Engineering - heart valves
Nature of the Pathology:
- The aortic valve controls the flow of blood out from the heart to the rest of the body. If the valves don’t open or close properly, the blood flow through your heart to your body can be disrupted
The aortic valve may need to be replaced for 2 reasons:
- the valve has become narrowed (aortic stenosis) the opening of the valve becomes smaller, obstructing the flow of blood out of the heart
- the valve is leaky (aortic regurgitation) the valve allows blood to flow back through into the heart
Complications:
- heart failure
- stroke
- blood clots
- heart rhythm abnormalities
- death
Implications of complications:
- the problems can get worse over time and in severe cases can lead to life-threatening problems such as heart failure if left untreated
- all these complications would lead to more intervention needed by doctors and would require more medical care
- this would increase the amount of money spent by the NHS
Diagnosis:
- Echocardiogram: ultrasound scan where a transducer, emits high frequency waves which create echoes by bouncing off the heart. These echoes are picked up by the probe, creating images of the beating heart. 3D or transoesophageal echocardiogram may also be used. The latter produces images at a different angle, closer to the aortic valve.
- Electrocardiogram: Electrodes are attached to the chest and sometimes limbs to measure electrical activity of the heart i.e. how fast the heart is beating or if there’s an abnormal rhythm. This test can also show signal patterns which could suggest heart disease or swelling.
- X-rays: used to take images of the heart and chest. Can show swelling of the aorta and calcium build-up on the aortic valve (stenosis)
Treatment:
3 main types of mechanical valve:
caged ball:
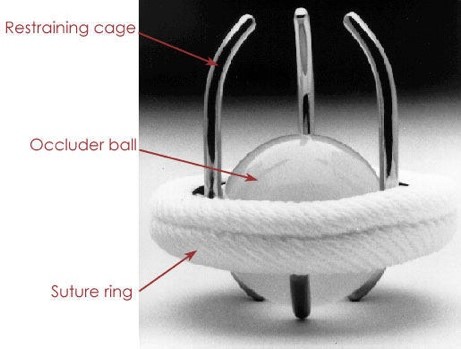
silicone elastomer ball in a metal cage
- earliest design
- blood pressure within chamber > pressure outside, ball pushes against cage allowing blood flow
- post contraction, pressure drops and ball returns to base of valve, forming a seal
tilting disc:
- introduced in 1969
- single circular occluder controlled by a metal strut
- ePTFE walls stitched into the heart to hold it in place
- ring contains flexible ring that opens and closes as blood flows
bileaflet:
- two semi circle leaflets that rotate around struts attached to the ring
- some have suggested this creates more natural flow of blood
- most common design
Traditional insertion method: recovery time 1 to 3 months
- heart-lung bypass machine used to circulate blood around the body as heart must be stopped
- cutting open chest and breastbone for access
- valve stitched into heart
Transcatheter aortic valve implantation (TAVI): shorter recovery time:
- catheter inserted via groin or wrist to reach the valve
- This inserts a folded valve which unfolds to sit on top of the existing valve
- Heart doesn’t need to be stopped; faulty valve doesn’t need removing
MitraClips:

connect mitral valve leaflets A2 (anterior) and P2 (posterior) to treat mitral regurgitation
- inserted using TAVI method. Before procedure is carried out, the morphology (form) and pathology causing regurgitation are determined
- small metal clip covered in polyester
- consists of a guide catheter which is inserted via the femur and then into the left atrium across the septum, guided using ECG
- helps valve to close more fully
Future and Development:
Polymeric Materials:
- potential materials for prosthetic valves
- overcome many clinical and mechanical challenges
- can be designed to match native tissue closely
- promising both financially and physiologically
Treatment methods:
- more patients will be receiving TAVI
- doctors can perform smaller incisions when inserting prosthetic valves
Tissue engineering:
- functional, living semi lunar valve replacements being developed in vitro
- often require isolation and culture of many autologous cells (patient’s own stem cells)
Limitations:
- tendency for blood clots to develop on valve’s metal surface so lifelong prescription of blood thinners required to prevent complications eg heart attack or stroke
- use of blood thinners prevents patient from doing high intensity physical activity
- stitches holding mechanical valve in place can be damaged by other cardiovascular conditions the patient may have