t7c: Miotics and Prostaglandins
Overview of Aqueous Outflow Medications
Two main classes: Miotics and Prostaglandins - INCREASE AQUEOUS OUTFLOW
Key learning outcomes:
Understand the pharmacology, uses, and side effects of each class
Compare effectiveness of different agents
Select appropriate agent for intended use
Miotics
Pilocarpine
Pilocarpine hydrochloride 1%, 2%, 4%
Brand names: ISOPTO CARPINE, PILOCARPINE, PILOT, PV CARPINE
Packaging: 15 ml, containing benzalkonium chloride as a preservative. 5 repeats costs px up to $25 per bottle.
Dosage: One drop 4 times daily; effects last 4-8 hours
Minims (Single-dose): Pilocarpine nitrate 2%, 4%
Mode of Action
Directly acting parasympathomimetics (cholinergic agonists)
Bind to acetylcholine receptors on the iris sphincter and ciliary muscle
Mimic acetylcholine effects, causing:
Contraction of longitudinal muscle fibres in the ciliary muscle
Opening of the Trabecular Meshwork
Increased aqueous outflow
Clinical Uses
Acute Angle Closure Glaucoma: emergency treatment
Administer 2% pilocarpine every 5 minutes until miosis achieved
Contraindications for concentrations >2% due to risks
No more effective than 2% and can cause further shallowing of the anterior chamber intensifying the pupil block and leading to permanent PAS and permanent angle closure
If IOP >50-55mmHg pilocarpine ineffective due to ischaemia of the iris sphincter
Open-Angle Glaucoma:
Reduces IOP by contracting ciliary muscle which exerts a force on the scleral spur and stretches the trabeculae
Reduces IOP by %20-25 by reducing resistance to outflow
Works by contracting ciliary muscle
Effects generally last 6 hours; other agents are preferred for long-term use
Should only use 1% in fair skinned individuals and 2% in dark skinned individuals - gets pigment bound
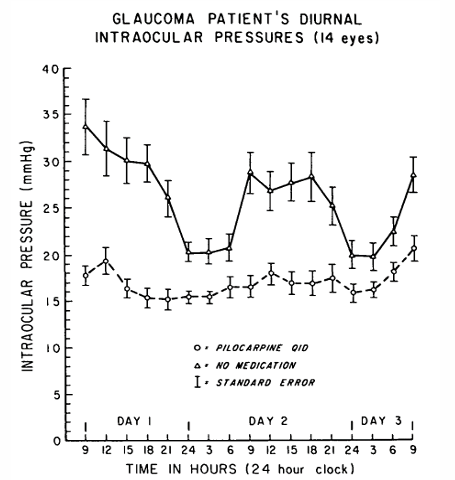
IOP Effects
Reduces IOP significantly (e.g., from 26 to 17 mmHg)
Decreases maximum diurnal variation from 18.5 to 8.5 mmHg
Side Effects
Ocular:
Accommodative spasm causing brow ache, pseudomyopia (myopic shift)
miosis, dim vision for night driving
pupil block glaucoma
Conjunctival injection, allergic blepharoconjunctivitis
Rarely cataract and retinal detachment
Systemic:
Bronchoconstriction (respiratory distress in asthmatic patients)
gastrointestinal upset (nausea, vomiting, diarrhea)
increased salivation
CNS effects
Contraindications
Ocular: PSCC, neovascular and uveitic glaucoma, history of retinal detachment
Systemic: age under 40, pregnancy, asthma, peptic ulcers, Parkinson’s disease
Prostaglandin Analogues/Prostamides
Commercial Preparations
Latanoprost 0.005% (e.g., XALATAN)
Travoprost 0.004% (e.g., TRAVATAN)
Bimatoprost 0.03% (e.g., LUMIGAN) - only amide based (all other are esters)
Tafluprost 0.0015% (e.g., SAFLUTAN)
Dosage: Typically administered once daily, more effective at PM than AM
Common effect: increases uveoscleral outflow; peak IOP reduction lasts 8-12 hours
peak effect: one month
packaging: Xalatan and Saflutan require refrigeration Lumigan and Travatan at room temperature
Pharmacology of prostaglandins
Prostaglandins are naturally occurring compounds in the body.
They are synthesised following injury and play a role in the inflammatory response.
In 1981, it was observed that administering PG F2α to monkeys resulted in decreased intraocular pressure (IOP).
Natural PG F2α in the body also causes pain, headaches, and conjunctival hyperaemia.
Modifications have been made to create prodrugs with improved effect profiles.
These prodrugs have good corneal penetration and are fully hydrolysed to active acid forms as they pass through the cornea, making metabolism easier.
Latanoprost and travoprost act on PG FP receptors located on ciliary muscle cells.
The exact mechanism of their impact on uveoscleral outflow is unknown but is believed to involve transient changes in the extracellular matrix of the ciliary muscle.
Prostaglandins (PGs) are produced by cells within the outflow pathway of the human eye eg trabecular meshwork cells
PGs have a role in the normal regulation of aqueous outflow.
Minute amounts of topical exogenous PGs can reduce intraocular pressure (IOP) without causing inflammation.
Pathway / mechanism of action
The prostaglandin F2 (PGF2) analogues (eg latanoprost) act through FP and cause a COX2-dependent increase in prostaglandin E2 (PGE2) and matrix metalloproteinases (MMPs) levels which in turn cause tissue remodelling.
Prostaglandins activate a molecular transduction cascade that leads to increased biosynthesis of matrix metalloproteinases.
These proteinases cleave extracellular-matrix (ECM) components, such as collagen, within the ciliary muscle and sclera
The resulting reduction of the extracellular matrix may contribute to the mechanism of increased uveoscleral outflow
Mechanism of Action (summary)
Bind to FP receptors on ciliary muscle cells
Increase biosynthesis of matrix metalloproteinases (MMPs)
Cause extracellular matrix remodelling, enhancing aqueous outflow
Latanoprost (Xalatan)
selective prostanoid FP-receptor agonist that reduces intraocular pressure (IOP) by increasing the outflow of aqueous.
Onset of Action: Reduction of IOP starts within 3 to 4 hours after administration with peak concentration in the aqueous humor occurring in about 2 hours.
Maximum Effect: Maximum reduction in IOP is reached after 8 to 12 hours and is maintained for at least 24 hours.
Mechanism of Action: The main mechanism involves increased uveoscleral outflow, with some reports of increased outflow facility (decreased outflow resistance).
Aqueous Production: Latanoprost does not significantly affect aqueous production or the blood-aqueous barrier.
Systemic Effects: At clinical doses, it has not shown significant pharmacological effects on the cardiovascular or respiratory systems.
Repeats: latanoprost 0.005% eye drops, 2.5 ml x 5 (cost $22.58)
Contraindications: use in pregnant women is limited due to high incidence of abortion shown in animal experiments.
Travoprost (e.g. Travatan)
Bimatoprost is an ester prodrug of a prostaglandin F2alpha analogue.
It is hydrolyzed to the free acid as a full agonist of the prostaglandin FP receptor.
Reduces intraocular pressure (IOP) by increasing outflow via uveoscleral pathways and trabecular meshwork.
Onset of Action: IOP reduction starts about 2 hours after administration.
Maximum Effect: Maximum effect is reached after 12 hours.
Duration of Action: Significant lowering of IOP can be maintained for periods exceeding 24 hours with a single dose.
repeats: travoprost 0.004% eye drops, 2.5 mL x 5 (cost $39.50)
Bimatoprost (e.g. Lumigan)
Bimatoprost is a synthetic prostamide analogue that selectively mimics the effects of naturally occurring prostamide.
It is biosynthesized through a COX-2 pathway, leading to the synthesis of endogenous lipid amides that lower intraocular pressure (IOP). Bimatoprost reduces IOP by enhancing uveoscleral outflow and increasing aqueous humor outflow through the trabecular meshwork.
Onset of Action: Reduction of IOP starts approximately 4 hours after the first administration.
Maximum Effect: Maximum effect is typically reached within 8 to 12 hours.
Duration of Action: The reduction in IOP is maintained for at least 24 hours.
repeats: bimatoprost 0.03% eye drops, 3 mL x 5 (cost $39.50)
Minims: bimatoprost 0.03% eye drops, 30 x 0.4 mL unit doses
Tafluprost (Saflutan)
12 x greater prostaglandin receptor-binding affinity than latanoprost
no real evidence that it is superior to the older agents
advantage: comes in preservative free form
Minims: 15 μg per mL (0.0015%), single dose units, 30 × 0.3mL unit doeses x 5 repeats (cost $39.50)
Clinical Use and Effectiveness
Average IOP reduction:
Latanoprost: 27%
Travoprost: 31%
Bimatoprost: 33%
Not effective for about 10-15% of patients
Travatan ~9%
Xalatan ~14%
Timolol ~23%
other prostaglandins may still be effective.
Patients with IOP in high teens may respond with IOP reduction up to 30%
In NTG, IOP reduction by ~20% with latanopros
Only glaucoma medication class with no cross over effect in non-treated eye
if you treat one eye, there is no effect in IOP in the other.
Prostaglandins: Comparison to Timolol
Early studies compared Prostaglandins to Timolol (the then gold-standard)
Xalatanbetter than Timolol bd when directly compared (35% vs. 27%)
69% on Xalatan vs. 34% using Timolol had IOP <18 mmHg
Lumigantwice more likely to achieve an IOP <15mmg than Timolol
Effective in CNAG (chronic narrow angle glaucoma):
Better IOP control than Timolol (8.8mmHg vs. 5.7mmHg reduction)
Side Effects
Ocular:
Conjunctival hyperemia
iris pigmentation/heterochromia
More pronounced in blue, green, hazel eyes: irreversible increase in the size of the iris melanocytes
Hypertrichosis – longer, thicker, darker, more curled, distichiasis
Epithelial erosion, hypertrichosis, periorbital pigmentation, cystoid macular edema
stinging, burning
foreign body sensation
Systemic:
Rare headaches, respiratory symptoms, skin rash, diarrhea
Contraindications
Local: history of uveitis, cystoid macular oedema, herpes simplex keratitis, complicated cataract surgery
inflammatory glaucoma
no systemic contraindications
interactions:
topical NSAIDs have antagonistic effect
If used concurrently the effectiveness of prostaglandins is decreased by up to 30%
Summary of Comparisons
Travoprost is most effective for lowering IOP in African Americans
Lumigan has the greatest initial redness followed by Travatan
Xalatan has greatest periorbital pigmentation and greatest iris pigmentation at 6 months
Xalatan ~ 6.7% and ~16.1% at 12/12
Travatan ~ 3.1%
Lumigan~ 1.2% and ~1.5% at 12/12