Psychosis
What is Psychosis?
- no single diagnosis of ‘psychosis’
- psychotic episodes are core to some diagnoses like schizophrenia and delusional disorder
- psychosis can be diagnosed as an optional part of other disorders → e.g., bipolar disorder
Symptoms
- Delusions
- A delusion is where a person has an unshakeable belief in something implausible, bizarre, or obviously untrue
- The concept of delusion is that the process of belief formation and updating isn’t functioning correctly.
- Following Jaspers (1913), delusion is defined as a belief that is has the following characteristics:
- certainty → (held with absolute conviction)
- incorrigibility → (not changeable by compelling counterargument or proof to the contrary)
- impossibility or falsity → (implausible, bizarre, or patently untrue)
- Types of delusion
- Erotomanic: The person believes someone is in love with them and might try to contact that person. Often it’s someone important or famous. This can lead to stalking behavior.
- Grandiose: This person has an over-inflated sense of worth, power, knowledge, or identity.
- Jealous: A person with this type believes their spouse or sexual partner is unfaithful.
- Persecutory: Someone who has this believes they (or someone close to them) are being mistreated, or that someone is spying on them or planning to harm them. They might make repeated complaints to legal authorities.
- Somatic: They believe they have a physical defect or medical problem.
- Mixed: These people have two or more of the types of delusions listed above.
- Delusional themes
- Delusion of external control of thoughts or actions → (particularly associated with schizophrenia)
- Somatic delusions → (alterations to the body)
- Delusions of reference → (the news is about me etc)
- Misidentification delusions → (seemingly rare)
- Hallucinations
- seeing, particularly hearing, or feeling things that aren’t really there → related to the delusion
- hallucinated voices (auditory verbal hallucinations)
- Stereotypically the experience of ‘a voice talking to you’ but phenomenological studies show it to be far more complex (Woods et al., 2015)
- Commonly involves the experience of being communicated to by a character or persona
- Often not a clear auditory experience
- Often accompanied by other voices and hallucinated sounds
- Hallucinations may occur with or without insight into their hallucinatory nature
- the absence of insight defines it as a psychotic symptom
- Impaired self-awareness of disease, termed “insight” into illness.
- This means that patients commonly do not know if they are currently experiencing an episode of psychosis, or they do not attribute psychotic delusions to having the disease.
- Disorganised thought, speech or behaviour
- known as formal though disorder
- detected as a language disorder
- ranges from tangential (diverging from a previous course or line) to ‘word salad’
- ‘Negative symptoms’ → most associated with the diagnosis of schizophrenia
- Negative symptoms → associated with features that are no longer present or are lacking
- Emotional blunting → inexpressiveness and apparent unresponsiveness
- However, studies on people diagnosed with schizophrenia show:
- …reduced emotional expressions
- …normal levels of pleasure and normal levels of negative emotion to unpleasant stimuli (Cohen and Minor, 2010)
- …increased negative emotion to neutral and pleasant stimuli (Kring and Ellis, 2013)
- Poverty of speech
- Apparent lack of desire for the company of others
- Anhedonia → apparent inability to show or feel pleasure
- Reduced motivation
How many people experience psychosis?
- Psychotic experiences → mostly benign and transitory → 8%
- Psychotic symptoms → associated with a degree of distress → 4%
- Psychotic disorder → clear distress and disability → 3%
Population distribution of symptoms
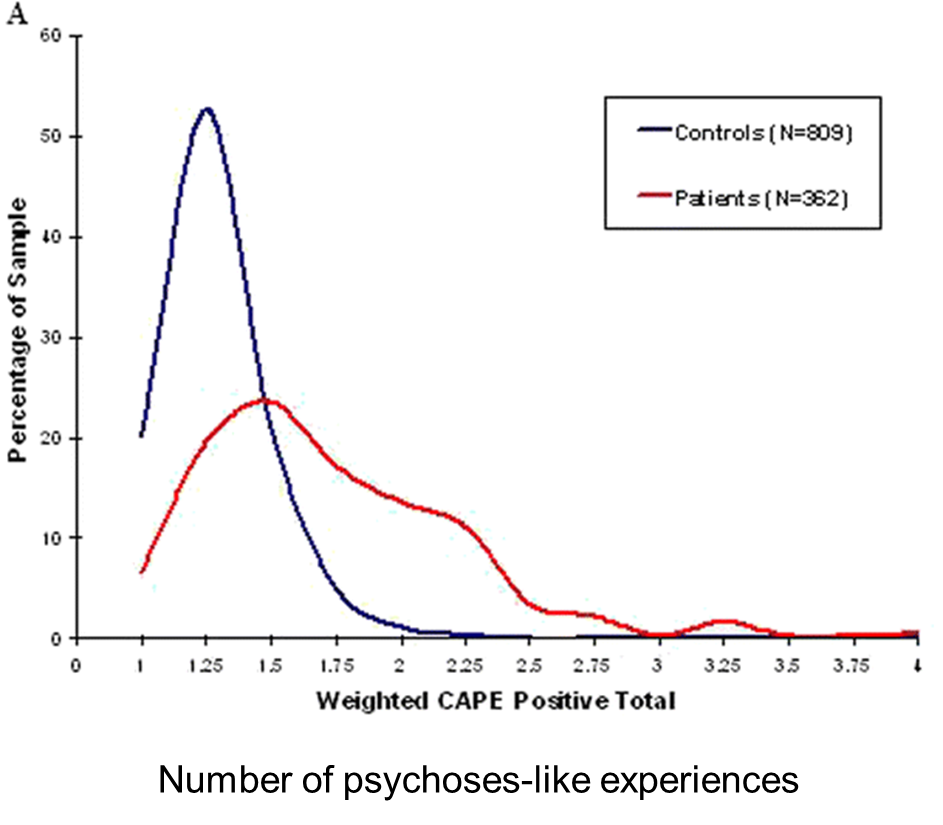
Not all psychosis experiences are equal…
- some people can have limited or brief psychotic experiences
- some people can have experiences that don’t seem to cause distress or disability (like hearing voices)
- however, they tend to become more disabling as they become more tense and/or negative in tone
How does psychosis start and when does it occur?…
- no single way → sometime the onset psychosis happens slowly or rapidly → depends on causes and individual variation
- typical age of onset is between 17-30
- earlier age of onset for males
What causes psychosis?…
- there are a wide variety of causes
- described as a fever of mental health → seems to be the end point of various types of psychological and neurological stresses
- causal pathways (mix of causes) may be different for different people
Drug-causing psychosis
- Purely idiosyncratic reactions → the drug doesn’t raise the risk at the population level but can trigger psychosis in others
- Developental stage specific → e.g. high THC canabis in young people
- Dose dependent → stimulant drugs (e.g. speed, cocaine) and corticosteroids
Damage to nervous system
- Dementia (very common)
- Epilepsy → can be a specific syndromes
- Stroke
- Parkinson’s disease
- Traumatic brain injury
- Mutiple sclerosis
Psychosis without neurological problems
- known as functional psychotic disorders
- Depending on presentation, might be diagnosed as sometime like:
- Schizophrenia
- Schizoaffective disorder
- Bipolar disorder
- Delusional disorder
- Depression with psychotic features
Schizophrenia: Genetics
- lots of debate about the validity of this diagnosis
- Two types of genetic risk:
- Rare mutations
- typically non-inherited
- e.g. 22q11.2 deletion
- uncommon but markedly raises risk of schizophrenia diagnosis
- Effect of combined common genetic variants
- typically inherited
- accounts for most genetic risk
- Schizophrenia shows 80% heredity → 80% of the variance in the risk of schizophrenia in the populations in which it has been studied is accounted for by genetics rather than environmental factors
Schizophrenia: environment
- Risk is raised by
- Childhood trauma and adverse experiences
- Being an immigrant (not a particular ethnicity)
- Living in urban environments Birth complications
- Foetal development problems
- Drug use
Treatment
- Main forms
- Medication → antipsychotics
- Psychological therapy → best evidence for CBT
- Domestic support for people most disabled
- our current treatments help but are limited in their effectiveness
Cognitive and neurocognitive models
- Focus on how the symptoms of psychosis are caused or maintained in terms of cognitive and neural processes
Core findings in psychosis
- People with psychosis reported to show:
- Poorer reality monitoring (keeping track of internally vs externally generated experiences)
- Probabilistic reasoning bias (making decisions on fewer data points)
- Attentional biases (to less relevant information)
- Increased presynaptic dopamine turnover in mesolimbic pathway
Garety et al. (2001) → cognitive model
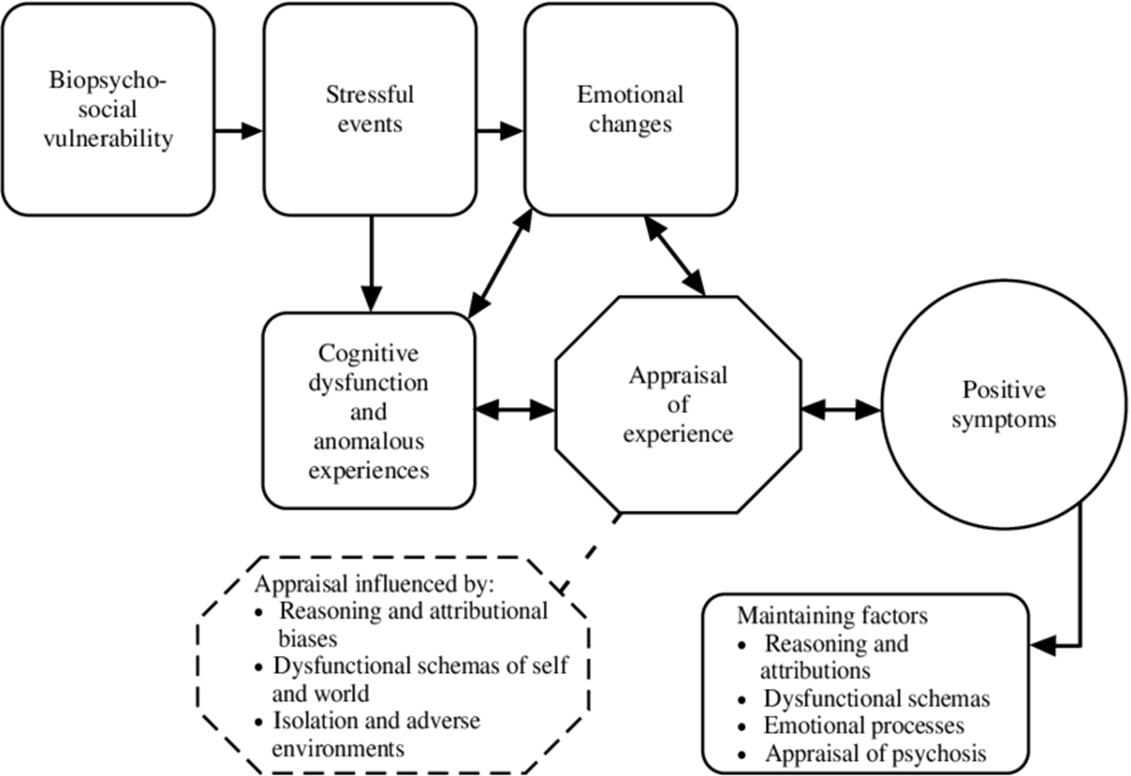
- Designed by and for CBT therapists
- Not framed in terms of normal cognitive function
- Tries to explain maintenance rather than genesis
Aberrant Salience Model of Psychosis
- Often attributed to Kapur (2003) but actually first described several times before (e.g. Spitzer, 1995)
- Misfiring mesolimbic dopamine attributes meaning to otherwise irrelevant stimuli, leading to psychosis.
- However, it’s not clear why this would lead to psychosis, rather than just distraction.
- doesn’t account for the selective content of delusional themes and voices.
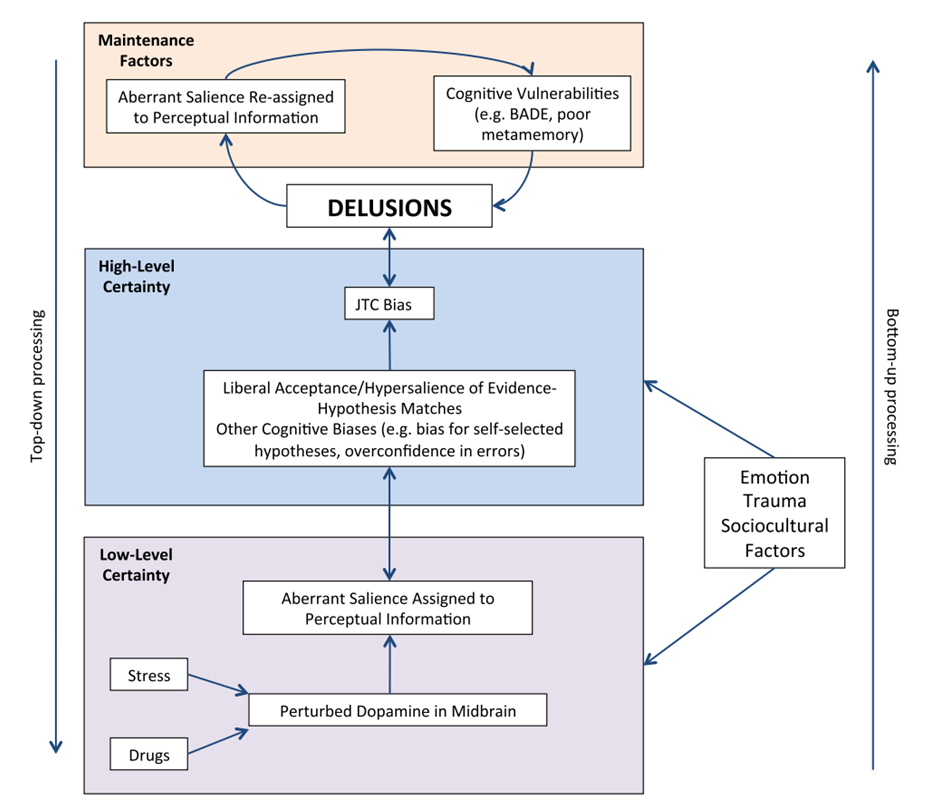
Combined model: Broyd et al. (2017)
Predictive coding models
- Predictive coding models argue that Bayesian prediction is the fundamental unit of information processing in the brain
- At every level, a prediction (prior) is tested against the outcome.
- The error (difference with prediction) along with a measure of confidence (precision) leads to an updated prediction (posterior)
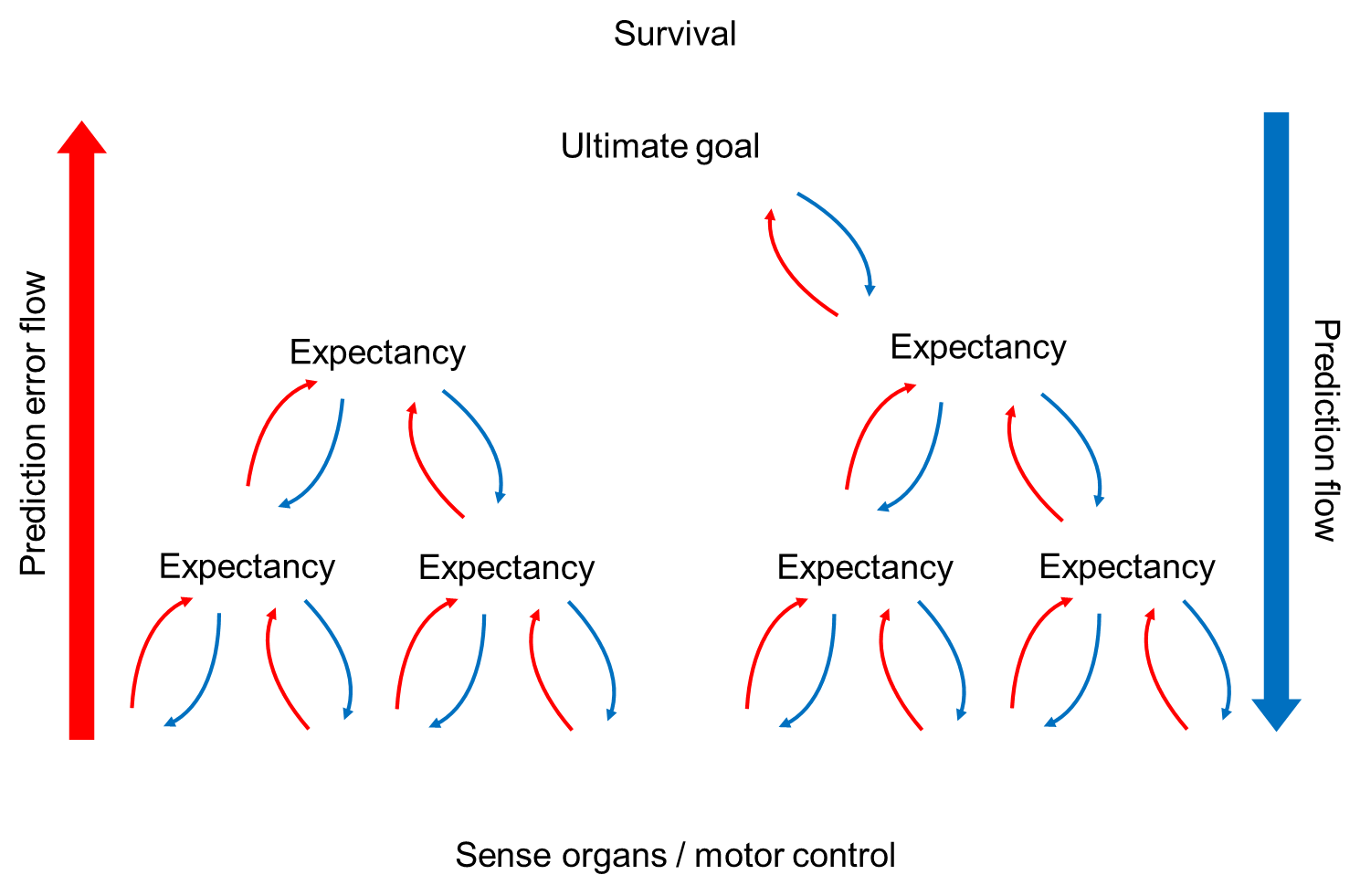 Predictive coding models of psychosis
Predictive coding models of psychosis
if cognition consists of layers of predictive coding feedback loops based on Bayesian principle → psychosis can be understood as a dysfunction to this system
Current predictive coding models
- Noisy prediction-error signals (Fletcher and Frith, 2009)
- Inaccurate or unreliable precision weighting (Adams et al., 2013)
- Differing effect of dysfunctional priors in different senses and at different stages of the hierarchy (Sterzer et al., 2018)
Conclusions
- Psychosis is considered a marker of severe mental health problems although some, typically less intense experiences, can occur without distress or disability
- Psychosis has many causes that are not the same in all people – better to think of ‘causal pathways’
- There are many models of psychosis, each of which emphasise a different aspect of the experience, often for different motivations (clinical work, cognitive science etc)