Week 10 - Value Trade Off
Agenda
The “official” Purpose of HTA
a multidisciplinary process that summarizes information about media, social, economic, and ethical issues…
Aim: To inform the formulation of safe, effective, health policies that are patient-focused, and set to achieve best value
“Ethical Paradox”
→ the intention: Ethics has been a stated, constituent part of HTA since its inception in the 1970s
→ the reality: “despite almost 40 years with repeated intentions, only a few HTA reports include ethical analysis” (Hofmann, 2014)
not printed in the actual report
the moral imperative
HTA is not just a calculation; it serves as a stewardship mechanism
At the hospital level:
Imperative: Responsible use of resources for the local community
Question: Does this new surgical robot mean cutting nursing hours elsewhere?”
At the Provincial level (e.g., BC HTA, INESS, Ontario Health):
Imperative: Balancing the health budget and ensuring equitable access
Question: “Does funding a $500k/year drug for 20 people mean 2000 people lose physiotherapy?”
At the Federal Level (e.g., CADTH):
Imperative: National standards, pricing, consistency, fairness
Question: “What precedent does this decision set for the entire country?”
Every HTA decision has moral consequences
What is normatively at stake?
Shifting from a technical problem to an ethical and political one
Technical Question (old HTA) vs. normative Question (real HTA)
Efficacy → what is the value of the outcome?
e.g., 3 months of life in pain vs. one month in high-quality life?
Cost effectiveness → What is a fair price, and what is the opportunity cost?
What do we give up by funding this?
Target Population → Who gets left behind by this definition?
Those not in trial, with co-morbidities, marginalised groups
Measurement → what should we measure?
Clinical endpoints, patient hope, family burden, social participation?
Innovation → Is this innovation responsible?
Addresses real needs or just a market opportunity? Is it sustainable?
Shaping the dilemma: Key tradeoffs
All HTA is a balancing act. There is no single right answer, only a justifiable one
common dilemmas
individuality vs collective
Life-saving drug for one vs. public health program for thousands
efficiency vs equity
maximum
innovation vs affordability
Rewarding new, uncertain, expensive tech vs. long-term sustainability
Transparency vs. health complexity
Simple, public decisions vs. Capturing complex, multi-dimensional value
The political choice
Balancing a tradeoff is not a scientific calculation; it is a political choice
Evidence informs the decision; it does not make it
Values (equity, solidarity, innovation, cost-effectiveness) drive the decision
The weight given to each value is a political act
Example 4$1M/ year rare disease drug
Technical frame: “ ICER is $1.5M/QALY above $50k threshold → recommend ‘no
Political frame: “We prioritise system sustainability over Rule of Rescue and vertical equity for this group”
Which value should matter most in a public system?
maximising total health
Getting the “most bang for the buck” ( highly cost-effective hip replacement)
innovation
Prioritizing cutting-edge tech (AI, gene therapy)
Fairness and Equity
Prioritising the sickest of those with no other options
Sustainability
Protecting the budget even if it means saying no to beneficial drugs
From Calculation to deliberation
How do we structure messy, value-based decisions?
We need models that move beyond simple calculation and embrace deliberation
Calculation:
plugging numbers into a formula to get the ‘right’ answer
Deliberation:
A structured, transparent, and fair process from making a justifiable choice in the face of value conflicts
Models for valuing tradeoffs
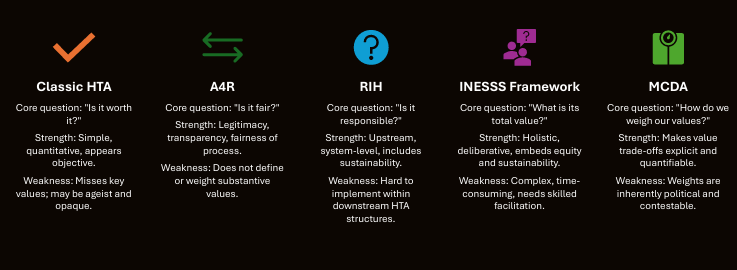
Model 1: Classic HTA
Is it worth it?
Tool: Cost-Utility Analysis (CUA)
Metric QALY (Quality-Adjusted Life Year)
1 QALY = one year of life in perfect health
0.5 QALY = 1 year of half at 50% health, or 6 months in perfect health
The ICER (Incremental Cost-effectiveness Ratio):
ICER = (Cost new - Cost old)/(QALY new - QALY old)
=$ per QALY Gained
Threshold: decision rule (e.g.) $50,000 per QALY) for judging value
Limits of QALY
Utilitarian focus: maximise total QALY, regardless of who gets them
‘ageism’: Preferentially funds treatments for younger people
Disability Bias:
Baseline utility for chronic disability may be 0.7; a treatment restoring to 0.7 may be valued as 0 gain
Meanwhile, a minor gain in a healthy person (0.9 →1.0) is valued
Conclusion: The QALY is a useful tool, but a poor master
Model 2: Accountability for reasonableness (A4R)
Core Question: What makes the decision legitimate and fair?
Focus: Fair process rather than a single “right” outcome
Four conditions for a fair process:
Publicity/transparency
Decisions, rationales, and evidence are publicly accessible
Relevence
Rationales based on reasons and values that stakeholders see as relevant
Appeals/Revision
Mechanisms to challenge and revise decisions in light of new evidence
Enforcement
Assurance that the first three conditions are actually followed
A4R in practice
Shifts HTA from a “black box” to a transparent deliberative body
What A4R does:
Creates a space for value trade-offs to be discussed
Hosts the political and ethical debate in a structured way
What A4R does not do:
Does not define substantive values
Does not tell you how to weigh competing values
Examples:
CADTH and INESS publish decisions and rationales, offer reconsideration processes, and include expert and public committees
Model 3: Responsible innovation in Health (RIH)
Core Question: Is this innovation responsive to systemic health system challenges?
Focus: move assessment upstream; steer innovation, not just screen it
Systemic challenges addressed:
Equitable access and reduction of inequalities
Workforce shortages and burnout
Accountable policy-tradeoffs
Environmental Sustainability
Key Value domains:
Population health value
health system value
Economic value (including frugality)
Environmental value
RIH in Proactive
Shifts HTA from reactive gatekeeper → Proactive system steward
Example: AI Surgical robot
Classes HTA question: Is it more effective than a human surgeon?
RIH-informed questions:
Does it exacerbate workforce shortages by requiring highly specialised staff?
Does it worsen inequality by being available only in elite hospitals?
What is its environmental footprint (energy-use, e-waste)?
RIH forces attention to long-term, system-wide impacts
Model 4: INESSS Multi-Dimensional Framework
Question: What is the total value of this technology for society across all relevant dimensions?
Focus: Holistic, value-based assessment integrating A4R and RIH principles
Five evolving dimensions of value:
Population Health Value:
Burden reduction, equity, social justice, and patient autonomy
Health System Value
Resilience, accessibility, responsiveness, and coordination
Economic Value
Affordability, opportunity cost, and long-term sustainability
Organizational Value
Governance, transparency, stakeholder participation, and data stewardship
Environmental Value
Lifecycle footprint, material waste, energy demand, e-waste
INESS model in practice: Rare Disease Example
Scenario: $1M drug for ~10 patients with low-quality evidence
Clinical dimension:
Acknowledge uncertainty; integrate experiential evidence from patients and caregivers
Population dimension:
Quantify unmet need; recognize priority status of ultra-rare, severely affected group
Economic dimension:
Recognize extreme opportunity cost and budget impact
Sociocultural dimension:
incorporate values of hope and solidarity (Rule of Rescue)
Environmental dimension:
usually downplayed here
Possible recommendation:
Yes, but…” (e.g., restricted centers, conditional coverage with evidence development)
Model 5: Multi-Criteria Decision Analysis (MCDA)
Question: How can we quantify values for a transparent choice?
Focua: Practical toolbox for multi-dimensional, value-based decisions
Typical MCDA process:
Step 1: Define criteria
Efficacy, equity, cost, innovation, quality of evidence, etc.
Step 2: Assign weights (political choice)
Committee debates relative importance (e.g., equity 30%, innovation 10%)
Step 3: Score options
Rate each technology (e.g., 1-5) on each criterion
Step 4: Calculate
Weighted average produces a composite “value score.”
Model comparison
Case studies
Case Study 1: AI in Medical Imaging
Technology: AI-driven software tool for a hospital radiology department