Episcleritis
Infections and Inflammations of the Sclera and Episclera
Sclera: tough, outer fibrous coat. Problems are very rare but can be potentially blinding and require urgent referall.
Episclera: Relatively thin layer of vascular connective tissue that lines the outermost layer of the sclera. Problems in the episclera are relatively quite common.
Episcleritis
Definition: Inflammation of the episclera, the space between the sclera and the conjunctiva, involving the episclera and Tenon's capsule.
Commonality: A prevalent condition that is typically benign, self-limiting, and potentially recurrent. It is non-sight threatening.
Demographics: Most commonly affects young adults to middle-aged individuals, with a higher prevalence in women.
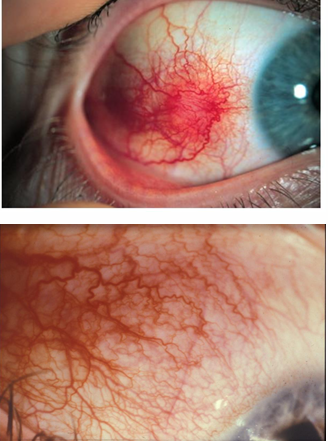
Symptoms: Can be asymptomatic or present with tenderness in the affected area. Presents as a sectorial, diffuse (more common) or nodular redness under the conjunctiva, typically near the limbus (usually unilateral)
Etiology: Most cases are idiopathic; some have associations with collagen vascular diseases such as:
Rheumatoid arthritis
Polyarteritis nodosa
Systemic lupus erythematosus (SLE)
Gout
Herpes zoster ophthalmicus (HZO)
Main Presentations of Episcleritis
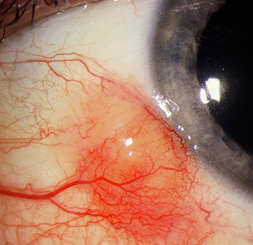
Simple Sectorial Episcleritis: sector of redness within the eye. Most common form of Episcleritis.

Simple Diffuse Episcleritis: redness is more generalised across the eye.

Nodular Episcleritis: redness enlarges into a raised nodule in the episclera. Least common form.
Simple vs Nodular:
Simple:
Rapid onset: reaches maximum redness in 12 hours
Resolves quickly: two to three days
can recur in the same eye or opposite eyes.
Nodular:
gradual onset: enlarges over a couple days
Lasts longer
More discomfort then simple episcleritis.
Nodular Episcleritis
Symptoms: More intense than simple episcleritis.
Duration: Tends to last longer than simple episcleritis.
Association with Systemic Disease: Stronger link with systemic diseases compared to simple episcleritis.
Rheumatoid Arthritis (RA): 5%
Herpes Zoster Ophthalmicus (HZO): 7%
Gout: 3%
Appearance:
Focal area of hyperaemia with a raised congested nodule.
The nodule may be translucent
Nodule can be mobile.
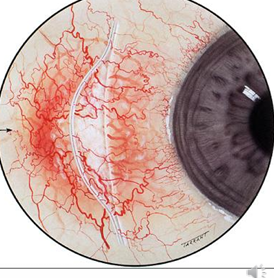
Differentiating from Scleritis
Key Differences:
Oedema and dilated vessels in episcleritis are superficial and do not involve the sclera.
Scleritis patients will present with more painful symptoms.
Slit-lamp Examination:
Posterior surface appears flat in episcleritis.
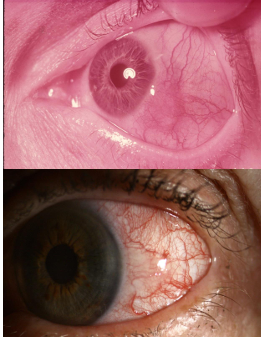
Phenylephrine 2.5% drops cause blanching of episcleral vessels, but scleral vessels remain dilated. Eye will become white in episcleritis
Hue of Hyperaemia:
Episcleritis: Pink to red
Scleritis: Blue to purplish red
Management and Treatment of Episcleritis
Natural Course: Usually spontaneously resolves, as it is self-limiting and benign.
Comfort Measures:
Non-preserved lubricants
Cold compresses
Very short-term decongestants
If Discomfort is Marked: Surface steroid, e.g., FML 0.1% suspension (administered q6h). Useful for nodular episcleritis (more symptomatic).
Systemic NSAIDs: May help in reducing frequency and severity of recurrent episodes.
Medical Workup: Recommended especially for cases that are recurrent, nodular, or unresponsive to treatment. Remind patient this is a condition that may recur.