Week 5: Complications From Heart Disease
Week 5: Complications From Heart Disease
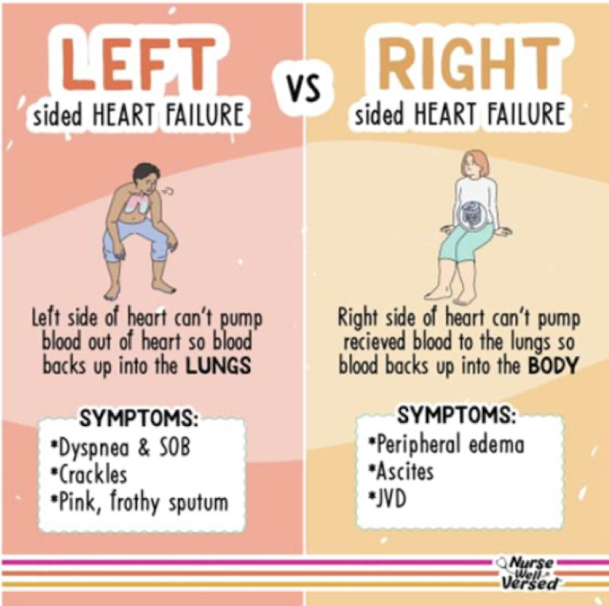
Heart Failure
The heart muscle is unable to pump effectively, resulting in inadequate cardiac output, myocardial hypertrophy, and pulmonary/systemic congestion. The heart is unable to maintain adequate circulation to meet tissue needs.
HF is the result of an acute or chronic cardiopulmonary problem, such as
Systemic hypertension
MI
Pulmonary hypertension
Dysrthmias
Valvular heart disease
Peridcarditis
Cardiomyopathy
Heart Failure Classification
New York Heart Association functional classification scale
Class I: client has cardiac disease but exhibits manifestations with activity
Class II: client has manifestations with ordinary excretion (everyday ADLS)
Class III: client displays manifestations with minimal exertion
Class IV: client has manifestations at rest
American College of Cardiology and American Heart Association staging heart failure
A: high risk for developing heart failure
B: cardiac structural abnormalities or remodeling, but no manifestations of heart failure
C: current or prior manifestations of heart failure
D: refractory end-stage heart failure
Heart Failure Key Terms
HF: The heart’s inability to effectively fill and/ or pump blood
Stroke volume
Volume of blood pumped by the heart per contraction
Cardiac output
Volume of blood pumped by the heart per min
CO = SV x HR
Preload
Amount of blood in the LV before contraction
Afterload
Stress on the ventricular wall during systole (contraction)
Ejection fraction
% of blood leaving the heart during each contraction
Frank-Straling mechanism
Loading the ventricle with blood during diastole, stretching out the cardiac muscle, = increased SV during systole
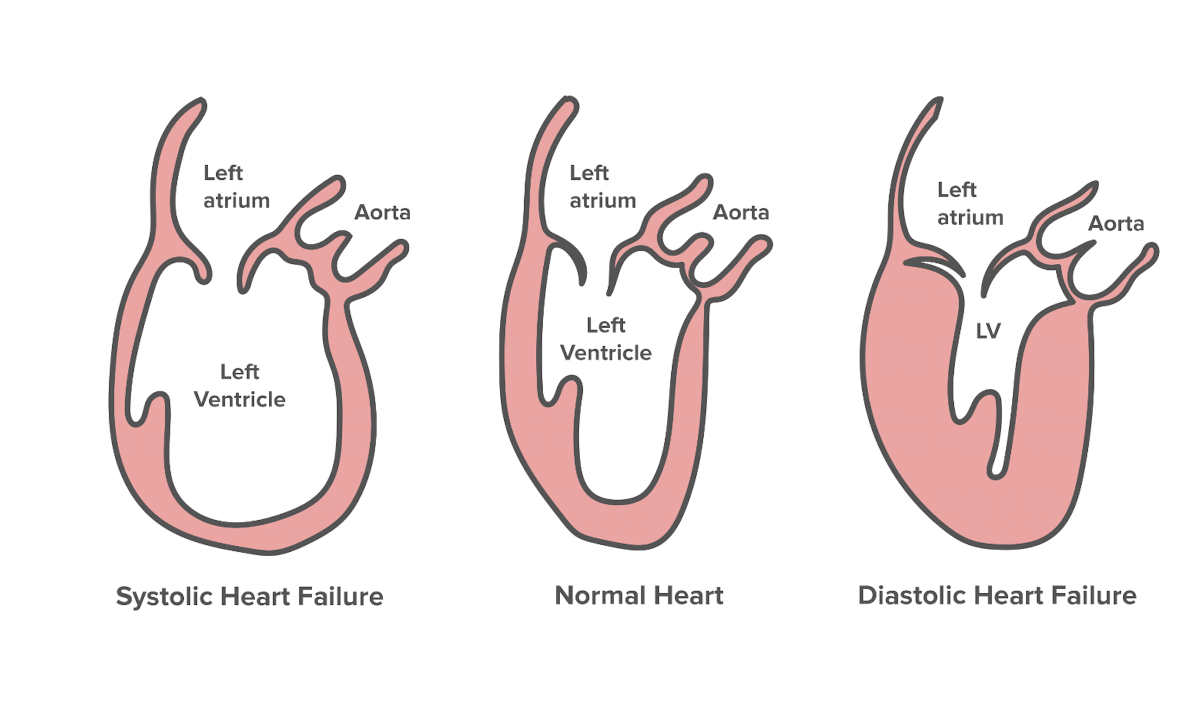
Heart Failure with Reduced Ejection Fraction (HFrEF)
Systolic HF: “pump dysfunction.”
Causes
Decreased force of contraction (MI)
Decreased supply of the heart (CAD)
Afterload (HTN)
Impaired mechanical function valve disease)
Normal preload, decreased force of contraction leading to inadequate emptying of ventricles during systole (contraction), causing decreased EF
Heart Failure with Preserved Ejection Fraction (HFpEF)
Diastolic HF: “filling dysfunction.n”
Causes
Restrictive cardiomyopathy (amyloidosis)
Valve disease
HTN
Ventricles are noncompliant and unable to fill during diastole (rest), leading to increased filling pressure, decreased preload, and normal force of contraction, causing decreased SV and preserved EF.
Heart Failure Risk Factors
HTN
DM or metabolic syndrome
Obesity
Smoking
CHD
Chronic tachyarrhythmias
Anemia
Increasing age
CAD
Stroke
PVD
Valvular heart disease
Heart Failure Complications
Cardiogenic shock
Biventricular heart failure
Arrhythmias
Liver damage
End organ damage
Exacerbation of HF
MNEMONIC: FAILURE
Forgot medication
Arrhythmia/anemia
Ischemia/infarction/infection
Lifestyle
Upregulation of CO (pregnancy)
Renal failure
Embolism (pulmonary)
Heart Failure Management
Perload agents
Loop diuretics
Thiazide
Potassium-sparing
Afterload-reducing agents
ACE or ARB
CCB
Phosphonsiesterase-3 inhibitors
Surgery
Heart transplant
Lifestyle modification
Ventricular assist device (VAD)
Implanted defibrillator
Diventricular pacemaker for resynchronization
Acute Decompensation
Mnemonic: POND
Position (upright) +/- positive pressure ventilation
Oxygen
Nitrates
Diuretics
Heart Failure Nursing Management
Assess:
Observing the effectiveness of therapy
Patients' ability to understand and implement self-management strategies
s/s of pu,monary and systemic fluid overload
I & O
Emotional response to the diagnosis of HF
Coping skills
Health history
Fatigue
SOB
Dyspnea on exertion
Cough
Sleep distrubancer, PND: number of pillows needed for sleep
Edema
Abdominal symptoms
AMS
ADLS
Daily weights
Activities that cause fatigue
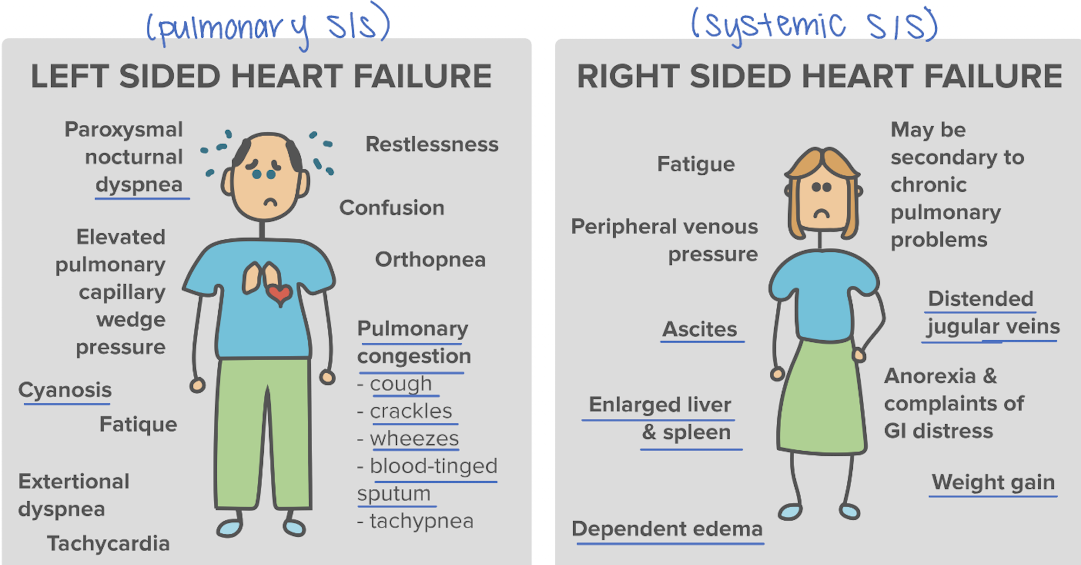
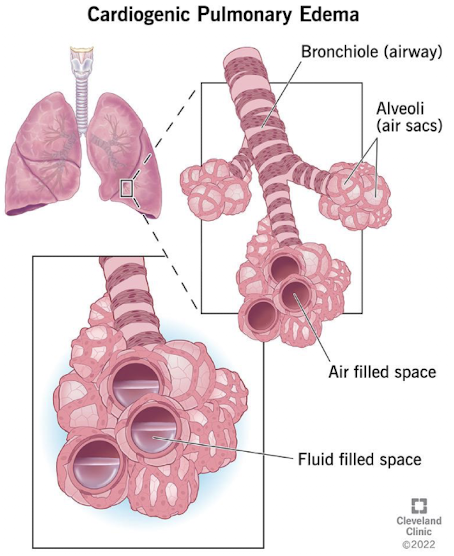
Pulmonary Edema
The accumulation of excessive fluid in the alveolar walls and alveolar spaces of the lungs
Cardiogenic form of pulmonary edema is caused by disturbances in the Starling forces.
The pulmonary capillary pressure increases.d
The alveoli are normally kept dry because of the negative pressure in extra-alveolar interstitial spaces, but when there is:
Increased pressure/pooling → increased pulmonary venous pressure → increased pulmonary capillary pressure → fluid in interstitial spaces → increased pressure in interstitial spaces → fluid in alveoli (pulmonary edema)
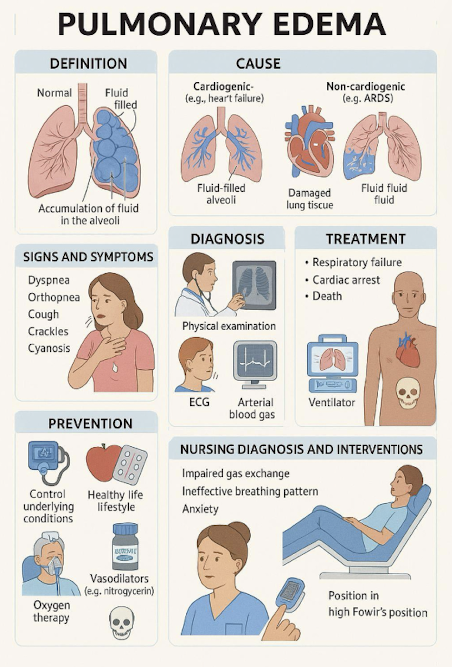
S/S Pulmonary Edema
Trouble breathing or SOB
Feeling of anxiety related to breathing difficulties
Wheezing or noisy breathing
Quick, shallow breathing
Trouble breathing while lying down
Confusion
Discomfort related to breathing
A feeling of suffocation
Coughed-up sputum that appears frothy and pinkish, if blood is present
Pale of bluish skin
Sweating or feeling clammy
Swelling in the feet or ankles
Management of Pulmonary Edema
Supplemental oxygen
Medications:
Diuretics ( to rid the body of excess fluid)
Nitroglycerin ( to help lower pressure within the heart)
inotropes ( to help the heart pump more efficiently)
ACE inhibitors ( to manage blood pressure levels)
Morphone can help reduce anxiety and improve breathing
Continuous positive airway pressure (CPAP)
Ventilators, when other methods are unsuccessful
Renal replacement therapy, when pulmonary edema causes kidney failure
Cardiogenic Shock
A life-threatening emergency where the heart suddenly cannot pump enough blood to meet the body’s needs, often caused by a MI.
Critical hypotension → organ failure
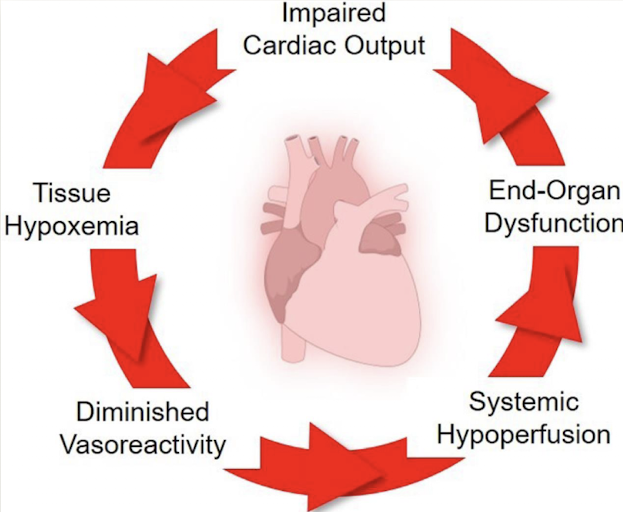
Cardiogenic Shock Pathophysiology
Obstruction reduces blood flow into or out of the heart
SV decreases
CO decreases
Organ and tissue hypoperfusion
To compensate, the body releases vasoconstrictors
When compensatory mechanisms fail
Severe tissue hypoxia
Multiple organ failure
Blood backs up into the pulmonary and systemic circulation
Complication
Pulmonary edema
Peripheral edema
Cardiogenic Shock Causes /Risk Factors
Any condition that prevents the heart from pumping sufficient blood:
MI
Myocardial contusion
Myocarditis
HF
Arrhthmias
Valve insufficiency
Risk factors
Existing heart condition
Chronic hypertension
Coronary heart disease
Diabets
Medications
Electrolyte imbalances
Asian Americans and pacific islanders
Cardiogenic Shock S/S
Initial stage
Tachycardia
Decreased mean arterial pressure (MAP)
Blood pressure normal
Compensation stage
Decreased MAP
Skin is cold and clammy
Pallor
Hypotension
Tachycardia
Decreased peripheral pulses
Oligiura
Jugular venous distension
Pulmonary edema
Peripheral edema
Progressive stage
Decreased MAP sustained
Anxeity
Altered LOC
Cyanosis
Tachypena
Low oxygen saturation
Hypotension
Bradycardia
Arrhythmias
Refractory stage
Decreased MAP sustained
Multiple organ dysfunction
Sudden loss of consciousness
Shallow respirations
Unmeasurable oxygen saturation
Non-palpable pulses
Death
Cardiogenic Shock Management
Address the underlying cause
Inotropic medications
Mechanical support device
Goal of care
Maintain CO
Monitor for complications
Monitor for improved hemodynamic stability
Assess vital signs, LOC, pulses, heart and lung sounds, and pain
Report to HCP immediately
Chest pain
Hypotension
S3 heart sounds
Pulsus paradoxus (exaggerated drop in systolic blood pressure during inspiration)
Continuous cardiac monitoring
Administer IV fluids, review ABG results
Notify HCP immediately
Tachycardia
Tachypnea
Confusion
Headache
Insert an indwelling catheter
Measure intake and output
Check for decreased cerebral perfusion pressure
Notify HCP immediately
Minimal urine output
Altered LOC
Cool or clammy skin decreased peripheral pulses
Monitor central venous pressure and MAP
Cardiogenic Shock Patient/ Family Teaching
Explain the condition, plan of care, and how to safely self-administer medications.
Promote heart health
Smoking cessation
A healthy diet
Provide transitional resources
Instruct how to recognize signs of shock
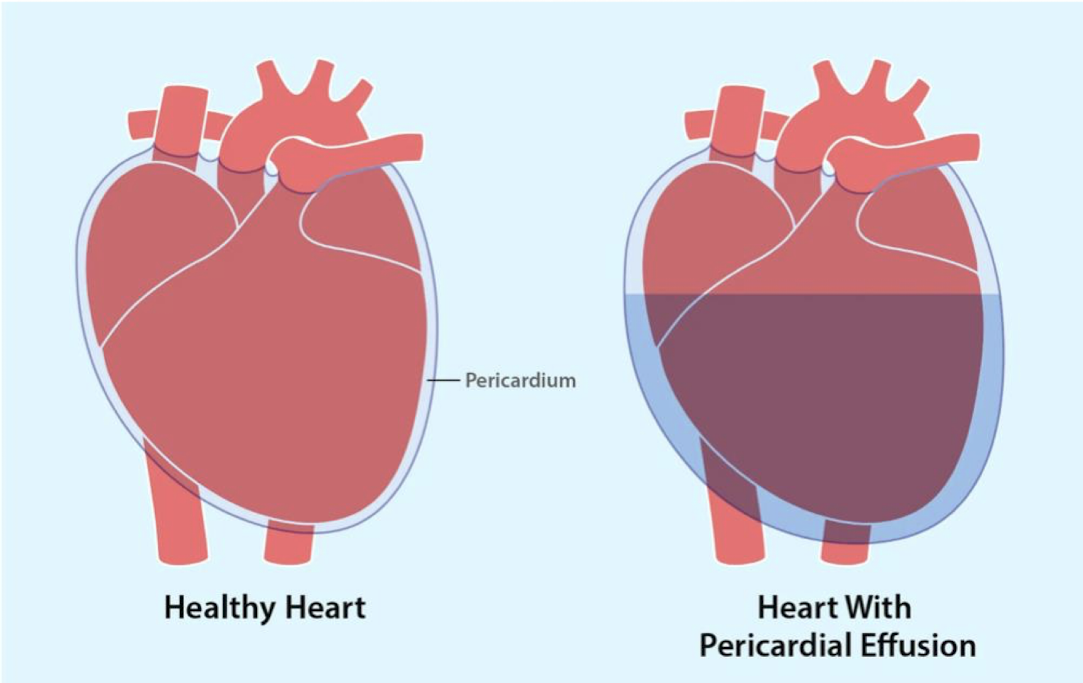
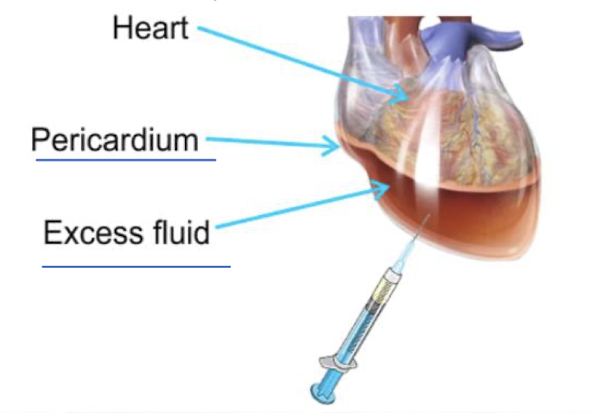
Pericardial Effusion and Cardiac Tamponade
Pericardial effusion = fluid accumulation in the pericardial sac
Cardiac tamponade = a life-threatening emergency where fluid or blood rapidly accumulates in the pericardial sac, compressing the heart and preventing proper filling
Cardiac Tamponade S/S
Beck’s Triad (classic findings)
Hypotension
Jugular vein distension: a bulging neck vein due to high pressure
Muffle Heart Sounds: Heart during auscultation
Respiratory and Cardiovascular Distress
Dyspnea, tachycardia
Chest pain improved by sitting up or leaning forward
Chest pain is often sharp, radiating to the neck, shoulders, back, or abdomen
Tachycardia
Pulsus paradox (decreased systolic BP > 10 mm Hg with inspiration)
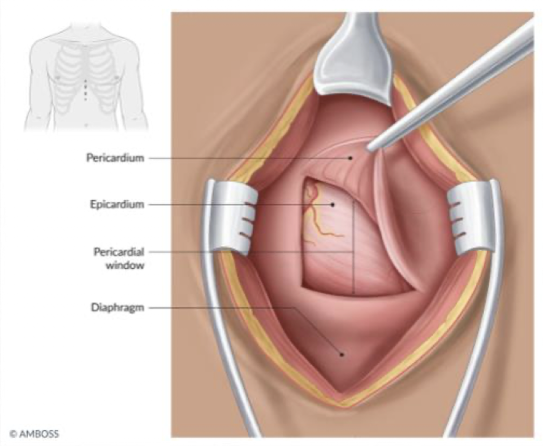
Cardiac Tamponade Medical and Nursing Management
Puncture of the sac to aspirate pericardial fluid (pericardiocentesis)
During procedure
Vital signs
Hemodynamic pressures
Emergency resuscitation equipment should be readily available
HOB elevated 45 to 60 degrees
Peripheral IV line
Complications of pericardioventesis
Ventricular or coronary artery puncture
Arrhythmias
Gastric puncture
Myocardial trauma
Aftercare
Monitor: HR, BP, venous pressure, heart sounds
Pericardiotomy can also be done for recurring cardiac tamponade to allow fluid to drain off (pericardial window)
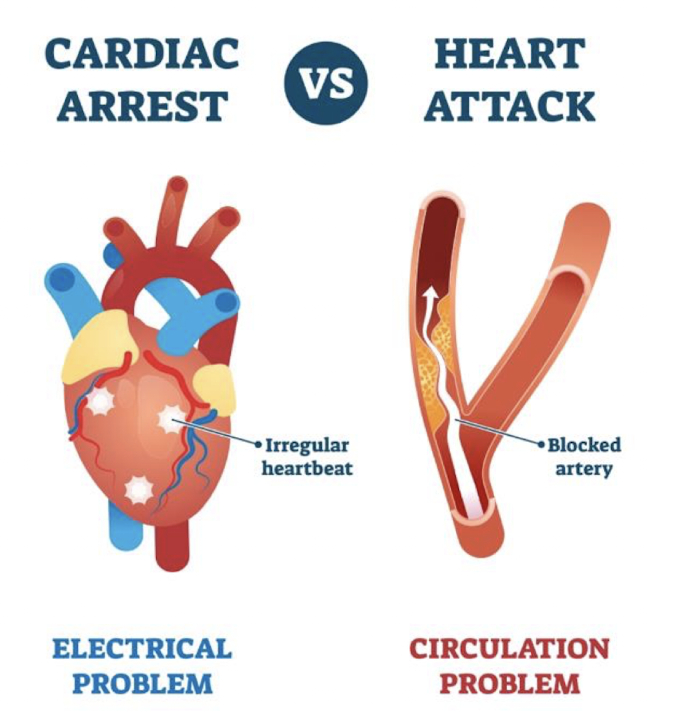
Cardiac Arrest
Normal Cardiac Physiology
Myocardial cells
Create and transport electrical potential (action potential)
Automaticity
Excitability
Conductivity
Contractility
Electrical conduction
Impulses begin in the SA node
Conducts through the atrium (P wave)
Through the atrioventricular (AV) node, propagation slows: PR interval
Bundle of his
Right and left branches
Purfinjine fibers
Right and left ventricles contract: QRS complex
Ventricles depolarize; T wave
Late ventricular depolarization: U wave
Cardiac Arrest Risk Factors
CAD- a build-up of plaque in your arteries may cause them to narrow, obstructing blood flow to the heart
CHD-
Structural heart changes
Family history
Biological female/ children
Cardiac Arrest Causes
Primary
Problem with the cardiac conduction system
Secondary
A condition unrelated to the conduction system impairs the heart's ability to fire and conduct impulses
5 HS and 5 TS
Cardiac Arrest Pathophysiology
Cessation of electrical activity
Ventricles are unable to depolarize and contract
Blood isn’t pumped to the body
Body tissues deprived of oxygen and nutrients
Complications
Brain damage
Death
Cardiac Arrest S/S and treatment
s/s
Sudden collapse
Loss of consciousness
Unresponsive
Apnea
Pulseless
No recordable blood pressure (BP)
Treatment
CPR
Iv epinephrine
H’s & T’s management
Cardiac Arrest Care
Goal of care
Restore perfusing rhythm
Call for assistance
Begin CPR
Admnister 100% oxygen and epinephrine
Assess for signs of return of spontaneous circulation (ROSC)
Provide post-cardiac arrest care
Coordinate transfer to the intensive care unit