locomotion
3 fundamental types of movement
ambulation: brainstem (subconscious adaptation) and SC (reflexive)
posture: brainstem
reach/grasp: cerebral cortex
locomotion vs. ambulation: locomotion is how we move our body through space in whichever way is most efficient vs ambulation is walking
3 motor control requirements of ambulation
progression: moving body/COM in desired direction
postural control: maintain appropriate posture and dynamic stability to generate movement in a meaningful way
adaptation: to meet goals of individual and demands of environment/task
motor control of ambulation: descending control
cerebral cortex
provides a goal
control of overall movement plan
lateral corticospinal tract: goal directed motor program
medial corticospinal tract: posture through neck & trunk
brainstem (descending tracts)
posture and gross limb movements
reticulospinal: adjusts strength of muscle contractions
lateral & medial vestibulospinal tracts
basal ganglia (modulator)
force, amplitude, coordination modulation
cerebellum (modulator)
timing, coordination, error correction
spinal cord
stepping pattern generators (reflexive patterns) in lumbosacral
sensory information
adapt motor output related to environmental conditions (afferent input)
descending input pathway
supraspinal input from the brain (descending control)→spinal cord→reflex and central pattern generator→effector muscles
afferent input contributes to reflex arc and continues up to the brain
stepping pattern generators
ipsilateral side: flexor activated=extensor inhibited; extensor activated=flexor inhibited
contralateral side: flexor activated on IL=flexor inhibited on CL; extensor activated on IL=extensor inhibited on CL
IL flexors activated=extensors activated on CL side
cycles of these 2 SPGs coordinated by signals in anterior commissure of spinal cord
basic rhythmicity of stepping is produced by neuronal circuits contained entirely within SC
afferent input is processed at SC: joint position during swing, loading response during stance (via GTO)
descending input helps modulate and refine SPG movement
descending command centers=plans for and adjusts movement (ex. vision): environment and timing
afferent input to SC=proprioception and loading—not necessarily relying on input to initiate gait
terminal stance facilitates the transition from stance to swing
gait initiation
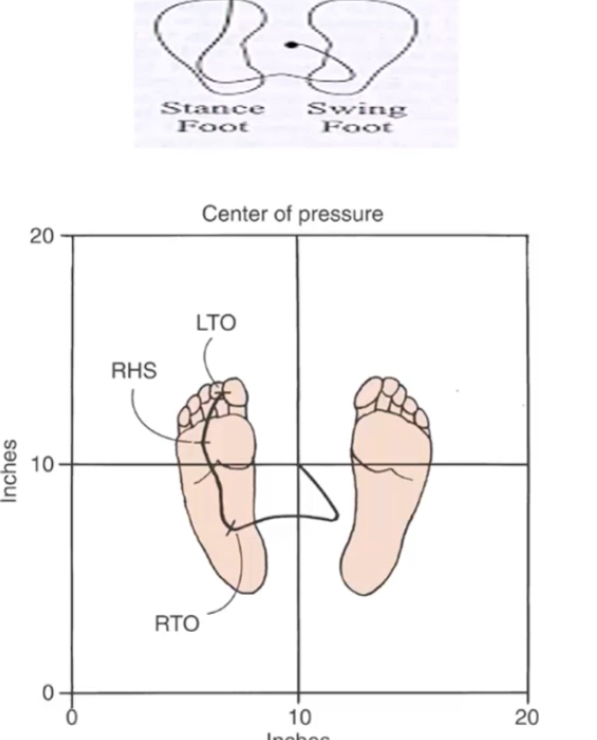
COP moves posterior & lateral over swing limb: bilateral ankle strategy against backward sway (TA, quads)
COP shifts toward stance limb and forward: TA causes DF in stance ankle→pull shank over foot as body moves forward in preparation for toe off
steady state velocity reached within 1-3 steps
not seen consistently in children until 4-5 y/o
adaptation
SPGs are adaptable
spontaneous recovery of SPGs
experience dependent adaptive neuroplasticity of SPGs
low variability—not able to adapt to environment very well (stepping over/around objects)
can train/modify coordinated control
stairs
adapting to environment (steps)
requires feedforward (descending) and feedback (afferent) pathways for adaptation
SPG alone are not sufficient to produce stair climbing
movement patterns/strategies
step to pattern
reciprocal pattern
2x greater forces and ROM needed compared to level ground walking
ascent: force generation is 2x> concentric quads/knee extension
descent: GRF=2x BW with WA on descent (quads, gastroc)
ascent phases
stance: WA, pull up, forward continuation
swing: foot clearance, foot placement
descent phases
stance: WA, forward continuation, controlled lowering
swing: leg pull-through, preparation for foot placement
development of ambulation
stepping patterns
present in newborns
disappears ~2 mo
reappears
assisted ambulation ~10 mo
progress to indep walking ~12 mo
infant stepping
increased hip flex, fwd trunk lean, co-contraction
forward and backward progression of knee, rapid COM progression, stagnant & vertical movement in COM, excessive foot clearance
adult stepping
normalization of hip flex/upright trunk posture
reciprocal pattern of muscle activation, linear pattern
healthy older adults >65 yo
slower speeds, decr stride length, vertical head movement smaller, lateral movement larger
aging or pathology?
fall risk: gait variability, changes in feedback/reactive control
cognitive factors
sensory impairments (vision, proprioception, vestibular)
decr muscle strength
studies show excs can improve amb fx in OAs
walking speed: functional vital sign
not a great measure of ability to walk
related to mortality rate
is pt likely to walk safely only at home b/c they walk slow, or are they likely to be more able to get around community in short distances or are they truly community ambulatory (requires greater gait velocity ex. crossing the street)
considerations with impairment of neurologic system
decreased automatic processing of ambulation: motor or sensory impairments
cognitive processing impairments (attention)
decreased capacity for appropriate attention to ambulation
decreased ability for appropriate selection of attention on tasks
effects on ambulation
decreased gait speed, increased DL support, decr stride length, incr variability—regardless of pathology, all can be expected with any neuro pathology