BPH
Obstructive vs Irritative symptoms
Obstructive | Irritative |
physical blockage or narrowing of urethra from enlarged prostate | overactive bladder symptoms from irritation of bladder muscle |
hesitancy | urgency |
straining | frequency |
weak urine stream | nocturia |
post-void dribbling | bed or clothes wetting |
bladder full after voiding | |
decreased bladder emptying |
Dynamic vs Static Factors
Dynamic | Static |
narrowing of the urethral lumen | enlargement of prostate gland |
excess α-adrenergic tone in stromal tissue increasing smooth muscle tone and contraction of bladder neck in urethra | testosterone/DHT stimulation of epithelial tissue |
Laboratory/diagnostic tests for screening
Lab Test | Results |
American Urological Association | mild <7 moderate 8-19 severe 20+ questionnaire |
Urinalysis | rules out infection/stones |
Prostate Specific Antigen (PSA) | patients in 40+ years old with 10 year life expectancy normal < 1-1.5 ng/mL |
Digital Rectal Exam (DRE) | assess size and shape of prostate normal <20 g |
Transrectal Ultrasound (TRUS) | radiologic and imaging |
Post-void Residual (PVR) | normal < 50 mL left in bladder post pee 300+ mL refer to urologist |
Uroflowmetry | urine voided per sec |
Medications that worsen BPH
Class | Examples | How |
Sympathomimetics | decongestants (α1 adrenergic agonists) antihypertensives (α2 adrenergic agonists) | more contraction less flow |
Opioids | increases sphincter tone increasing PVR | |
Diuretics | loop and thiazide | more urine increasing frequency and urgency |
Anticholinergics | antihistamines tricyclic antidepressants antipsychotics muscle relaxants antispasmodics | less bladder contraction increases PVR |
Testosterone Products | increase prostate growth |
Explain the MOA of 5 α-reductase inhibitors, α1 adrenergic receptor antagonists, and PDE5 inhibitors
Class | MOA | best patients | Monitoring | Notes | Patient counseling |
α1-Adrenergic Receptor Antagonists | smooth muscle relaxation of prostate bladder neck and urethra | reduces dynamic factors in moderate (AUA 8-19) symptoms | takes 1-6 weeks to see benefit of symptom relief lowest dose at night and increase weekly monitor BP and HR | a1A prostate and urethra desired effects a1B vascular smooth muscle may cause orthostatic hypotension or syncope a1D only bladder | Orthostatic Hypotension
Intraoperative floppy iris syndrome
Hypotension
Priapism
|
5 α-Reductase Inhibitors | inhibit conversion of inactive testosterone to active dihydrotestosterone DHT | reduces static factors in moderate symptoms | best in patients with prostate 30+ g decrease PSA levels by 50% and prostate size by 25% over 6 months monitor PSA | correct PSA by doubling measured PSA after 6 months to approx true | Pregnancy category X
ask doctor to order PSA level before starting Side Effects
|
PDE5 inhibitors | smooth muscle relaxation of prostate, bladder neck, and prostate urethra | reduce dynamic factors in moderate symptoms | monitor BP pulse and hearing | metabolized by CYP3A4 so avoid medications that are inhibitors | Do not take with nitrates
Side effects
|
Compare the distribution of 5 α-reductase enzyme and α1-adrenergic receptors in BPH and how that corresponds to response in therapy
Normal Prostate | BPH |
2 stromal to 1 epithelial | 5 stromal to 1 epithelial |
more 1α than 5α (DHT) | even more 1α than 5α (DHT) more narrowing |
Nonpharm
Healthy Lifestyle | Patient Education |
low-fat diet with high fruits and vegetables | restrict fluid close to bedtime empty bladder often while awake |
regular physical exercise stop smoking | minimize caffeine, alcohol, drugs that worsen voiding symptoms |
Match brand/generic and class of drugs used for treatment of BPH
Drug (Generic) | Brand Name(s) | Class | Dose | Other |
|---|---|---|---|---|
Finasteride | Proscar, Propecia | 5α-reductase inhibitor | 5 mg PO Qday | inhibit type 1 sebaceous glands FDA alopecia |
Dutasteride | Avodart | 5α-reductase inhibitor | 0.5 mg PO Qday | inhibit type 1 and 2 sebaceous glands and prostate and genital tissue tamsulosin combo Jayln |
Tamsulosin | Flomax | 3rd Gen α1A-adrenergic antagonist | 0.4 or 0.8 mg Qday | off-label nephrolithiasis Caution in sulfa allergy take 30 min after a meal do not crush or chew |
Silodosin | Rapaflo | 3rd gen α1A-adrenergic antagonist | 8 mg Qday | if CrCl 30-50 mL/min or hepatic impaired 4 mg If CrCl < 30 mL/min contraindicated |
Prazosin | Minipress | 2nd Gen α1-adrenergic antagonist | 0.5-5 mg BID | FDA HTN off-label BPH |
Terazosin | Hytrin | 2nd Gen α1-adrenergic antagonist | 1-20 mg Qday | FDA also HTN |
Doxazosin | Cardura | 2nd Gen α1-adrenergic antagonist | 1 - 8 mg Qday | FDA also HTN XL OROS ghost tablet in poop |
Alfuzosin (most uroselective) | Uroxatral | 2nd Gen α1-adrenergic antagonist | 10 mg Qday | do not crush or chew prolongs QT interval bradycardia caution in CrCl < 30 mL/min |
Tadalafil | Adcirca | PDE5 inhibitor | 40 mg PO Qday | BPH and pulmonary HTN |
Tadalafil | Cialis | PDE5 inhibitor | 5 mg PO Qday | BPH and erectile dysfunction |
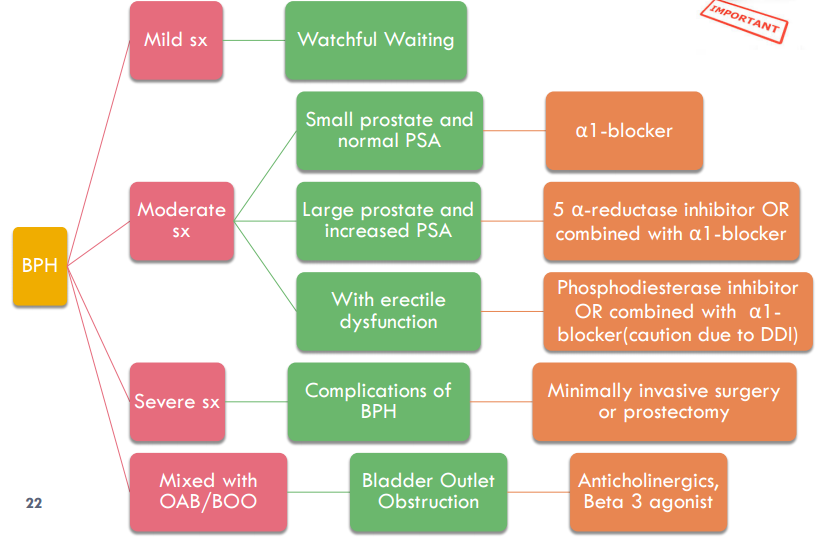
List treatment options in BPH based on severity of symptoms (According to AUA guidelines)
Uroselective and their advantage over non-uroselective agents
Uroselective (α1A selective): Tamsulosin, Silodosin, Alfuzosin (most uroselective among 2nd gen)
Advantage: Lower risk of orthostatic hypotension and cardiovascular side effects compared to non-uroselective agents.
Differentiate between different pharmacological classes used for treatment of BPH in terms of adverse effects, onset, effect on PSA/prostate size, monitoring parameters, and halting disease progression
Class | Onset | Prostate Size/PSA | Adverse Effects | Disease Progression | Monitoring |
|---|---|---|---|---|---|
α1-blockers | 1–6 wks | No effect | Orthostatic hypotension, dizziness, IFIS, priapism | No | BP, HR, symptoms |
5α-reductase inhibitors | 6–12 mo | ↓ size, ↓ PSA | ED, decreased libido, gynecomastia | Yes | PSA, DRE |
PDE5 inhibitors | 4 wks | No effect | Headache, flushing, hypotension | No | BP, symptoms |
Describe the role of anticholinergics/antispasmodics in BPH (side effect vs. therapeutic use)
Drug | Brand | Formulation | Dosing |
Darifenacin | Enablex | Oral tablet | 7.5-15 mg Qday |
Fesoterodine | Toviaz | Oral tablet | 4 - 8 mg Qday |
Solifenacin | Vesicare | Oral tablet | 5-10 mg Qday |
Oxybutynin | Ditropan Ditropan XL Oxytrol Gelnique | Oral tablet/syrup Oral tablet TD patch Topical gel | 5-10 mg BID/TID 5-30 mg Qday 1 patch Q4D 3 pump Qday |
Tolterodine | Detrol Detrol LA | Oral tablet Oral Capsule | 2 mg BID 4 mg Qday |
Trospium | Sanctura Sanctura XR | Oral tablet Oral capsule | 20 mg BID 60 mg Qday |
Therapeutic use: For patients with mixed symptoms of BPH and overactive bladder (OAB), anticholinergics or beta-3 agonists may be added. block receptors to inhibit contraction of the detrusor muscle
Side effect: Anticholinergics can worsen urinary retention and are generally avoided unless OAB symptoms predominate. should not be used in patients with PVR > 250 mL