Burns
Overview of Burn Injuries
Burn injuries result from damage to skin or tissues from heat, chemicals, electricity, or radiation.
Men are twice as likely to have burn injuries than women.
Adults between 20 to 30 years old have the highest prevalence of burn injuries.
long length
Types of Heat Injuries
Dry heat injuries result from open flames or explosions.
Moist heat injuries result from contact with hot liquid or steam.
Thermal burns occur when clothing ignites from heat or flames.
Types of Burns
Chemical burns result from exposure to caustic agents.
Electrical burns occur when electrical current passes through the body, causing severe damage.
Radiation burns can result from therapeutic treatment for cancer or sunburn, causing thermal effects or damage to cellular DNA.
Factors Affecting Burn Injury Severity
Age of the patient, depth of burn, amount of surface area burned, presence of inhalation injury, other injuries, location of injury, and comorbid conditions.
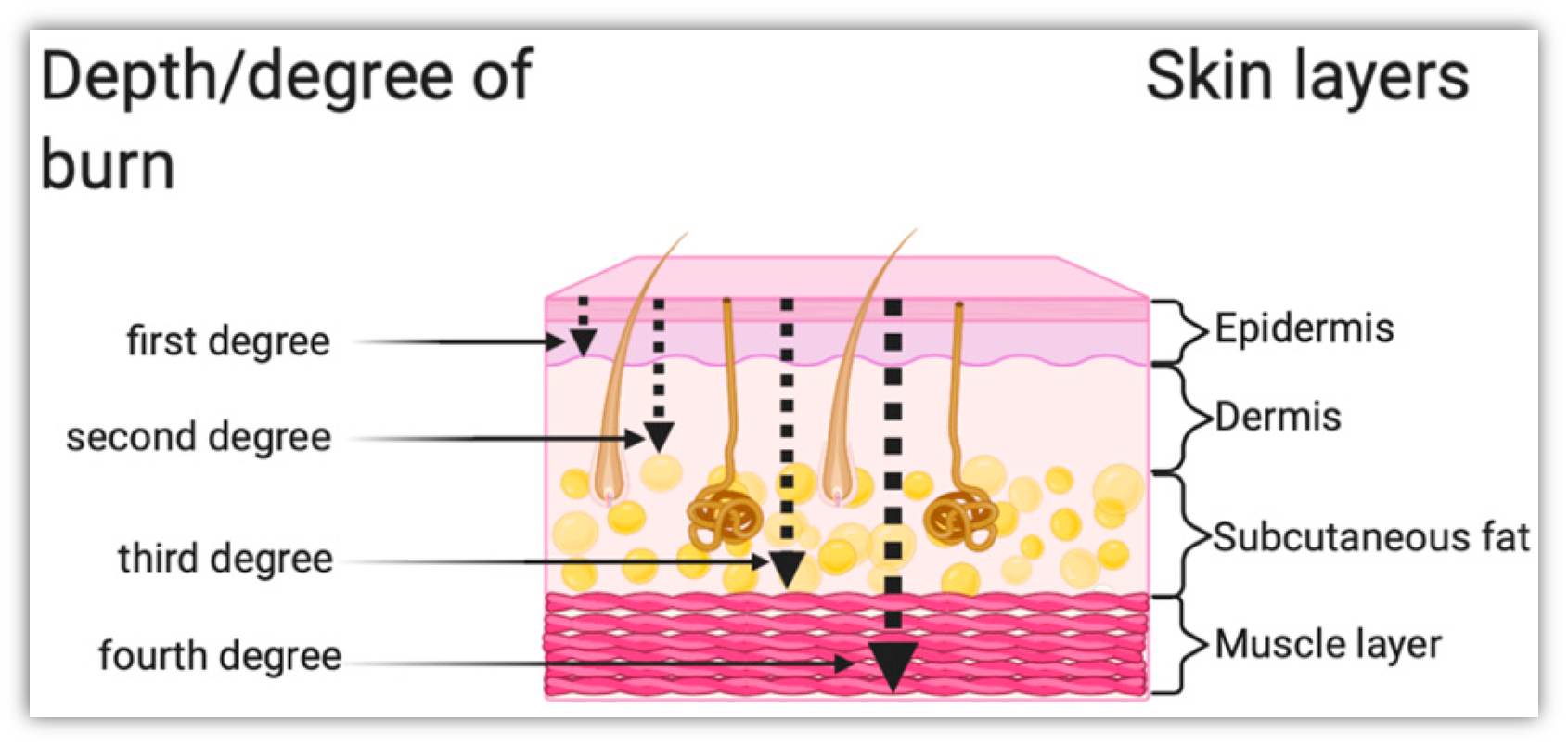
Burn Depth Classification
First-degree (superficial) burns involve the epidermis and have appearances like redness (blanches w/pressure), minimal/no edema and possible blisters. Sensation and healing involve tingling, hyperesthesia, pain that’s soothed by cooling, peeling, itching

Second-degree (partial thickness) burns involve the epidermis and a portion of the dermis, with appearances of pink, red, white, possible blistering and mild-moderate edema. Sensation/healing involve pain, hyperesthesia, sensitive to air currents, & may require grafting.

Third-degree (full thickness) burns affect the epidermis, dermis, and sometimes subcutaneous tissue, may involve connective tissue and muscle and nerve damage. Appearance with red, black, brown, yellow or white, can appear leathery or charred, severe edema and no blisters. Sensation/healing involves minimal or absent sensation, scarring, and grafting.

Fourth-degree burns damage all layers of skin, extending to deep tissues, muscles, and bones. Appearance includes black/charred, no edema or blisters. Sensation/healing include no pain, scarring, grafting and amputations are likely.

Burn Depth Assessment
Ability of burn to heal depends on the burn depth
Factors like how the burn occurred, causative agent, temperature &duration of contact with agent, and skin thickness at the injury site determine burn depth.
Burn Center and Extent of Body Surface Area
Burn centers are specially equipped to treat burn patients from injury through rehabilitation.
Patients may need transfer to a burn center for third-degree burns, burns face/hands/feet/genitalia/perineum/major joints, electrical burns, inhalation injuries, and other severe conditions.
Methods like the Rule of Nines, Lund and Browder method, and Palmar method are used to estimate total body surface area affected by burns.
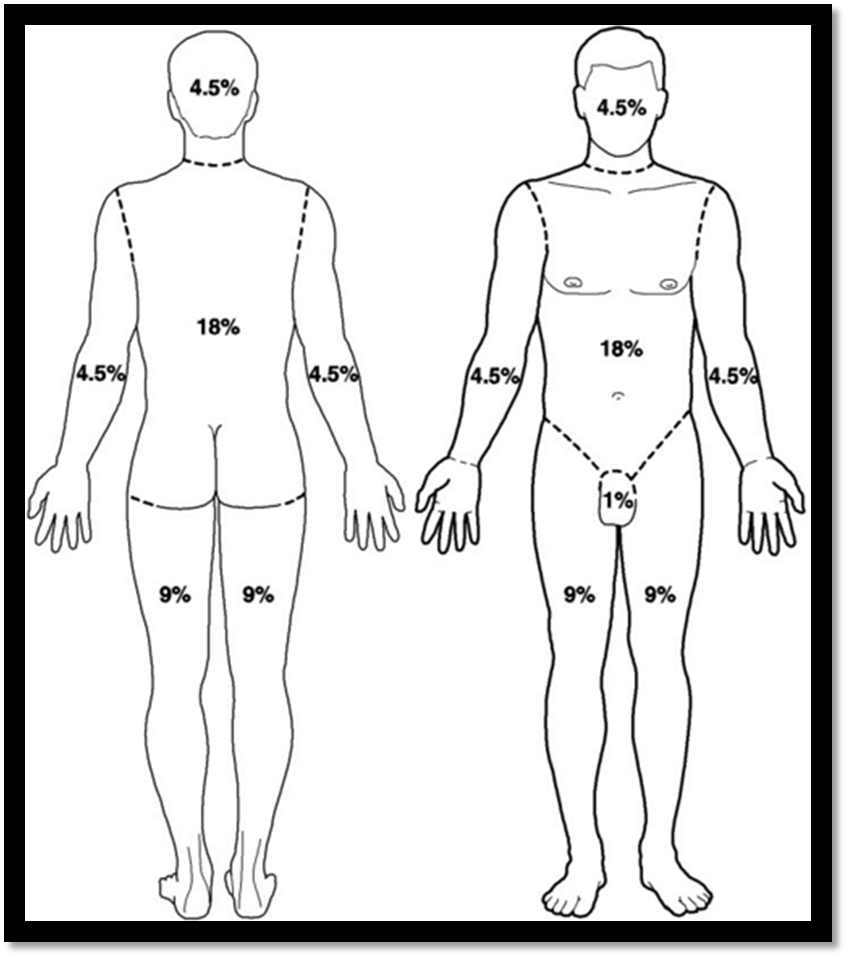
Rule of Nines and Calculation
The Rule of Nines is a common method based on anatomic regions to estimate burn extent.
Calculation involves summing up zones to determine the percentage of total body surface area burned.
Lund & Browder Method- more precise, uses percentage of surface area of specific anatomic parts
Palmar Method- quick method to approximate scattered burns, palm of patient’s hand (including fingers) = 1% TBSA
Management of Burn Injury
Management of Electrical Burns: serum creatinine kinase levels, risk for myoglobinuria, patient may require multiple surgeries.
Cardiovascular alterations: third spacing (capillary leak syndrome), “burn shock”, fluid resuscitation.
Fluid & Electrolyte Alterations- edema (forms rapidly after burn), circumferential burns, treatment (escharotomy/fasciotomy). Electrolyte abnormalities: sodium and potassium
Pulmonary Alterations: inhalation injuries- upper /lower airway injury
Clinical Manifestations: singed facial hair, sooty sputum, hoarseness, wheezing, stridor.
Dx: bronchoscopy
Upper airway injury- severe airway edema from direct thermal injury or secondary edema from face/neck burns. Possible tx: protective intubation
Lower Airway Injury- pt inhales smoke or noxious gases; possible carbon monoxide poisoning. Tx: 100% oxygen
Escharotomy/fasciotomy:
escharotomy:
fasciotomy:
Emergent/Resuscitative Phase
Phase begins with burn injury & ends with completion of fluid resuscitation.
PRIORITIES: ABC’s, prevention of shock/respiratory distress, detection & tx of associated injuries, wound assessment/initial care
transport to nearest ED
focus on ABC’s
continuous monitoring of airway patency
calculation TBSA burned
fluid resuscitation initiated AFTER urgent respiratory needs addressed
ABA Fluid Resuscitation Formulas
For adults with thermal or chemical burns:
2 mL LR (x) patient’s weight in kg (x) % TBSA
For adults with electrical burns:
4 mL LR (x) patient’s weight in kg (x) % TBSA
The total volume calculated will be administered over the initial 24hr post-burn period
One half of total calculated will be administered in first 8 hours post-burn injury
Second half of calculated volume is administered over the next 16 hours
Nursing/Collab Management- Fluid Resuscitation:
Urinary Output- desired 0.5 - 1 mL/kg/hr
Gold standard for monitoring response to fluid resuscitation
indwelling (foley) cath inserted
Nursing Interventions:
monitor temp
monitor resp. status
assess pulses
cardiac monitoring
potential difficulties w/ obtaining vital signs
elevation of burned extremities
assess pain level
Acute/Intermediate Phase
Phase begins with diuresis to ends with wound closure
Begins 48-72 hr after burn
Priorities of Acute/Intermediate Phase:
Wound care and closure
Prevention or treatment of complications, including infection
Nutritional support
Upper airway edema can lead to airway obstruction
Complications:
Endotracheal intubation, ventilator-associated pneumonia (VAP)
Potential for fluid overload
Hyperthermia
Surgical excision of necrotic tissue
Infection Prevention & Control
Burn injuries cause dysregulation of immune system
Clinical signs of infection
PPE for staff
gown, gloves, eye protection, mask
Wound cultures
Avoid prophylactic antibiotics
Wound Cleaning
Goal of wound care:
remove nonviable tissue/wound exudate/previously applied topical agents
Patients who are:
Hemodynamically unstable- wash wounds at bedside
Ambulatory- pt may shower independently or w/ assistance.
Non-ambulatory- can be bathed/receive wound care using shower cart
Wound Dressing
Application of several dry dressings after prescribed topical agents
Circumferential dressings- apply distally to proximally
Wrap fingers/toes individually
Facial burns
Dressings after new skin grafts
Nursing interventions:
dressings that adhere to wound bed
documentation
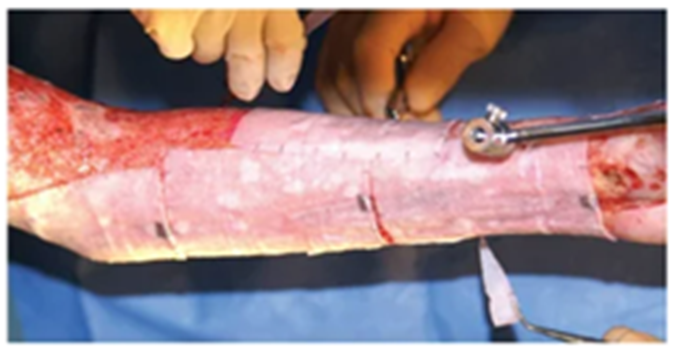
Wound Debridement
Removal of devitalized tissue to prepare site for healing & possible grafting
4 types of debridement: natural, mechanical, chemical, surgical
Natural Debridement
devitalized tissue spontaneously separates from underlying viable tissue
bacteria present between devitalized & viable tissues gradually liquifies the fibrils of collagen that hold eschar in place
Mechanical Debridement
uses tools to separate & remove eschar
usually performed w/ routine dressing changes
“wet-to-wet” or “wet-to-moist” dressings
Chemical Debridement
use of topical enzymatic agents to debride burn wounds
can be combined w/ topical abx therapy
topical agents containing silver can deactivate chemical debriding agents
Surgical Debridement
Timeframe- may be performed ASAP after injury
post-Procedure Interventions- wound covered immediately w/ skin graft (if necessary) or dressing. Temporary biologic or synthetic dressing possibly
Risks- extensive blood loss. Anemia related to blood loss
Benefits- shorter length of hospitalization. Granulation tissue creates barrier to bacteria
Wound Grafting
Use for deep partial- or full-thickness burns
permits earlier function
reduces scar contractures
Autograft Types and Characteristics
preferred autologous method for burn wound closure
not rejected by pt’s immune system
Types of Autografts:
Split-thickness Autografts
most common
remaining donor site retains sweat glands/hair follicles
Application- sheets; expanded by meshing
scar formation
graft loss
Full-thickness Autograft
donor site includes dermis & epidermis
consider cautiously
Cultured Epithelial Autograft (CEA)
used w/ massive burns (>90% TBSA burned)
availability of non'-burned skin as donor sites
cultures grown from full-thickness biopsies that were obtained from pt’s unburned skin (culture)
about 3 weeks for final product to be ready
Disadvantages-
fragile, prone to graft loss. Expensive. Requires long length of stay
SHEET GRAFT

MESHED GRAFT
Care of Graft Site
Post-op goals: protection & immobility
1st dressing change
early graft loss
careful patient positioning/turning
elevating grafted extremities
Care of Donor Site
Dressing applied to site after hemostasis is obtained
Painful wound
potential site of infection
very susceptible to pressure injury
should heal spontaneously 7-14 days
Temporary Wound Coverage
Body’s immune response will eventually reject
provide temporary wound coverage until autografting is possible
stay in place for varying lengths of time
removed for bacterial colonization, infection, rejection
Temporary Wound Coverage:
Homografts:
avail from “skin banks”
revascularization occurs within 45H
may be left for several weeks
Advantages: best infection control of all biologic/biosynthetic dressing
Disadvantages: most expensive biologic dressing
Xenografts:
avail from commercial suppliers
used for temp covering of clean wounds
Advantages: provides pain control, allows underlying wound to re-epithelialize
Disadvantages: does not vascularize
Biosynthetic & Synthetic Dressings:
may eventually replace biological dressings
many products on the market
tend to be expensive
Pain Management
burn injuries are considered one of the most painful types of trauma
pain management plan should address background, breakthrough & procedural pain
Background Pain:
a continuous level of discomfort experienced even when pt is inactive/not undergoing procedures
Goal: to provide long-acting analgesic agent that will provide uniform coverage for long-term discomfort
Use small, escalating doses when initiating analgesia to reach acceptable level of pain control
PCA
Breakthrough Pain:
acute, intense & episodic pain. Generally related to an activity/movement of affected area
Goal: to achieve PRN pain control using short-acting agents
Procedural Pain:
discomfort that occurs w/ procedures such as daily wound tx, invasive line insertions, PT/OT
Goal: plan proper analgesia to facilitate comfort for pt throughout procedure
Pharmacologic treatment:
opioids, NSAIDS for pain
benzos for anxiety
antipruritic agents, water/silica-based lotion for itching
Nonpharmacological therapies:
relaxation techniques, distraction, guided imagery, therapeutic touch
Nutritional Therapy
Early nutritional support
Nasogastric tube placement if needed
High-protein, high-calorie meals if able to take PO
Dietary consult
Promoting Physical Mobility
Deep breathing, turning, and proper positioning
Passive & active ROM exercises
Splints/functional devices
PT/OT consults
Other Nursing Interventions
Daily weight
Strict I&O
Monitor sodium levels
Regular bathing & linen changes
Documentation: nutritional intake, wound status
report any significant changes in wound to provider
Potential Complications
Acute respiratory failure/acute resp. distress syndrome
Heart failure
Sepsis
Delirium
Rehabilitation Phase
Phase begins after wound closure & ends at pt’s return to optimal level of physical/psychosocial adjustment
Priorities:
prevention & tx of scars & contractures
physical, occupational & vocational rehab
functional & cosmetic reconstruction
psychosocial counseling