7. Emily Wilkins - A Case of Falls
Pre-reading - Session 1
Anatomy Videos
Anatomy of the hip joint
Joint between the head of the femur and the acetabulum of the pelvis
Acetabulum is the name of the articulating surface for where the pelvis attaches to
Hip joint is a ball and socket joint
Ball - ball of the hip joint
Socket - acetabulum of the pelvis
Hip joints can perform flexion and extension
Flexion - raising the thigh upwards
Etension - bringing the thigh back down to standing position
Abduction - taking the lower limb away from the midline (outwards)
Adduction - taking the lower limb back towards the midline (inwards)
Rotation - two types: external and internation
External - lateral movement of the head of the femur within the acetabulum (used when crossing the legs)
Internal - medial movement of the head of the femur within the acetabulum (return thighs after having crossed legs)
Circumduction - flexion, extension, abduction, adduction, external and internal rotation put together
Circumduction can only happen at the hip and the shoulder
Free range of movement means there is a compromise in the stability (more mobile = less stable)
However hip joint is more stable than the shoulder joint - important because hip joint is a weight bearing
Features of the Femur:
Head of the femur forms the ball aspect of the hip joint
Neck of the femur connects the head to the shaft of the femur
Slightly diferent angle to the shaft
Two lumps of bones called trochanter
Large trochanter - greater trochanter
Lesser trochanter is lower than the greater trochanter
Trochanter - bony process which serves as an attachment for the muscles which move the hip joint
Inter-trochanteric line - ridge of bone which joions the greater and lesser trochanter together
Joint capsule - increases stability of the hip joint
Connective tissue sheath wrapping around head and neck of the femur and attaches to the outer rib of acetabulum
Serves to pull the head of femur into the acetabulum providing stability and preventing dislocation
Joint capsule attaches just above the intertrochanteric line
Blood Supply to the hip joint
Arises from the femoral artery
Pulse can be felt in the groin region
Femoral artery branches in the profunda femorus (deep femoral) artery
Arising from the profunda femorous is the lateral and medial circumflex artery - wraps around the hip joint to provide circular blood flow.
Circumflex artery travels upwards (instead of travelling distally)
Retrograde blood flow - arteries travel upwards back towards the proximal blood supply
Arteries supply the head and the neck of the femur and the vessels lie within the joint capsule itself.
Lecture - Session 2
Task 1
When to suspect delirium
Behaiour changes that develop acutely (hours to days)
Behaviour changes include:
Altered cognitive function
Inattention
Disorganised thinking
Altered perception, physical funciton, social behaviour and level of conciousness
Diagnosing delirium
Use the CAM criteria for delirium
Confusion - developed suddenly
Inattention - ask if the patient is easily distracted or has difficulty focusing
Disorganised thinking - ask if the person’s thinking is disorganised, incoherent, illogical or unpredictable
Altered level of conciousness - ask about changes in level of conciousness from alertness to lethargy (drowsiness, stupor, comatose or hypervigilance).
Types of delirium
Hyperactive - inappropriate behaviour, hallucinations or agitations
Hypoactive - lethargy, reduced concentration and reduced appetite
Predisposing risk factors
Age (>65)
Pre-existing cognitive impairment
Previous delirium
Poor mobility
Severe current illness (hip fractures/emergency)
Visual or hearing problems
Drugs (sedatives, steroids, antidepressants can all make people more drowsy)
Social isolation and substance misuse
Triggers for Delirium
Infection
Drugs - opiod analgesics, steroids and sedative
Surgery
Substance misuse or withdrawal symptoms from addictive drugs and alcohol
Vtiamin deficiencies
Intra-cerebral trauma from head injury or stroke
Task 2
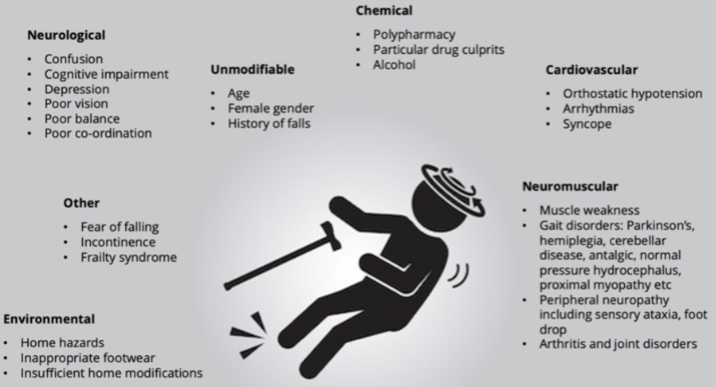
Risk factors for falls in the elderly
Task 3
X-rays and 4 diagnoses
Mrs J - normal X-ray
Mrs L - extracapsular necofemur fracture
Mr K - around the neck of the femur and on the right
Extracapsular vs Intracapsular
Everything from the neck and up is intracapsular
Everything from below the neck of the femur is extracapsular