LIPID METABOLISM 3
Atherosclerosis - Defenition
It is the process that leads to the narrowing, or a sudden complete occlusion, of the arterial lumen.
lipid deposition in the subendothelial layer
ASCVD
coronary heart disease stops oxygen from getting to the heart and causes muscles to stop pumping blood around the body
stroke
peripheral vascular disease (in the leg)
renal artery disease will stop waste from leaving the body
PROGRESSION
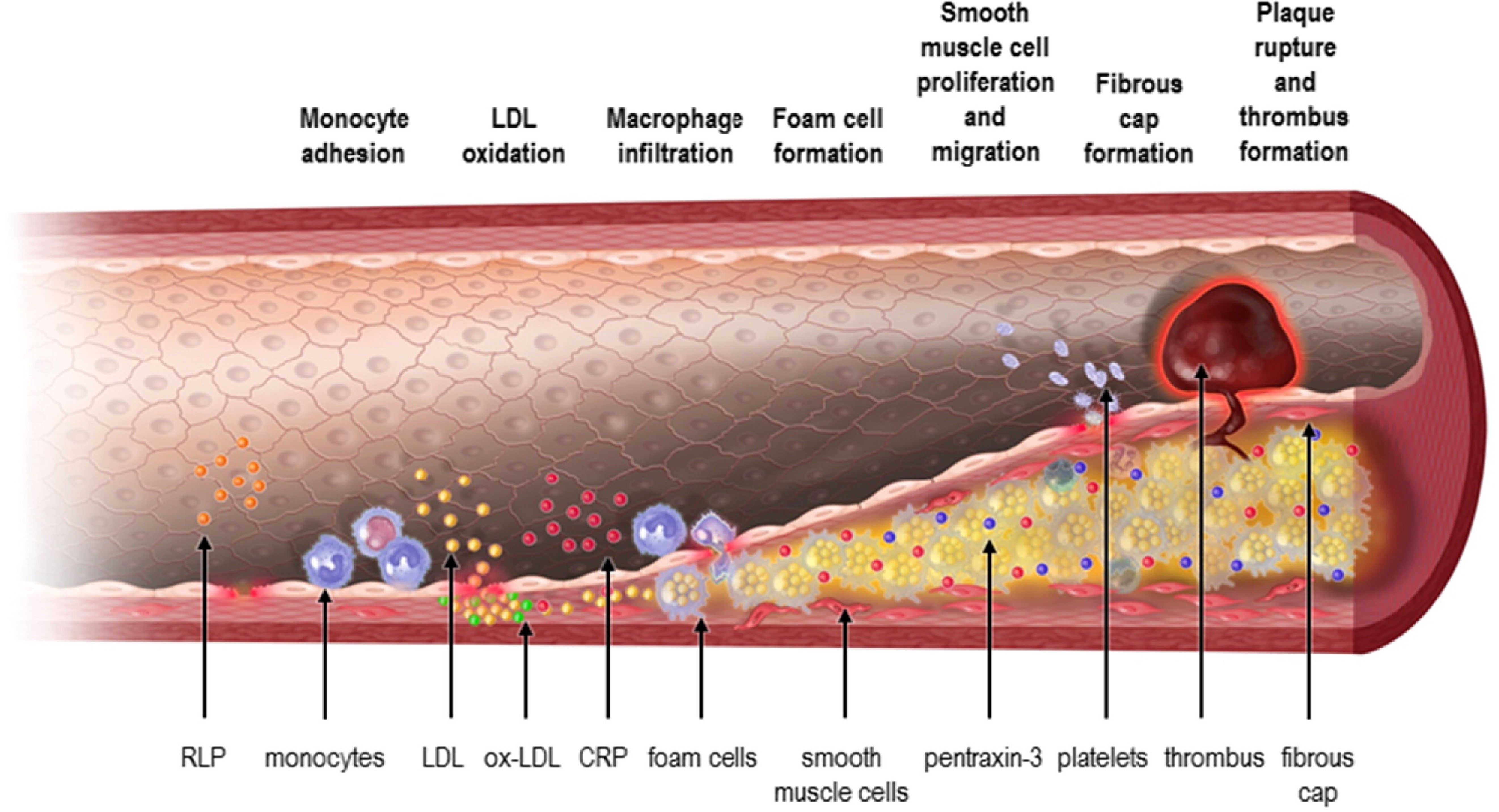
Material from the blood will fill the RLP area
RLP carries fat and proteins and deposits them in the blood tissue
RLP is the material left off after the body has digested the fatty acids and proteins
Macrophages take up anything that is Foreign in that tissue
foam cells send out signals to get more monocytes to help get rid of these tissues which create more foam cells in that tissues
higher blood pressure because of a narrow pathway.
this will damage the tissue.
angiogenesis - formation of new blood vessels
1) Endothelial Dysfunctional
2) formation of lipid layer within the intima
3) monocytes and smooth muscle cells migrate into the vessel wall to form macrophages
4) Foam cell formation ( Cholesterol as detergent)
5) Degradation of extracellular matrix
Calcification - Calcium build up in Plaques
> 5 years after plaque formation
The problem is over 40s
Arteries stiff, reduced expansion and contraction make it more difficult to treat Atherosclerosis
Stent is needed
Normal endothelial Layer have High Kruppel-like factors (KLF2-KLF4) anti-inflammatory control
Dysfunctional endothelium
A) KLF Factors suppressed
B) NFkB Predominates
increases expression of cell-adhesion molecules (CAMS)
Promotes adhesion of monocytes and T lymphocytes to endothelium
Decrease No production = promotes Vasoconstriction
INFLAMMATION
HDL is good cholesterol it takes away the build-up of macrophages from the liver.
Accentuated traditional Risk Factors
Dyslipidemia
smoking
hypertension
Physical activity
insulin resistance
Obesity
AUTOIMMUNE CONDITIONS :
Rheumatologic disorders
systemic Lupus Erythematosus
Risk factors elicit pro-inflammatory cytokines
High Fat diet
Diabetes and LPL deficiency
Increase Chylomicrons and VLDL
VLDL comes out of the liver to pass fats around the body
Hepatic Lipase deficiency (rare)
Usually secreted to the blood
helps transport HDLs
Converts VLDLs and IDLs to LDLs
in the disease
decreased secretion of hepatic lipase
change lipoprotein quantity
Greater risk of developing atherosclerosis of heart disease
LYSOSOMAL ACID LIPASE DEFICIENCY
1:40k to 300k people
lysosomal Acid lipase (LIPA gene muatations)
Usually: Cholesteryl esters and triglycerides break down in liver lysosome
EXCESS CHOLINE could possibly lead to heart disease
Gut bacteria convert excess dietary choline into trimethylamine
liver converts trimethylamine to trimethylamine N oxide
Function of Cholesterol
Modulates membrane fluidity
some nerve cells have 25% in PM
The brain contains 25% of the body’s cholesterol
yet less than 2% of the body’s weight
SYMPTOMS can start before the age of 10
abdominal pain is often due to inflammation of the pancreas
often enlarged liver
half-developed fat deposits under the skin
High-fat content in the blood
treatment - low-fat diet
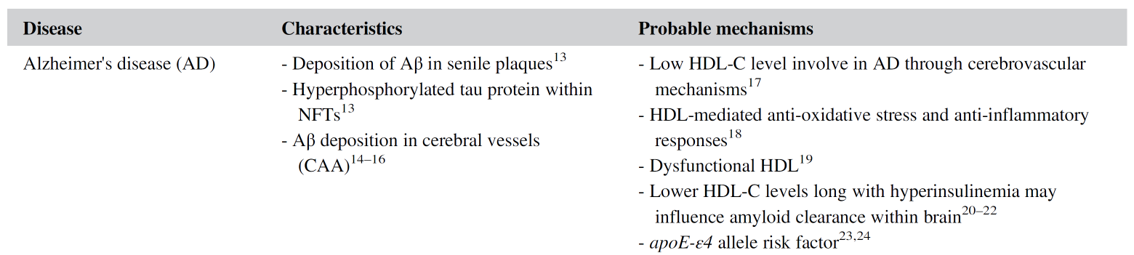
it affects over 44 million people. more in the elderly.
HDL
Decreases blood vessel deterioration
Decreases vascular inflammation
Increase No production
HDL LIKE PARTICLES + ApoA-I
once in the brain, they can inhibit Beta-Amyloid fibrillization
Decrease neuroinflammation
AB plaque can build up in the brain and the brain won’t be able to function properly
HDL cant cross the brain barrier
HDL LIKE PARTICALS + ApoE = detrimental effects (damaging the brain barrier)
PARKINSONS
alpha presynaptic protein monomer
Triacylglycerols (TAGs)
there a certain membrane components the APPM will configure with
unfolding of Alpha-Synuclein aggregation
Lipid pathway changes in Parkinson’s
decreased cholesterol
increases eicosanoids
increases DAG TAG AND GPI
Decreases sphingomyelin
Increased
lipid raft slightly elevated part of the membrane
increase LDL receptors
increased LDL uptake in the blood and increased cholesterol clearance
Via decreasing cholesterol precursors:
inhibit bile salt reabsorption
ingesting a charged resin (E.g. Cholestyramine)
Binds bile salts = decrease reabsorption
PCSK9 target LDL receptor for degradation.
Fibrates
Agonists of PPRA transcription factor
stimulate lipoprotein lipase
decreases plasma triglyceride concentration
increase in HDL
NIACIN
Binds to niacin receptors
reduces free fatty acid release from adipose
inhibits HDL uptake by the liver
ULTIMATELY
raise HDL
LOWE LDL
Lower triglycerides