires, so some studies showing neuroticism to be related to health have results that are questionable, at best (Friedman & Kern, 2014)An alternative, as we saw back in Chapter 2, is L data such as medical records. Some studies of personality and health use these records, but they are protected by layers of privacy laws and can be difficult to obtain. As a partial solution to this problem, at least one major study of personality and health focused on obtaining death certificates (Friedman & Martin, 2011). One nice thing about death certificates is that they are, in most jurisdictions, treated as public records. Another advantage is that death is an ultimate measure of physical well-being. As two experienced researchers noted, a person who has been issued a death certificate is, without question, “currently in terrible ‘health’” (Friedman & Kern, 2014, p. 721).
A person who has been issued a death certificate is, without question, currently in terrible “health.”
One recent research program combined a focus on longevity with personality assessments that moved beyond self-reports, being based on peer ratings. In other words (the words of the researchers), the study examined whether “your friends know how long you will live” (Jackson et al., 2015). It turns out they do, to some extent. Between 1935 and 1938, the study gathered friends’ ratings of the personalities of 600 people who were then in their mid-twenties, and checked to see who was still alive in 2013, more than 75 years later. The friends’ ratings predicted longevity better than self-ratings did. Men rated by their friends as more conscientious and open to experience tended to live longer, as did women who had been rated, years earlier, as more emotionally stable and agreeable.
These are interesting findings, but what do they mean? A further challenge is explaining the connections between personality and health that data like these reveal. Correlations between personality traits and self-reports of “feeling good” may reflect how personality affects mood rather than physical health. Correlations between personality traits and biomarkers, biological indicators related to health outcomes, may not actually reveal connections between personality and health. For example, personality traits have been related to cortisol levels (see Chapter 8), indicators of immune function, and vagal tone (a measure of activity of the parasympathetic nervous system; see Chapter 8), but the connections between these traits and actual health outcomes—such as functioning well in life and simply staying alive—are often less clear. Researchers have also found intriguing connections between personality traits and specific diseases, but these connections, too, are difficult to explain. For example, one major study found that in later life low conscientiousness was associated with a greater risk of stroke, high blood pressure, diabetes and arthritis; neuroticism was associated with lung disease, heart disease, and arthritis; and low openness was associated with stroke, heart disease, high blood pressure and arthritis (Weston, Hill, & Jackson, 2015). But why? It is undeniably important when personality traits turn out to predict how long a person lives and even specific diseases, but that does not mean it’s easy to figure out what’s going on.
At least two possible pathways between personality and health always need to be considered. One is biological: A personality trait may predispose an individual to certain physical reactions that have short- or long-term health consequences. For example, neuroticism may lead to repeated experiences of stress, which cause corticosteroids to be released into the bloodstream so often that there is excessive wear and tear on the heart. The other is behavioral: A personality trait may predispose an individual to certain behaviors that have health consequences. For example, a conscientious person may refrain from smoking, drive carefully, and even be careful to stay inside during thunderstorms (Friedman & Kern, 2014). All of these behaviors will make the person likely to stay healthier and live longer.
These are important points to keep in mind as we home in on the implications for health of three aspects of personality: The Type A personality, emotionality (negative and positive), and conscientiousness. The Type A Personality
The modern age of research on personality and health was initiated by a cardiologist named Meyer Friedman,13 who noticed that some of his heart patients seemed jittery, overreactive, and hyper-competitive. With colleague Ray Rosenman, he published a pioneering report claiming that blood and cardiovascular indications of risk for heart disease were correlated with a behavioral style of being obsessively ambitious to the point of being a “workaholic,” and sometimes hostile as well (Friedman & Rosenman, 1959). This person became labeled the Type A Personality said to be on the way to a heart attack—everyone else was a Type B. In later work, Friedman and Rosenman claimed that they could detect a Type A simply by listening to his14 speech patterns, which were described as loud, rapid, and “explosive” (Friedman, Brown, & Rosenman, 1969, p. 829).
However, the idea of the Type A personality has faded from prominence over the years. It turns out that there is little evidence that a behavioral style aimed at striving to achieve is associated with health risk; if anything, as we shall see below, the reverse seems to be true. Support for the idea that being Type A in any way causes heart disease is inconsistent at best (Kuper, Marmot, & Hemingway, 2002), and, to make things even more confusing, the two most widely used questionnaire measures of the syndrome (the Jenkins Activity Survey and the Framingham scale) don’t correlate very highly with each other and may even measure different traits (Langeluddecke & Tennant, 1986). It is also notable that findings have fluctuated over the years. Early studies tended to be supportive; later research was more discouraging. By the beginning of the 1990s, even advocates of the original concept noticed that more recent studies didn’t seem to be finding that Type A and heart disease were strongly related (Miller, Turner, Tindale, Posavac, & Dugoni, 1991). After that, research on Type A dropped off precipitously and eventually pretty much stopped altogether (see Figure 17.3).
There probably was a small kernel of truth in the Type A portrait, but it had nothing to do with ambition or hard work. Instead, it seems to have involved hostility.
There probably was a small kernel of truth in the Type A portrait, but it had nothing to do with ambition or hard work. Instead, it seems to have involved hostility (Williams, 2001). Early researchers who used an interview (rather than a questionnaire) to identify Type A individuals discovered that some interviewees were hostile to the whole idea of being interviewed. They answered questions sarcastically and made comments like, “I don’t have time for this” but such comments had more to do with irritability and impatience than with actually having a lot of work to do. People like that may indeed be at risk. The chronic experience of repeated hostile encounters can stress the physical system via corticosteroid response and other mechanisms, and the result over time can be both coronary disease and earlier mortality (Barefoot, Dahlstrom, & Williams, 1983). One study found that the experience of “cynical distrust”—of the sort exhibited by the people who didn’t like being interviewed—was associated with blood indicators of inflammation, which is a risk factor for atherosclerosis (Ranjit et al., 2007). So chronic hostility does appear to be bad for your health, while the other, more distinctive aspects of Type A—in particular, ambition and hard work—are not.
How did the idea of the Type A personality stay popular as long as it did? One astonishing reason may be that, for years, research on the topic was subsidized by the tobacco industry! According to a review of documents made available through settlement of a major court case,15 both the Philip Morris and R.J. Reynolds companies provided major funding for research on Type A (Petticrew, Lee, & McKee, 2012) and considered it a “crown jewel” of their efforts to convince people that smoking isn’t bad for you.16 The reason for their interest was that tobacco companies wanted to argue that smokers were likely to be Type A personalities, and so research on smoking and health had a “third variable problem” of the sort that was described in Chapter 2: It was smokers’ personalities, not their smoking, that led to their heart disease and early death. Through the 1960s and even into the 1970s some people thought this was a persuasive argument; almost needless to say, hardly anybody does anymore. Smoking really is bad for you. Count on it. But so is being angry all the time.
Emotionality
Research has addressed the relationship between both negative and positive emotions and health. “Negative emotionality”—the general tendency to experience negative feelings—is to some extent the reverse of extraversion, which you will recall from Chapter 6 is associated with the experience of positive emotions. Negative emotionality is also an important component of neuroticism. By any label, a vast amount of research shows that negative emotionality is associated with poor physical health. Indeed, one of the influences that led researchers to turn away from an emphasis on Type A and hyperactive overachieving was a classic paper that reported essentially the opposite result, that depression and withdrawal from life were risk factors for heart disease (Booth-Kewley & Friedman, 1987). Many related studies reporting similar findings followed, and the research topic grew into a popular sensation. Some prominent writers even claimed that watching funny movies or having a positive attitude can cure serious illnesses, including heart disease and even cancer (Cousins, 1979).
However, the idea that there is a direct connection between emotions and health may be one of those ideas that feels right, intuitively, but is mostly wrong. Much of the research suffers from the problem, noted earlier, in which self-reports of emotion overlap with self-reports of physical well-being. Studies also have reported contradictory results. One study of 997 Catholic priests, nuns, and brothers found neuroticism was associated with general poor health (e.g., Wilson, Mendes de Leon, Bienias, Evans, & Bennett, 2004). But another study of 597 Medicare participants between the ages of 66 and 102 found that neuroticism actually had a long-term positive relationship with health (Weiss & Costa, 2005). The reason for this latter finding, the researchers suggested, was that “impulsivity,” which is a facet of neuroticism, might actually be an indication of robust good health in older adults. On the other hand, the overall relationship between neuroticism and poor health, when it is found, may to a large degree be simply due to the fact that people high in this trait are more likely to be smokers (Mroczek, Spiro, & Turiano, 2009). But even that is not the whole story. Smokers who are high in “negative affect” are prone to contract lung cancer earlier in life (Augustine, Larsen, Walker, & Fisher, 2008).
An even more widespread complication in this research is that, to the extent there is a relationship between negative emotionality and poor health, either one may be the cause of the other. People who experience serious illness naturally feel negative emotions about this fact, and may indeed be physically suffering. One large study tried to disentangle the process by following a group of people over time and calculating cross-lagged correlations between emotional experience and health (Gana et al., 2013). A cross-lagged correlation looks at relationships between variables across time to assess whether changes in one variable precede or follow changes in the other. The results of their analysis showed that better health led to more positive emotional experience, and poor health led to negative emotions, but that no effect in the other direction could be found. According to this study, at least, while being sick leads to negative emotions, experiencing negative emotions does not necessarily make you sick. Other researchers noted the classic finding, mentioned above, that depression is associated with heart disease and so did a meta-analysis to review the evidence as to whether treating depression would improve heart health (Rutledge, Redwine, Linke, & Mills, 2013). The answer was mixed; mental health treatment appeared to lower CHD (coronary heart disease) “events,” but had no effect on the overall death rate.
The most important way that negative emotions are connected to physical health may be the way they affect behaviors that lead to stress. One large study of almost a thousand middle-aged residents of the St. Louis area found that people high on neuroticism (negative) emotionality were more likely to experience what the researchers called “dependent stress life events.” These are negative life events that occur at least in part because of the person’s own behavior, such as divorce, unemployment, and financial problems. The occurrence of such events was more common in people high in neuroticism, as well as people who were impulsive and disagreeable. And the experience of these events, in turn, was associated with the onset of new health problems (Iacovino, Bogdan, & Oltmanns, 2015). These results suggest that personality traits can lead to poor health indirectly, by influencing behaviors that lead to stressful outcomes, rather than by being direct causes of illness.
Through this behavioral route, neuroticism can sometimes actually be beneficial to health! According to one large study in the United Kingdom, people high in neuroticism actually lived somewhat longer, apparently because their tendency to worry and feel vulnerable led them to pay more attention to their health and to seek medical help more quickly (Gale et al., 2017). This positive effect of neuroticism might be particularly important in men, because neuroticism appears to decrease mortality risk in old age for men, even as it increases risk for women (Friedman, Kern & Reynolds, 2010).
What about positive emotions, such as optimism? While excess optimism can lead one to ignore health risks and take unwise chances, as we saw in Chapter 14, a certain amount of optimism can encourage healthy behaviors and enhance resilience in the face of difficulties (Carver, Scheier, & Segestrom, 2010). When faced with a health challenge, optimistic people seek more information and are more likely to do helpful things such as exercise and watch their diet, compared to pessimists. In other words, “people who expect good things to happen take active steps to make sure good things do happen” (Carver et al., 2010, p. 883).
It’s hard to imagine anything more frustrating and unfair than suffering from a serious disease, and being told you would be healthier if you would just cheer up.
Overall, the relationship between emotionality and health is complicated. Some aspects of negative emotion probably just exacerbate feelings that are bad already; other aspects can serve as a warning that motivates a person to change her behavior or avoid risks. When it comes to positive emotions, popular claims that simply having an upbeat attitude can improve health are (sadly) false (Coyne & Tennen, 2010). Such claims are also potentially dangerous, because they sometimes come close to blaming victims of disease for their fate (Friedman & Kern, 2014). It’s hard to imagine anything much more frustrating and unfair than suffering from a serious disease, and then being told you could become healthier if you would just cheer up. Needless to say (I hope), it’s not nearly that simple.
To the extent that positive emotions have an effect, it is probably that they motivate people to seek information and change their behaviors in beneficial ways. Other conclusions are harder to draw. The many possible pathways between emotions and health remain open for exploration.Conscientiousness
Fortunately, the relationship between one personality trait and health is crystal-clear. Conscientiousness is good for you. It really is. Highly conscientious people don’t just live longer, as was noted in Chapters 4 and 6; they also enjoy a whole range of positive outcomes that include quality as well as length of life. One reason for the relationship to health is that highly conscientious people may handle stress better; specifically, they react less strongly and less negatively to the difficult challenges of daily life (Leger et al., 2016, see Figure 17.4).Highly conscientious people don’t just live longer; they also enjoy a whole range of positive outcomes that include quality as well as length of life.
Another reason for the connection between conscientiousness and health is that people high on this trait do things every day that make good health more likely. A recent meta-analysis summarized studies that, in total, looked at 76,150 participants, 3,947 of whom had died (Jokela et al., 2013). Conscientiousness was the only trait that consistently identified who would live rather than die during the period of the study. The reason seemed to be that people low in that trait exhibited low persistence, poor self-control, and a lack of long-term planning to do things to protect their health. By contrast, according to another study, people high in conscientiousness are less likely to be smokers, heavy drinkers, or obese (Turiano, Chapman, Gruenewald, & Mroczek, 2015). Similarly, an Internet survey with 460,172 respondents found that people lower in conscientiousness had poorer (self-reported) health, higher body-mass index (BMI, a measure of unhealthy vs. healthy weight), and more substance abuse (Atherton, Robins, Rentfrow, & Lamb, 2014).
Not all of the health-promoting behavioral patterns associated with conscientiousness are directly related to health. For example, being unemployed is bad for your health, in part because it may lead to lack of access to health care, poor nutrition, or even homelessness. Even in the short term, losing a job can cause stress that leads to adverse health consequences if the individual does not find reemployment within a year (Strully, 2009). But, statistically speaking, conscientious people are relatively likely to be employed and unlikely to be fired, as was summarized in Chapter 16. Thus, the employment-related behavioral styles associated with conscientiousness have consequences for health.
Notice how the lessons from research on conscientiousness, like the research on depression, are almost exactly opposite those initially drawn from studies of the Type A personality. The original Type A stereotype nearly seemed to imply that hard work is bad and ambition, dangerous. But research has repeatedly shown not only that occupational success and striving are related to health, but also that people who stay active into old age live the longest. Indeed, some studies show that early retirement may make early death more likely, even if the researcher adjusts for the possibility that people who are unhealthy seek to quit their jobs earlier (Bamia, Trichopoulou, & Trichopoulos, 2008; Carlsson, Andersson, Michaëlson, Vågerö, & Ahlbom, 2012). So the best advice for a ripe old age just might be: Keep working, especially if you can find something enjoyable and creative to do (Turiano, Spiro, & Mroczek, 2012).Prospects for Improving Health
Many prescriptions for improving health through psychological means have focused on changing personality. If we could just make people less anxiously driven, more emotionally positive, and more conscientious, perhaps we could make them healthier. Although seeking to strive less in life turns out likely to be bad medicine, increases in positive emotionality and conscientiousness might be helpful, although far from easy to accomplish. As we saw in Chapter 7, this kind of personality change might be possible, but it is certainly not easy.
Until we figure out how to change major traits of personality, more direct routes for improving health, informed by psychological research, remain highly feasible. For example, one study provided strong evidence that an important reason that conscientious people live longer is simply that that they smoke less. This finding implies it might be more practical to focus interventions on stopping smoking than on increasing conscientiousness, per se. The other health-enhancing behaviors associated with conscientiousness also offer promising targets for intervention, ranging from improving habits such as exercise, to promoting engagement in work and being active and productive into old age. Of course, if we really could do something effective to increase conscientiousness, we might, just might, be able to affect all of these behaviors at once. That would be awesome.THE HEALTHY PERSONALITY
The ideal “healthy personality” has two aspects. One concerns mental health, and the other concerns physical health. The new, improved section of the DSM-5 defines the psychologically “optimally functioning individual” as someone who
. . . has a complex, fully elaborated, and well-integrated psychological world that includes a mostly positive, volitional, and adaptive self-concept; a rich, broad, and appropriately regulated emotional life; and the capacity to behave as a productive member of society with reciprocal and fulfilling interpersonal relationships.” (American Psychiatric Association, 2013, p. 771).
On the physical side of things, researchers Howard Friedman and Margaret Kern (2014) list six indicators of health that include
Having the ability to do the things one wants to do
Feeling good
Having supportive social relationships and being able to support others
Being productive and getting things done
Having good memory capacity and being able to make good decisions
Staying alive
Both of these definitions are pretty good, but you may recall that Sigmund Freud said essentially the same thing in fewer words. Health, he said, is the ability to love and to work.
SUMMARY
People are different, and these differences have important implications for mental and physical health.
Personality Disorders
Personality disorders are configurations of traits that cause serious problems for the people who have them and the others who must deal with those people.
The Diagnostic and Statistical Manual (DSM)
The Diagnostic and Statistical Manual of the American Psychiatric Association describes a wide variety of mental problems, including personality disorders.
The new edition of the Manual, DSM-5, includes both an older, traditional and a new, more scientific approach to the personality disorders.
The purposes of every edition of the DSM have been to make psychological diagnosis more objective and to provide useful categories for various purposes ranging from scientific research to billing.
Defining Personality Disorders
All personality disorders have two essential characteristics: (1) They are unusually extreme in a way that generally entails a distortion of reality, and (2) they cause problems for the self or others.
Most, if not all, personality disorders are also social and stable. In addition, some disorders are ego-syntonic, which means they are not experienced as problems by the people diagnosed with the disorder.
The Major Personality Disorders
The traditional section of the DSM-5 lists 10 major personality disorders divided into three categories: Cluster A, the odd/eccentric disorders, include schizotypal, schizoid, and paranoid personality disorder. Cluster B, the impulsive/erratic disorders, include histrionic, narcissistic, antisocial, and borderline personality disorders. Cluster C, the anxious/avoidant disorders, include dependent, avoidant, and obsessive-compulsive personality disorders.
A useful system used by Aaron Beck and his colleagues conceptualizes personality disorders as incorrect beliefs or problematic ways of thinking which result in maladaptive patterns of behavior.
The new section of the DSM-5 retains only six disorders as having a sound scientific basis; the schizoid, histrionic, dependent, and paranoid disorders have been removed from the list. The ones retained are the schizotypal, narcissistic, antisocial, borderline, avoidant, and obsessive-compulsive personality disorders.
Organizing and Diagnosing Disorders with the DSM-5
The new approach of the DSM-5 not only reduces the list of disorders to six, it also moves away from discrete categories of disorders to describing them along continuous trait dimensions.
The “Bad Five” personality traits of the new DSM-5, analogous to the Big Five traits for describing normal personality, are negative affectivity, detachment, antagonism, disinhibition, and psychoticism.
The three steps to diagnosis of personality disorder are (1) assess the degree of the client’s function, (2) assess whether one of the six recognized disorders is present, and (3) assess the degree to which the client is characterized by each of the “Bad Five.”
Personality and Disorder
Pathologizing undesirable behavior can raise difficult moral issues, and also risks describing so many patterns as mental illnesses that the concept of illness begins to lose its meaning.
A list of psychological disorders does not imply a definition of mental health.
Labeling disorders carries serious risks, but also has helpful applications and may be inevitable.
The line between normal personality variation and personality disorder is fine and uncertain. Indeed, some personality disorders can be seen as exaggerations of traits that, in moderation, are desirable.
Physical Health
CONNECTIONS BETWEEN PERSONALITY AND HEALTH
Personality has important implications for physical as well as mental health.
Much research on personality and health uses self-report (S data) to measure both personality and health outcomes, which can make results difficult to interpret.
L data used in research on personality and health can include medical records and even death certificates.
Personality may have direct, biological associations with health, but a more important pathway is probably the way personality affects behaviors that affect health, such as smoking.
THE TYPE A PERSONALITY
Early research on personality and health identified Type A personality as a pattern of nervous and compulsive seeking for achievement, combined with hostility, that promoted heart disease.
Later research has tended to disconfirm early indications that Type A behaviors are unhealthy overall, and research on the topic has nearly stopped. However, chronic hostility does appear to have negative health consequences.
EMOTIONALITY
Negative emotions may be a consequence as much or more than a cause of poor health, and in some cases can actually motivate people to monitor and protect their health more carefully.
Positive emotions such as optimism do not lead directly to better health, but may help a person to seek information and change behavior in beneficial ways.
CONSCIENTIOUSNESS
The evidence about conscientiousness and health is clear. More conscientious people tend to be healthier and live longer, mostly because they perform behaviors that promote their health (e.g., drive carefully, stop smoking) and because their overall success at life promotes a healthy environment.
PROSPECTS FOR IMPROVING HEALTH
Although there is some indication that changing personality to improve health might be possible, in the short run a more promising route to improving health may be to target the behaviors that promote and harm health that personality research has identified.
The Healthy Personality
The healthy personality, both mentally and physically, belongs to someone who is capable of love and work.