Blood Lecture 3.01.docx
Components of Blood
- Plasma 55%
- 45% Red blood cells
- <1% White blood cells and platelets
“Buffy coat”
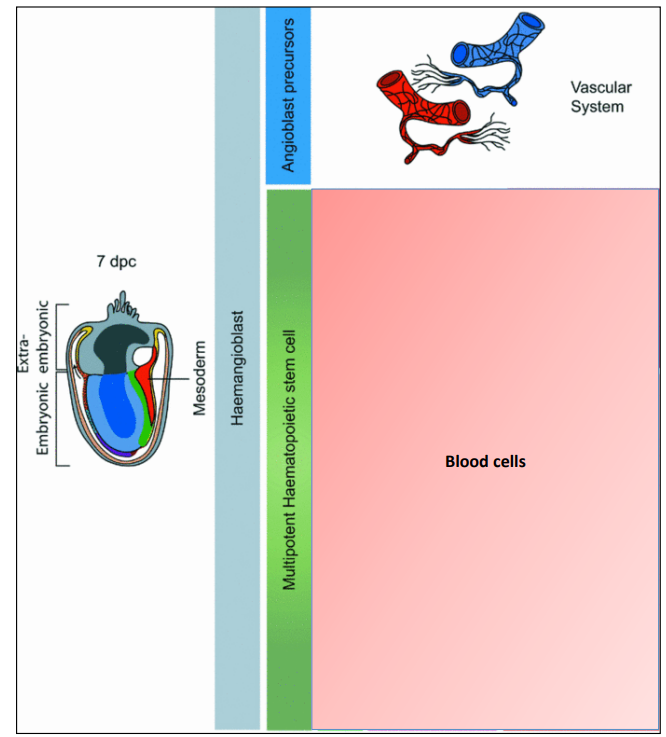
At a day 7 embryo stage, they have very few cells. There is one cell that forms – a stem cell. A stem cells that have the capacity to self-renew and are multipotent (give rise to multiple tissues).
This is fundamental to human embryology.
At the 7 day embryo stage, there is a single cell that is formed which is called a haemangioblast which gives rise to the entire vascular system including the heart, arteries and veins and other blood cells. It divides to form an angioblast – the first blood stem cell.
100-1,000 stem cells to keep us going for a life time as an estimate.
Stem cells reside in bone marrow.
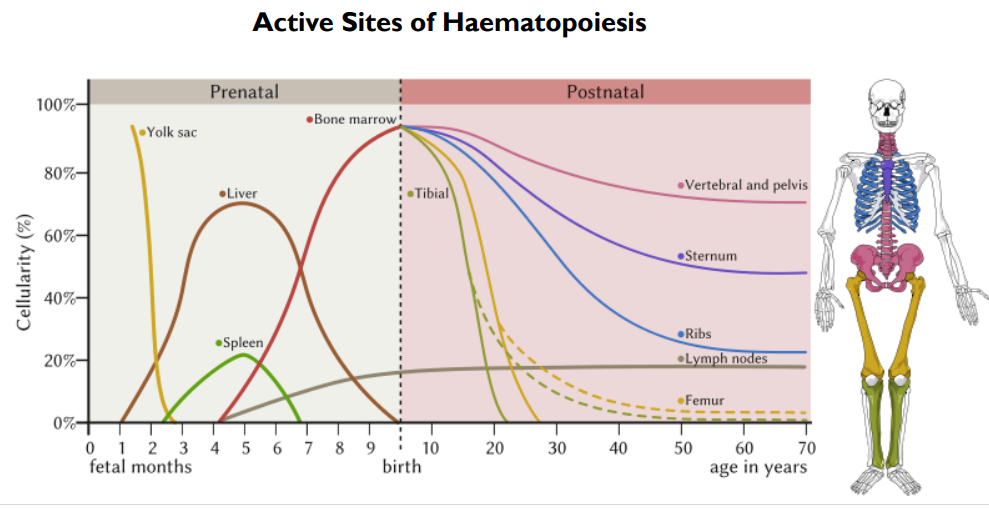
Most of the blood is produced in the yolk sac.
By 3 months foetal, this switches to the liver and spleen. Then again to the lymph nodes.
Bone marrow takes over by birth.
There is a lag period before it begins in the bone marrow due to everything being cartilage at this stage.
All bone have bone marrow at birth but this decreases with age to just the pelvis, sternum and spine.
Haematopoiesis
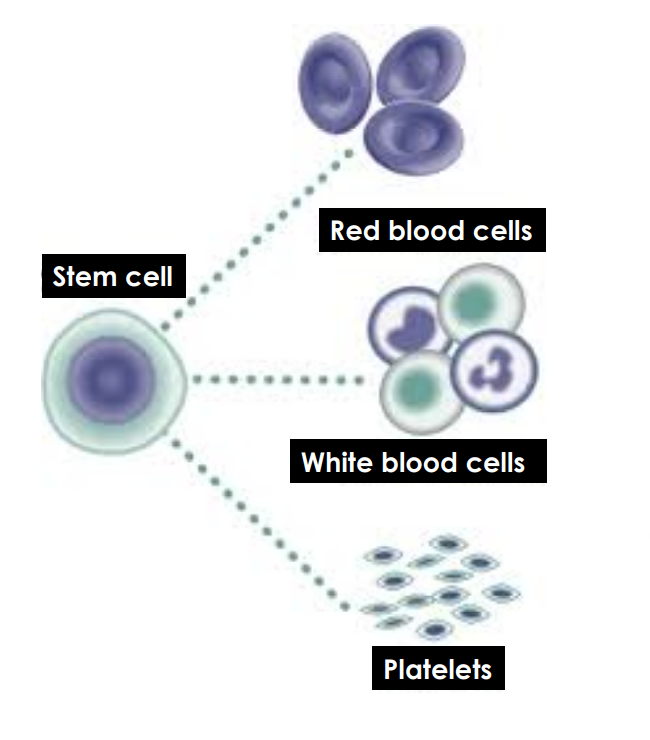
From the single stem cell, there are 3 types of cell produced (red cells, white cells and platelets)
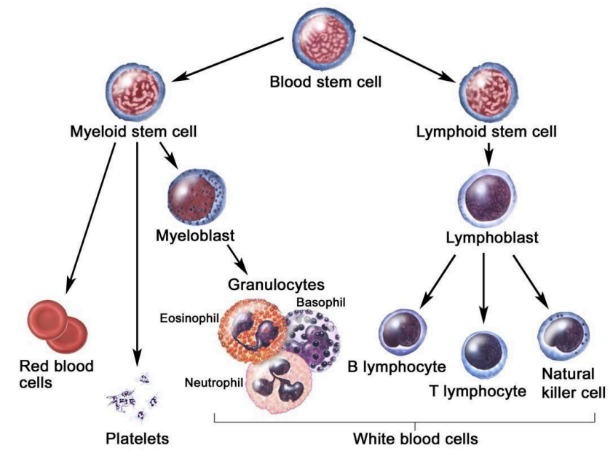
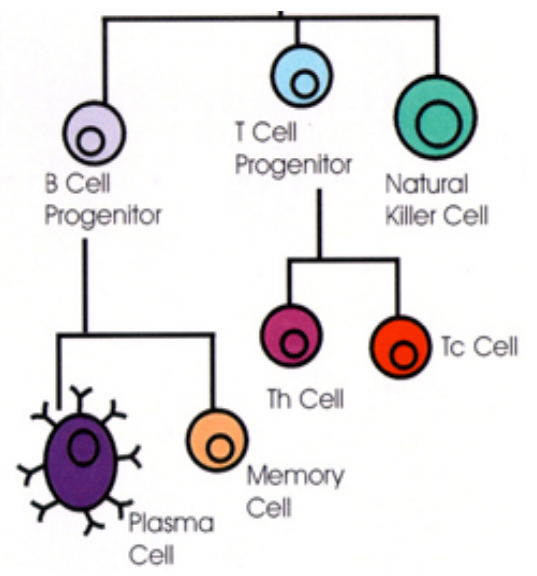
The stem cell has binary choice. The first choice it makes is to decide whether its going to become a myeloid stem cell or a lymphoid stem cell. The myeloid stem cell gives rise to red blood cells, platelets and all the white blood cells called granulocytes. The lymphoid stem cell is responsible for producing B cells, T cells and natural killer cells which are completely responsible for our immune systems.
White cells (leucocytes)
3 main types: neutrophils, eosinophils and basophils. Some are called granulocytes because they have granules in them. Monocytes and lymphocytes are also formed. Erythrocytes and platelets are not white cells.
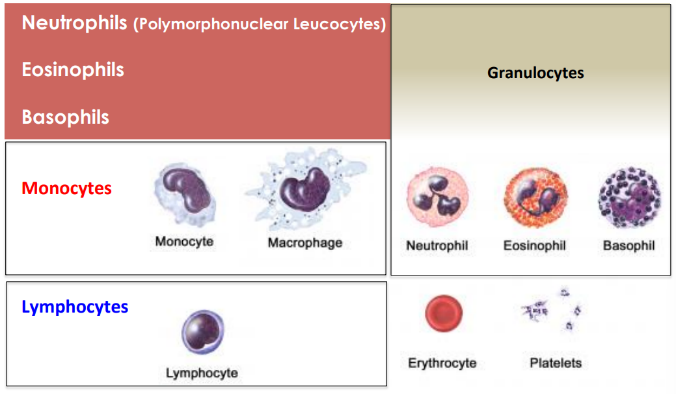
Lymphocytes
Structure – cells of the immune system
Mainly of the B cell, T cell and Natural killer cell types. The B cells differentiate to produce plasma and memory cells when they encounter any type of antigen. Plasma cells are responsible for producing antibodies aka immunoglobulins.
There are 5 types of immunoglobulins (G,A,M,E and D)
Leucocytes
Decrease is leucopenia
Increase is leucocytosis
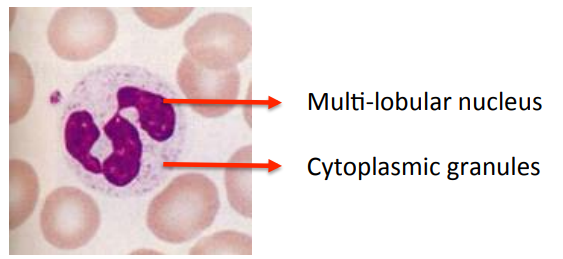
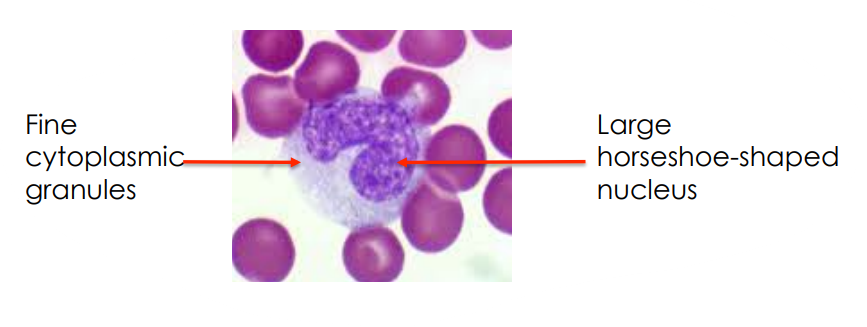
Neutrophils
Structure:
Function:
•Short-lived, motile cell designed to phagocytose bacteria and combat tissue infection.
•Multi-lobed nucleus allows extreme deformability (extravasation between endothelial cells - Margination).
•Neutrophils engulf bacteria to form a phagocytic vacuole. The cytoplasmic granules fuse with the phagocytic vacuole deliver bactericidal products.
Quantitative Abnormalities:
- Neutrophil leucocytosis (neutrophilia)
- Bacterial infections
- Inflammation
- Acute Stress
- Neutropenia
- Bone Marrow failure
- Hypersplenism
- Abnormal margination
Qualitative Abnormalities
- Myelodysplastic Syndrome (MDS)
- Rare hereditary defects (e.g. chronic granulomatous disease)
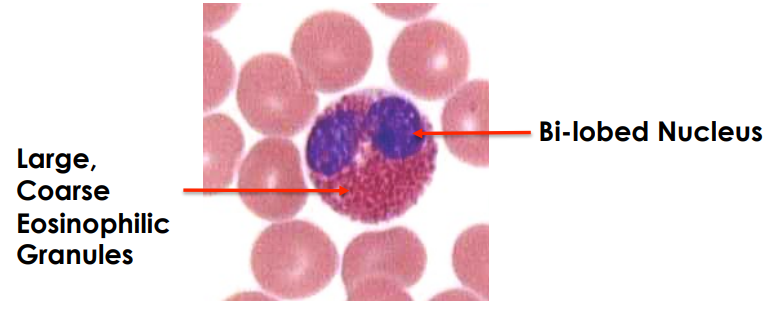
Eosinophils
Structure:
Function:
Short-lived motile cell concerned with certain allergic phenomena and immunity to helminths.
Quantitative Abnormalities:
- Increased Eosinophilia
- Allergies e.g. Asthma
- Helminthic infections
- Hyper-eosinophilic syndrome
- Hodgkin’s Lymphoma
Eosinopenia and qualitative abnormalities not important
Basophils
Structure:
- Nucleus not obviously multi-lobed.
- Cytoplasm packed with basophilic granules.
Function:
- Concerned with immune phenomena (IgE mediated).
Quantitative Defects
- Basophilia – Myeloproliferative disorders.
- Qualitative defects and decreased basophils not important.
Monocytes/Macrophages
Structure:
Function:
- Monocytes are maturing cells on their way from bone marrow to tissues where they form macrophages.
- Macrophages function as long-lived tissue phagocytes associated with chronic inflammation and chronic infections.
Monocytes
Quantitative Abnormalities:
- Monocytosis
- Marked Monocytosis
- Chronic Leukaemia
- Acute Leukaemia
Monocytopenia and Qualitative Abnormalities
- Not important
Lymphocytes
Function:
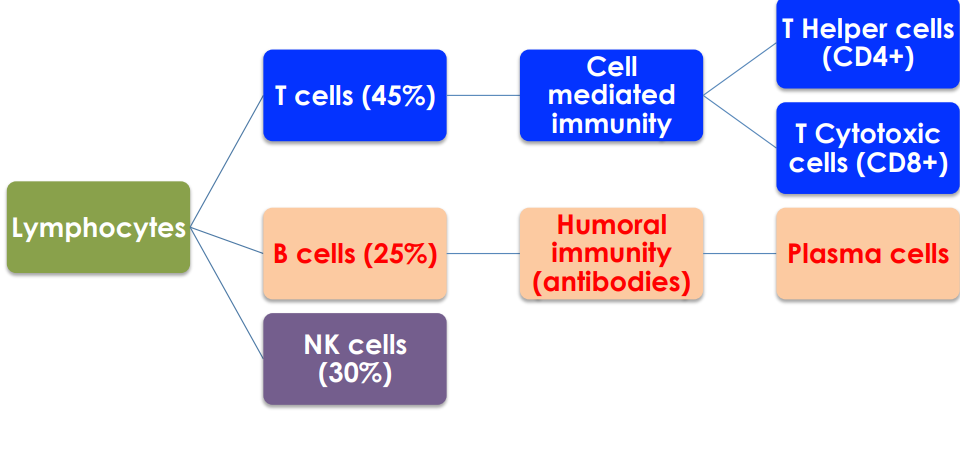
T is for timeless.
Cell mediated immunity is important for viruses
Low levels of CD4+ is found with HIV and AIDs
Abnormal Lymphocyte Counts
Lymphocytosis:
- Certain infections
- Viral (e.g. infectious mononucleosis)
- Lymphoid malignancies (chronic lymphocytic leukaemia CLL)
Lymphopenia:
- Steroid excess
- Therapy
- Acute Stress
- Malignancy
- Hodgkin’s lymphoma
- Disseminated neoplasia
- Connective tissue disorders
- Certain infections (TB)
- Chemotherapy
- Immune deficiency
Platelets
Structure:

Function:
- Haemostatic
- Platelet-damaged vessel wall interactions
- Platelet-platelet interactions
Quantitative Abnormalities
- Thrombocytopenia
- Immune Thrombocytopenic Purpura (ITP)
- Marrow failure
- Thrombocytosis
- Reactive (e.g. Rheumatoid Arthritis)
- Essential Thrombocythemia (ET)
Qualitative Abnormalities
- Membrane glycoprotein abnormalities (e.g. Glanzman’s disease)
- Granule defects (Storage pool defects)
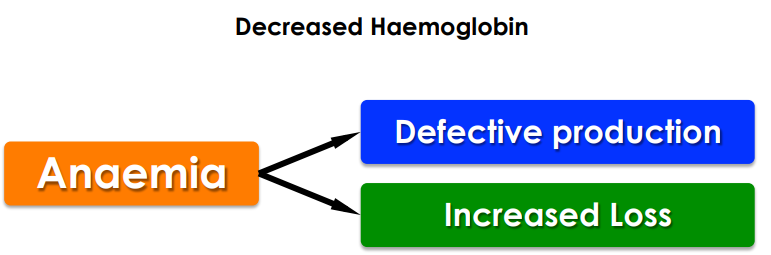
Pathological Classification of Anaemia
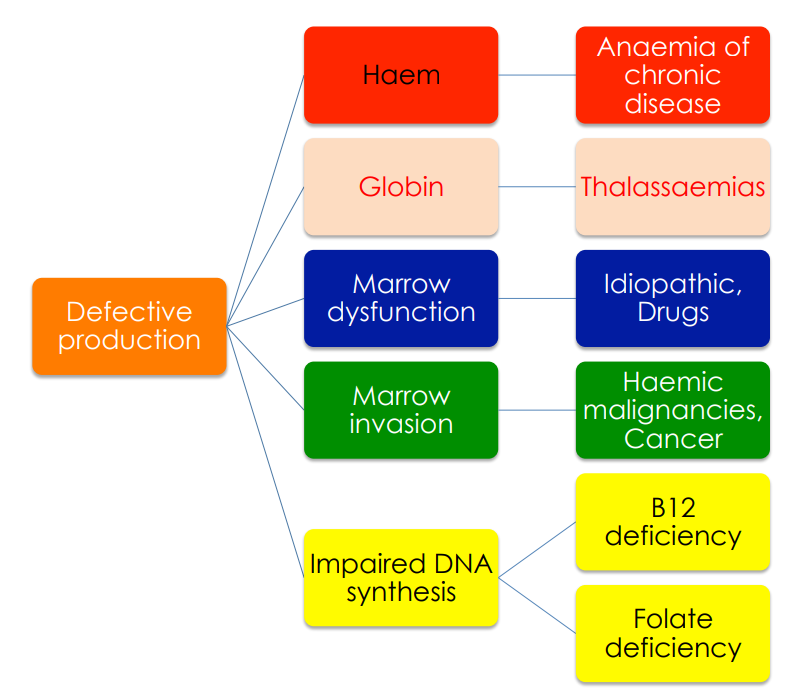
Haemoglobin is produced in the liver mainly. Globin production is much better protected by nature.
Thalassaemia is more common in south east Asia and Africa.
B12 deficiency is common in vegetarians/vegans.
Increased Loss:
- Haemolysis
- Intrinsic to the RBC
- Extrinsic to the RBC
- Bleeding
- Acute
- Chronic (iron deficiency)
Normal Haematological Counts
- Haemoglobin:
- Men: 13-18g/dl
- Women: 12-15g/dl
- White blood cell count: 5-10 x10^9/l
- Platelets: 150-400 x 10^9/l
White Blood Cells: Differential Counts
- Neutrophils: 2.0-7.5 x 10^9/l 40-75%
- Lymphocytes: 1.5-4.0 x 10^9/l 20-45%
- Monocytes: 0.2-0.8 x 10^9/l 2-10%
- Eosinophils: 0.04-0.4 x 10^9/l 1-6%
- Basophils: <0.01-0.1 x 10^9/l 1%
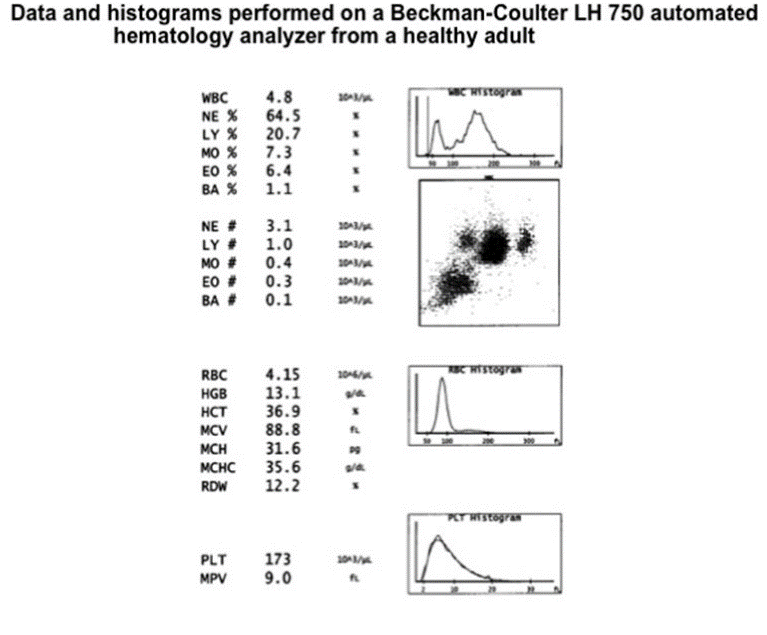
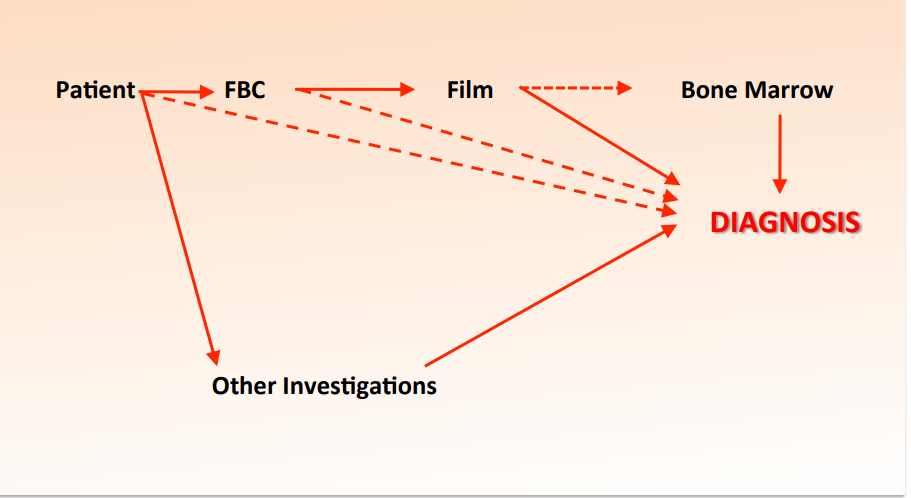
Coulter counters machine results
Derived Red Cell Indices
Packed Cell Volume (PCV) = RBC x MCV
(Haematocrit HCT)
Mean Corpuscular Hb (MCH) = Hb ÷ RBC
Mean Corp. Hb Conc. (MCHC) = Hb ÷ Reduced PCV
Red Cell Indices
Men | Women | |
Haemoglobin (Hb) | 13-18g/dl | 12-15g/dl |
Red Blood Count (RBC) | 4.5-6.5 x 10^12/l | 3.8-5.8 x 10^12/l |
Mean Cell Volume (MCV) | 78-93fl | |
Packed Cell Volume (PCV) | 0.4-0.52 l/l | 0.37-0.47l/l |
Reticulocyte Count | 0.2-2.0% | |
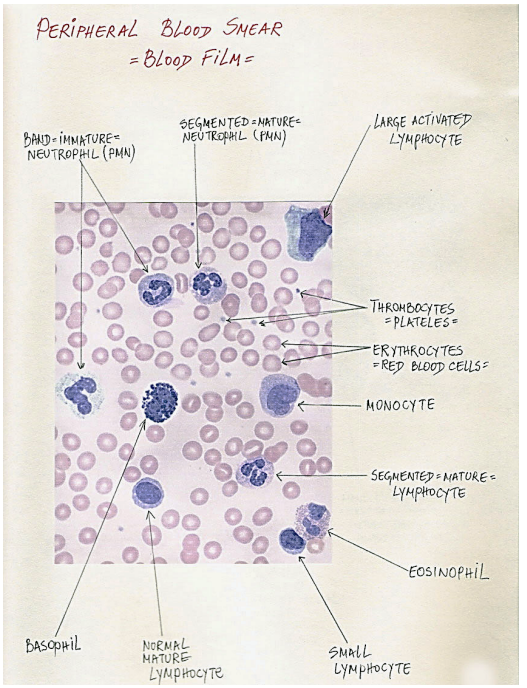
The sample is stained with haematoxylin and eosin stain which stains white cells blue and red cells red.
Gets observed by haematologists.
Red Cell Abnormalities
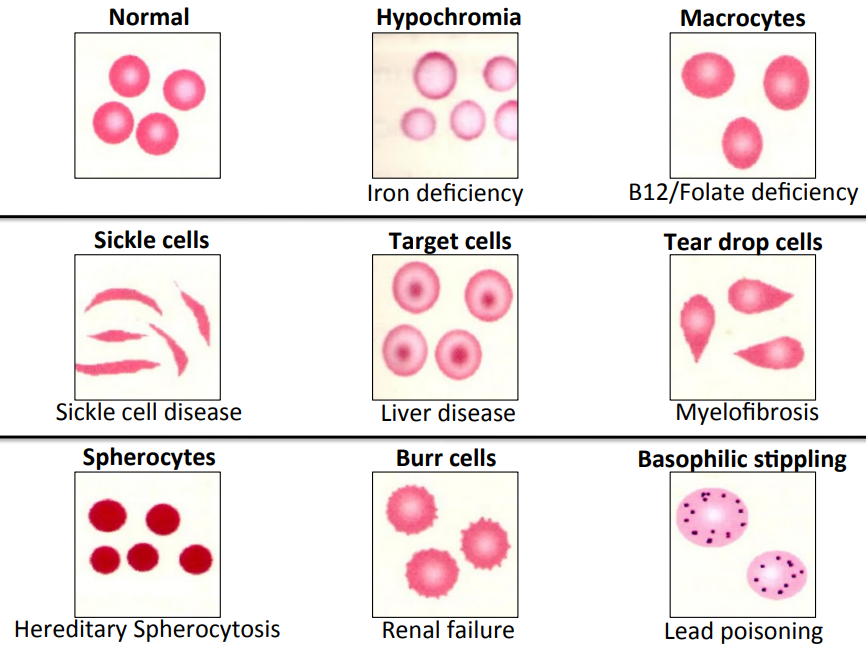
Anaemia - pale
B12/Folate deficiency - bigger
Sickle cell – deform completely
Observe size, shape, etc
Hypochromic Blood Film

Very pale and pencil-shaped
The Commonest cause of hypochromia is blood loss (gastritis) and therefore, iron deficiency.
Gum Infiltration by Monocytic Leukaemia

Monocyte count will be up in blood tests
Oral Candidiasis (Thrush)

Diseases that cause patients to be prone
Such as immune deficiency and low white cell count (neutrophils)
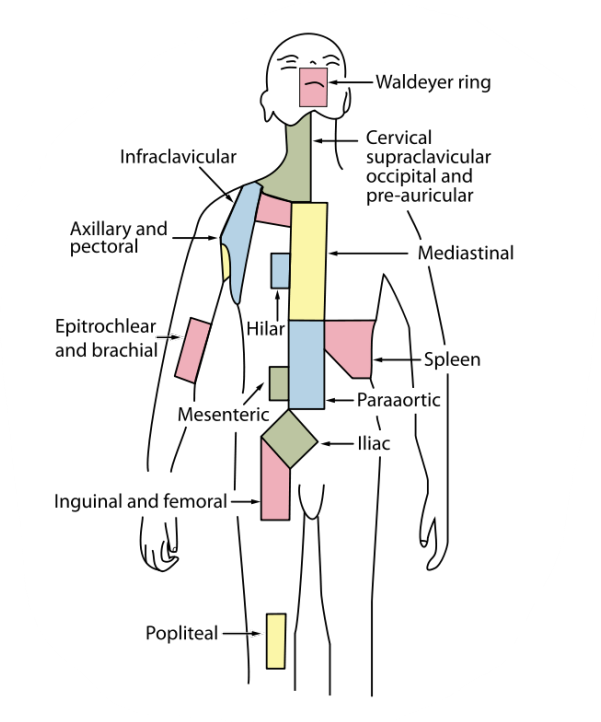
Lymph nodes
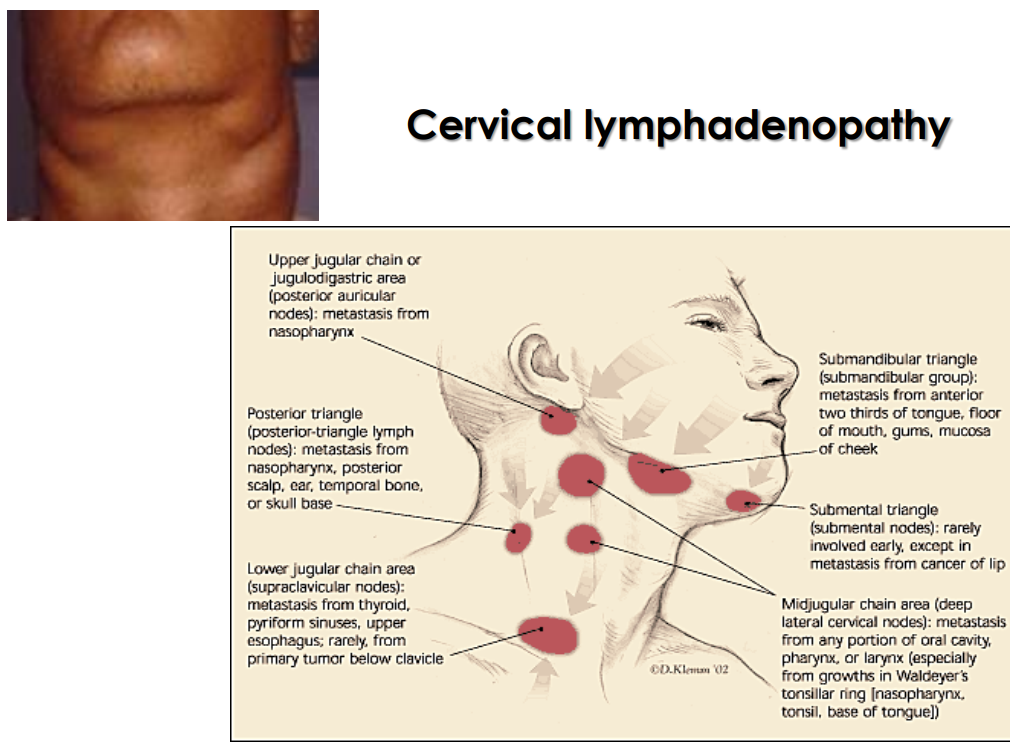
Cervical Lymphadenopathy
Shingles
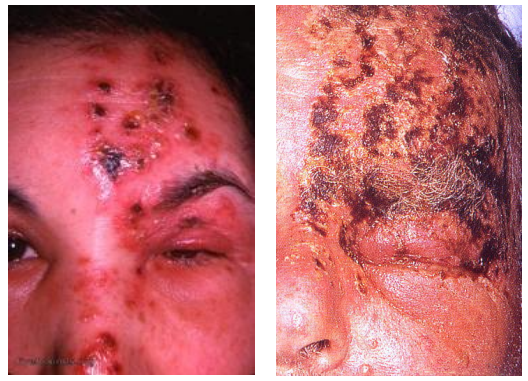
Virus that causes shingles is Herpes zoster
Can affect the trigeminal nerve (appear as toothache)
Infectious Mononucleosis
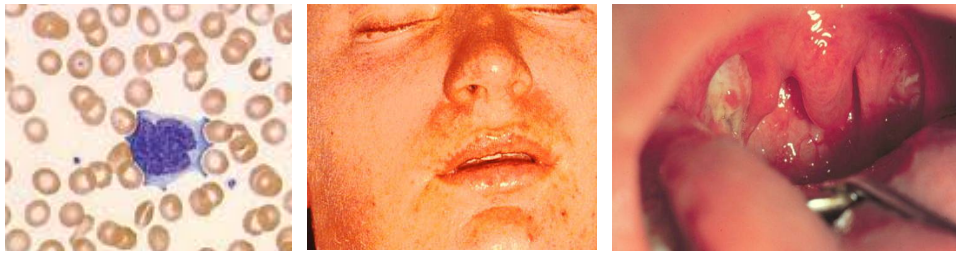
Virus that causes IM is Epstein Barr virus
Gives rise to an atypical lymphocyte
Can lead to lymphomas if not dormant.