Familial Hypercholesterolaemia (FH) (Class Test)
Blood containing high cholesterol has lipemic rather than clear serum meaning the serum is opaque.
Atherosclerosis is where atheroma/atheromatous plaque deposits are laid down on vascular walls. These deposits are made of macrophages, debris and cholesterol. They’re covered with a fibrous cap. When the fibrous cap of atheromatous plaque bursts, macrophages, debris and cholesterol are released and block capillaries. This can cause ischaemia and stroke or myocardial infarction.
The NHS list of symptoms for heart attack includes chest pain, pain in other body parts, lightheaded/dizziness, sweating, short breath, nausea, vomiting, feelings of anxiety, coughing/wheezing.
Treatment time for MI critical. Proteases used to dissolve blood clots, or surgery eg stents/angioplasty/bypass. These treatments are important to restore blood to the heart.
Risk factors for CHD include high blood pressure, cholesterol and triglycerides. Smoking, insulin resistance, obesity, diabetes and inflammation.
Chronic NSAID drug use is NOT a CHD risk factor for CHD.
Cholesterol is a key molecule in our bodies, it is when cholesterol levels become too high that it is an issue. Its physiological functions include cell membrane structure, bile acid production and being a precursor for steroid hormones eg progesterone/oestrogen and vitamin D. It also is a key component of Schwann cells.
Humans can synthesise cholesterol de novo with liver and intestine production accounting for 10% of total body cholesterol each. The rest is obtained from the diet. Dietary cholesterol and triglycerides are packed together with apo proteins in the liver and released into circulation as VLDLs so they can be transported in the blood. Triglycerides in VLDLs are degraded forming cholesterol rich LDLs. LDLs are recognised by LDL receptors on peripheral cell membranes and endocytosed. HDLs carry cholesterol from peripheral tissues to liver to remove excess cholesterol.
The rate limiting step in cholesterol synthesis is the conversion of HMG CoA into mevalonate by HMG CoA reductase. Statins competitively inhibit HMG CoA reductase and are prescribed to around 8 million in the uk.
Familial hypercholesterolaemia is genetic meaning it doesn’t occur as a result of diet etc. It is a genetic condition causing abnormally high cholesterol levels. It is an autosomal dominant trait. One copy of the mutated gene elevates cholesterol meaning the person is at risk of a heart attack in their 30s to 50s. Two copies causes highly elevated levels so the person is at risk of heart attack in childhood to 30s. LDL above 190 mg/dl is diagnostic for FH.
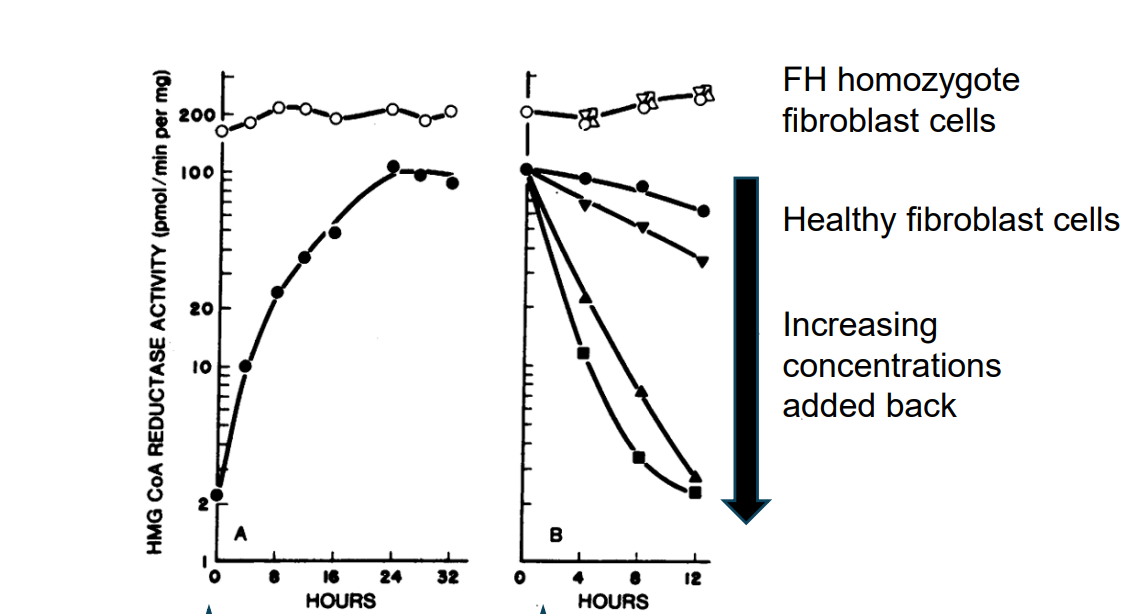
1st graph shows the removal of LDL/cholesterol from the media and 2nd shows reintroduction of LDL/cholesterol. Shows that as LDL/cholesterol conc increases in healthy cells, HMG-CoA reductase activity is reduced - negative feedback. However but enzyme activity remains high in FH individuals no matter what the cholesterol concentration is - it is not affected. Substrate binding is the same in both FH and WT individuals - the enzyme itself is not mutated. Most cases of FH are due to a mutation in the gene for receptors which bind LDL meaning cells don’t recognise that there is a high concentration of LDL. This means internalisation of LDL doesn’t occur, lysosomal hydrolysis doesn’t happen and no regulatory actions to reduce LDL eg reducing HMG CoA reductase doesn’t happen (no negative feedback mechanism).