Notes from practice assess Founds
enema, dementia, farenheit, injections, specimen collection, stages of dev, med administer,
Nutrition
dietary reference intake (DRIs) = RDA, estimated average requirements ( EARs), adequate intake (AI), tolerable upper intake level (ULs)
tolerable upper intake level: level not to exceesed to produc adverse
acceptable macronutrient distribution range (AMDR) daily % of macronutient
RDA: daily requirement considered adequate for healthy people
heart healthy lifestyle for HF:
weight everyday for fluid retention → call HCP if gain 3lb in 2 days
limit sodium for 2g per day
lie down and rest before meals bc eating needs energy and O2 comsumption
eat small frequent meals rather than big to decrease SOB
(furosemide = increase elimination of K) → increase K
diaharrea education: decrease GI motility + replenish electrolyte and flora
eat lot of K, probiotic
avoid alcohol, caffience, hot liquids, bc increase GI motility
carbonated, milk, fruit due to simple sugars
decrease fiber to decrease motility
well cooked veggies to decrease fiber
small meals throughout the day
Vit C + zinc help with wound healing
canned fruit have low fiber
1lb of fat = 3500kcal
gingitivitis= lack of c
spoon shaped nails = lack of iron
enteral feeding
report when:
gastric residual is >200mL
weight gain of >2lb in 24hr
3 loose stools in 24hr
ascultate before feeding
formula is in room temp
30-45 degree head
flash with 30mL
change bag every 3-7 days
NG:
removing:
disconect suction
instill 50mL of air
pinch NG while removing
pt holds breath
suction: 80-100mmHg
provide frequent oral hygene
measure drainage every shift
secure tube in gown
apply water-lube in nares
no air ascultation?
colonostomy care:
change bag before meal (change 3-7days)
cleanse stoma with warm water
herbs
echinacea: promote immunity
feverfew: wound healing + decrease inflammation w/ arthritis
valerian + camomile: decrease anxiety
ginger: N/V;
ginko: for memory
oral care:
unconsiuos: place in lateral position
open with padded tongue blade
use water or alcohol free mouth wash and use foam swab or soft bristle brush
check gag reflex
Elimination:
urinary catherte:
urine output : 30-50mL/hr → low =if catheter: check for patency before reporting
requires irrigation if not flowing (bladder scan shown urine despite catherter)
catheter irrigation: instill 30-40mL of fluid + 30-50ml syringe
subtract # of irrigation fluid from urine output
specific gravity: 1.005-1.030
male catheter holder : place it in upper thigh or lower abd
bowel obstuction
enema →side lying with right knee flexed (left side Sim position)
lub 2-3 in → insert 3-4in
hold container 12-18in in above rectum
if cramp then slowly lower
ascultate bowel sound
digital examination
enema:
hypertonic: cleanse pt preop
oil retention: stool softner
sodium polystyrene: high K
carminative: expel flatus
Specimen collection:
Urine:
clean urinary meatus
save discard 1st urine, then save all the rest of urine
urine w/ no feces
urine should be immideatly placed in container and refrigerated for at most 2hr
stool:
do not refrigerate
ask to defecate in bedpan or container → collect with tongue stick
sputum:
right when wake up
4-10ml collect
End of life care:
when patient dies:
obtain death announcemtn from HCP
verify if require autopsy → remove tube + indwelling lines
wash pt body
ask family if want to see body
place name tag
elevate head to not discolor face
religions when death
Islam: body is washed, wrapped during a ritual, then buried
Hindu: place body facing north then cremate
Judaism: stay with body until burial
Buddism: male family prepare body
complicated greif:
dependent
unresolved conflict
sudden death
individual had multiple recent losses
Infection control:
Protective enviroment:
for immoncompromised patients: positive air flow require 12 air exchange per hour + wear mask outside room to prevent contamination; HEPA filtration'; bathe daily with microbial soap
mask gown gloves, no plants, no visitors, avoid raw foods,
airborne: varicella, TB, measles
you do not need to limit visitors, just make sure they follow protocal,
anitmicrobial sanitizer is fine unless hands visible soiled
place soiled linens inside room
remove mask after room
droplet: FLU, pertussis, mumps, rubella, meningococcal pneumonia, streptococcal pharyngitis
gown, gloves, and surgical mask
contact: C. difficile, = use cholrine bleach to clean and use soap and water to wash hansd
MRSA, VRE, RSV, lice
if no contact with actual pt, then gloves is fine
when blood spill = clean with chloride bleach
primary prevention: immunization and screeing
secondary : early detection/stages of diease
third: rehabilitation and restoration
don: gown, mask, eye, gloves GMEG
doff: gloves, eye, gown, mask
Motility
can delegate SCD application to assistant personnel after initial assess of nurse
put legs dangling prior to standing to increase venous return and reduce ortho hypoTN + wait 60 seconds
with analgesic: always give before painful activity
ROM: 2 session/ day + 3-5 sets/ session (large joints 1st)
Cane:
is in strong side
flatter side is towards body
Walker:
to sit up, use chair not walker
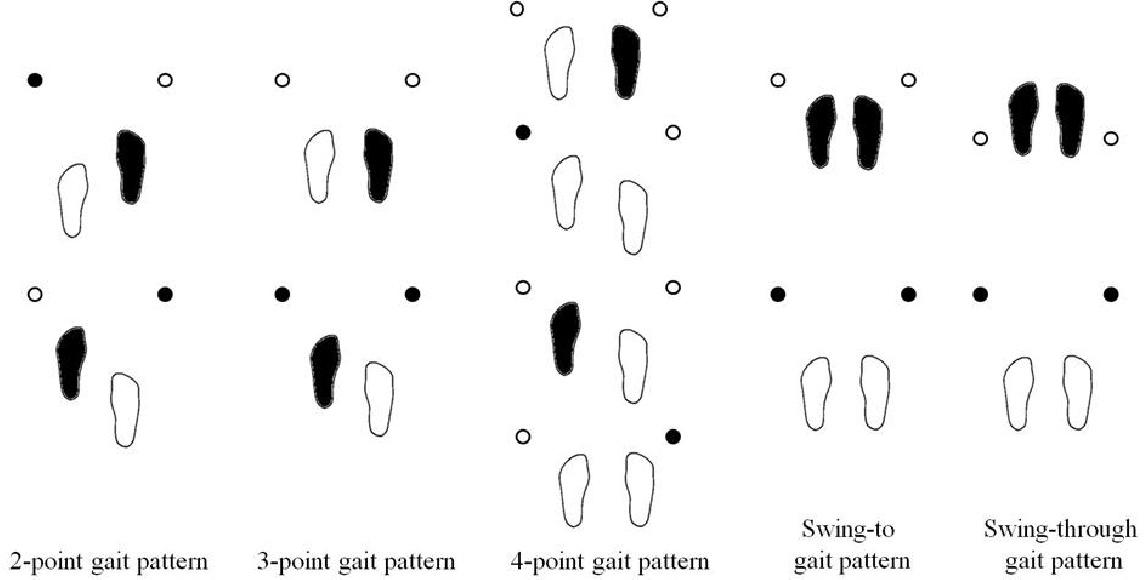
Crutches: weight on hand
swing gate: both crutches at once then swing
two point: opp leg and crutch together
three point: btoh crutchs and injured leg move then uninjured
four point: one crutch, opp leg, then other crutch, opp leg
up the stair: good leg first
descend: bad leg first
immotility:
prevent skin breakdown:
do not massage skin ares darker than skin because it can cause further capillary breakdown in subq tissues
use trapeze bar tue prevent shearing
chest physiotherapy for ateclais and fluid lung buildup:
tredenlenburg
percuss over one layer of cloth wiht cupped hand
crutch:
stairs:
descend: cructh first, then affected leg
sitting:
place crutches in one hand and grasp with other hand the arm of the chair

restraint
use padding
evaluate circulation q15min
remove restrains q2h while assessing hygene needs and toilet
DO NOT put restrain in beg frame
renew prescription q24hr
ensure 2 fingers fit
muscle groups:
antogonist: for joint : one contracts, other relax
synergistic: both contract
antigravity: stabilizing
skeletal: posture and voluntary movement
Assessment
latex allergy: also alergic to ethylene oxide ( banana, chestnut, strawberry, kiwi) + wrap cords ore devices containing latex
Assessments:
BP cuff 80% arm circumference
FLACC pain is for 2m -7y
confrontation test is for visual field
bladder scan:
place over symphysis pubis
instruct pt to void 10 mins before scan
pain assess:
quality: characteristic
severity: 0-10
onset, duration, pattern: if constant or intermmediate
Older adults
checkup
eye exam Q1Y/ Q2Y if no factors affecting vision
tetanus booster Q10y
shingles vaccine 50y old
pneumococcal when 65y due
or for people younger than 19 for heart, lung, liver disease, or smoke/ alcohol disorder
basilne ECG at 35
cholesterol Q5y
tuberculin Q2y
annual mammogram QY at 45 → 55 Q2Y
colonoscopy Q10Y
hearing aid:
allows for fine tuning of volume
physical activity dislodge
whistle sounds means hearing aid does not fit properly and build up of cerum
remove before shower
evaluation
subtracting 7: attention span
describe previous illness: remote memory
explain what to do in hypothetical situation: judgment
discuss meaning of common proverb: thinking abstractly
eyes:
glaucoma : high pressure: can be an obstruction in vitrous humor
retinopathy is changes in retina blood vessel
macular degeneration
Pre/post op
PCA pump:
intruct family members to not push button for clietn while client is asleep to revent toxicity
monitor Q1-2h for PCA pump for 1st 12 hr
instruct to use PCA pump when needed
seizure:
oral-nasal suction to reduce risk of aspiration
IS:
10/20time /hr
hold 5 sec breath after done
cough deeply after each use
stroke
dysphagia: offer tart or sour to inc saliva
careful w/ fluids bc may be too thin
tilt head foward
tracheostomy:
100% hypero2 for 2mins
pull suction 0.5in back when cough
allow 1 min between suction
max of 3 passes
do not cut guaze bc it can stay with threads
inflated cuff benefits:
stabilize tube
prevent aspiration and air leak
at home, for care, use medical asepsis
cover when outdoors
only remove inner cannula for cleaning since outer cannula is for stabilizing airway
half lumne size suction
120-150mmhg
nurse is a witness that the signature in the preop consent form is the pt
adolescent can give consent to treatmetn for sexually transmitted and SUD
chest physiotherapy:
trendelenburg
percuss over one single cloth layer
cupped hand
Med
IV
infiltration:
apply heat to increase circulation and remove filtration/ elevate arm
eye med
irrigation: above 1in toward lower conjuctive sac from inner to outer
exert pressure when holding eyelid (to open eye)
apply pressure in nasolactrimal for 30-60sec
hold eye dropper 0.4-0. in from lower conjuctiva
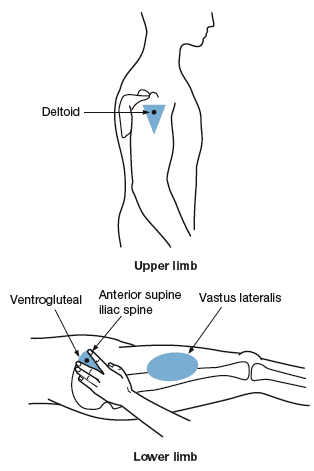
injection
ventrogluteal is safest ( for higher than 7 month)
dorsogluteal is too close to siatic nerve
deltoid may be underveloped (18 months)
vastus lateralis for child and infant
inhaler
shake before adm
rinse mouth after adm to reduce irritation
wait 20-30 secs between inhalantion
create seal, deeply inhale, hold for 10 sec
liquid
hold bottle with label in palm to prevent damage to label
med in cup is measured wiht meniscus or surface base of dosage scale
put auricle down for younger than 3 ( shorter)
Home safety:
home safety: toddlers in rear facing until 2years
ankle injury:
place covered 2/3 ice bag no longer than 30mins
o2:
wear cotton to prevent static
no oils or pretrolium
check daily + upright position
75watts for good lighting
Wound care

primary: wound edge is approxiamted
secondary healing: open wound
tenderness is expectied with pink granule appearence
tertiary: wound is closed but closure is delayed
types of wound dressing:
collagen: for clean, moist wound → stops bleeding and promotes healing
alginate = for exudate
proteolytic enzyme= debriment
hydrocolloid for 2 stage injury
change dressing daily
irrigation requires a 35ml syringe + warm solution
use eye protection + gown
remove staples: every other to see if healing