Anatomy of the Motor System
Page 3: Motor Areas of Cerebral Cortex
Primary Motor Area (M I)
Supplementary Motor Area (M II)
Premotor Areas includes:
Areas 6 and 8 of Brodmann
Broca’s Area (Areas 44 and 45 of Brodmann)
Frontal Eye Field
Regions involved:
Cerebrum: medial and tentorial surface supero-lateral surface
Frontal lobe: Precentral gyrus, Paracentral lobule (anterior part), Superior, middle, inferior, medial frontal gyri
Parietal Lobe: Postcentral gyrus, Superior parietal lobule
Page 4: Primary Motor Area (M I)
Corresponds to Area 4 of Brodmann in pre-central gyrus and anterior part of paracentral lobule.
Cortex is agranular with characteristic large pyramidal cells (Betz cells) in lamina V (15-60 microns in diameter).
Controls movements of voluntary muscles on the contralateral side.
Page 5: Motor Homunculus
Represents motor centres somatotopically:
Face and head below, trunk and lower limb above.
Lower limb below knee, involuntary control of micturition and defecation in anterior paracentral lobule.
Representation is not proportional to size but intricacy of movement.
Page 6: Supplementary Motor Area (M II)
Located on the medial surface of the hemisphere on the medial frontal gyrus (continuation of area 6).
Body representation: lower limb posteriorly, face anteriorly, intermediate part for the rest.
Lesions resemble effects of basal ganglia dysfunction.
Page 7: Premotor Areas
Areas 6 and 8 of Brodmann
Located in the posterior part of superior and middle frontal gyri in front of area 4.
Responsible for programming intended movements and control of movements in progress.
Divided into:
Dorsal area: movements initiated by the individual.
Ventral area: control of movements responding to external stimuli.
Lesions adversely affect skilled movements.
Motor Speech Area of Broca (Areas 44 and 45)
Located in the posterior part of inferior frontal gyrus.
Regulates coordinated movements of lips, tongue, palate, larynx, and pharynx during speech.
Injuries result in aphasia despite muscles not being paralysed.
Page 8: Frontal Eye Field
Located in the posterior part of the middle frontal gyrus, includes parts of areas 6, 8, and 9.
Stimulation causes conjugate eye movements to the opposite side.
Connected with cortical vision area in occipital lobe.
Lesion can lead to deviation of both eyes to the side of the lesion.
Page 9: Descending (Motor) Tracts
Efferent pathways: consist of pyramidal (conscious) and extrapyramidal (unconscious) tracts.
Extrapyramidal tracts: originate in brainstem.
Pyramidal tracts: originate in cerebral cortex, including corticospinal and corticonuclear tracts.
Page 10: Corticospinal Tract (Pyramidal Tract) - Origin
Composed of fibers from the primary motor area (Area 4) and additional fibers from:
Premotor area (Area 6)
Somatosensory area (Areas 3, 1, 2)
Superior parietal lobule (Area 5)
Page 11: Corticospinal Tract - Course
Fibers pass through:
Corona radiata
Posterior limb of internal capsule
Crus cerebri of midbrain
Ventral part of pons
Enter pyramids in upper medulla, where about 80% of fibers cross (decussation of pyramids).
Crossed fibers descend in lateral funiculus as lateral corticospinal tract; those that do not cross enter the anterior funiculus as anterior corticospinal tract.
Page 12: Spinal Cord - Transverse Section
Key tracts include:
Gracile fasciculus
Cuneate fasciculus
Anterior spinocerebellar tract
Spinothalamic tract
Lateral corticospinal tract
Various reticulospinal and vestibulospinal tracts.
Page 13: Nuclear Cell Columns
Spinal Laminae (of Rexed)
Contains various nuclei including:
Marginal nucleus, Posterior thoracic nucleus, Nucleus proprius, Intermediolateral nucleus, Medial and lateral motor nuclei.
Page 14: Termination of Tracts
Both lateral and anterior corticospinal tracts terminate in spinal cord gray matter at various levels:
Most fibers synapse with interneurons in laminae IV to VII.
Some fibers synapse directly on ventral horn neurons (lamina IX).
Page 15: Corticonuclear Tract
Pyramidal tract originating from motor areas (Area 4, 6, 3, 1, 2, 5).
Passes through the corona radiata, converges, and continues to brainstem nuclei of cranial nerves.
Innervates muscles of head, face, and neck, but does not descend to spinal cord.
Page 16: Corticonuclear Tract - Function
Innervates cranial nerves V, VII, IX, XII and contributes to motor regions of X.
Innervates bilaterally with exceptions in contralateral innervation for certain muscles (lower facial nuclei and hypoglossal nerve).
Page 17: Clinical Importance of Corticobulbar Fibres
Bilateral innervation leads to mild weakness from unilateral lesions.
Exceptions include:
Facial nerve (CN VII): contralateral innervation below the eyes.
Hypoglossal nerve (CN XII): contralateral innervation only.
Page 18: Damage to Corticobulbar Tracts
Unilateral lesions result in mild weakness; specific effects noted with cranial nerve involvement:
Hypoglossal nerve lesion: leads to spastic paralysis and deviation of tongue to contralateral side.
Facial nerve lesion affects muscles in contralateral lower quadrant of the face.
Page 19: Upper and Lower Motor Neurons
Upper Motor Neuron (UMN):
Located in the cerebral cortex; axons terminate in spinal cord or motor cranial nerve nuclei.
Lower Motor Neuron (LMN):
Located in the ventral gray column of the spinal cord or brainstem, innervates muscles through peripheral nerves.
Page 20: Lesions of Upper and Lower Motor Neurons
Upper Motor Neuron Paralysis:
Increased muscle tone, exaggerated reflexes.
Lower Motor Neuron Paralysis:
Flaccid muscles, atrophy, abolished reflexes.
Distinction between spastic (UMN) and flaccid (LMN) paralysis.
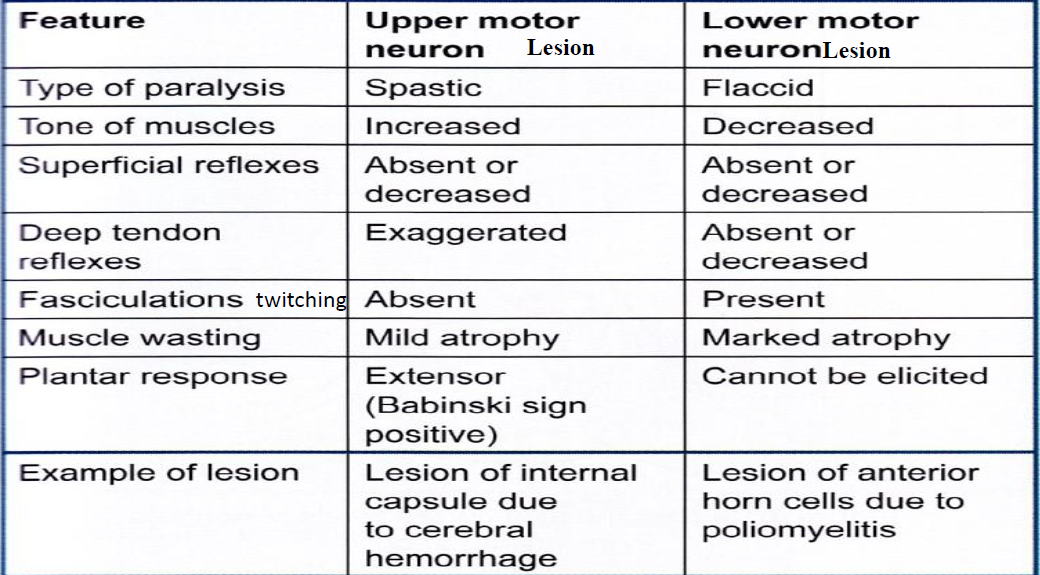
Page 21: Comparison of Lesion Signs
Table comparing signs between upper motor neuron and lower motor neuron lesions:
Page 22: Types of Paralysis
Monoplegia: paralysis of one limb.
Hemiplegia: paralysis of both limbs on one side.
Paraplegia: paralysis of both lower limbs.
Quadriplegia: paralysis of all four limbs.
Note: upper motor neuron lesions above crossing lead to opposite side paralysis, below leads to same side paralysis.
Page 23: Terminology for Motor Dysfunction
Paralysis: inability to move a body part.
Paresis: slight or partial paralysis.
Monoplegia: paralysis of one limb.
Hemiplegia: paralysis of one side of the body.
Paraplegia: paralysis of both upper or lower limbs.
Quadriplegia: paralysis of all four limbs.
Page 24: Extrapyramidal Spinal Tracts
Extrapyramidal system: consists of motor tracts not passing through pyramids of medulla.
Major tracts include:
Rubrospinal
Tectospinal
Vestibulospinal
Olivospinal
Reticulospinal
Regulates muscle tone, posture, and equilibrium, working alongside the pyramidal system.
Page 25: Rubrospinal Tract
Composed of axons from the red nucleus.
Fibers cross in lower tegmentum.
Functions in equilibrium, posture, and automatic learned movements (e.g., walking).
Facilitates flexors, inhibits extensors.
Page 26: Tectospinal Tract
Fibers arise from the superior colliculus, cross in the midbrain.
Responsible for spinovisual reflexes, conveys reflex postural movements to visual stimuli.
Page 27: Vestibulospinal Tracts
Lateral Vestibulospinal Tract
Arises from lateral vestibular nucleus (pons); important for equilibrium.
Facilitates extensor muscles, inhibits flexors.
Medial Vestibulospinal Tract
Arises mainly from medial vestibular nucleus.
Fibers are partly crossed & partly uncrossed.
Inhibitory role on neck and back muscles.
Page 28: Olivospinal Tract
Disputed existence; thought to arise from inferior olivary nucleus but recent studies suggest no direct pathways to the spinal cord (existence of olivospinal tract is strongly doubted).
Page 29: Reticulospinal Tracts
Medial (Pontine) Reticulospinal Tract
Originates from medial part of reticular formation of pons; regulates muscle tone and posture.
End directly/through interneurons on motor neurons of ventral gray horn of all levels of spinal cord.
Lateral (Medullary) Reticulospinal Tract
Arise in ventrolateral part of reticular formation of pons.
Fibers cross in medulla and descend in lateral funiculus.
Page 30: Differences Between Pyramidal and Extrapyramidal Tracts
Features | Pyramidal Tract | Extrapyramidal Tracts |
Composition | Corticospinal and corticonuclear tracts | Includes rubrospinal, reticulospinal, tectospinal, vestibulospinal |
Evolutionary Origin | Recent, present only in mammals | Older than the pyramidal system |
Fiber Source | Predominantly from cerebral cortex | Predominantly from subcortical areas |
Control Mechanism | Directly connected to lower motor neurons | Indirect connection, following a polysynaptic pathway |
Movement Type | Responsible for non-postural, precise movements | Responsible for gross postural movements |
Lesion Effects | Leads to increased muscle tone, spastic paralysis | Leads to spasticity and clasp knife rigidity |
Page 31: Self-Control Questions
Why is the corticospinal tract called a pyramidal tract?
Where are the primary and supplementary motor areas located?
List areas included in the premotor area.
Define motor homunculus.
Identify the center for lower limb movement below the knee.
Which part of the internal capsule does the pyramidal tract pass through?
What is the decussation of the pyramids?
Which structures receive unilateral innervation by the cortico-bulbar tract?
Compare upper and lower motor neuron lesion manifestations.
What are the functions of the rubrospinal tract, and what system does it belong to?