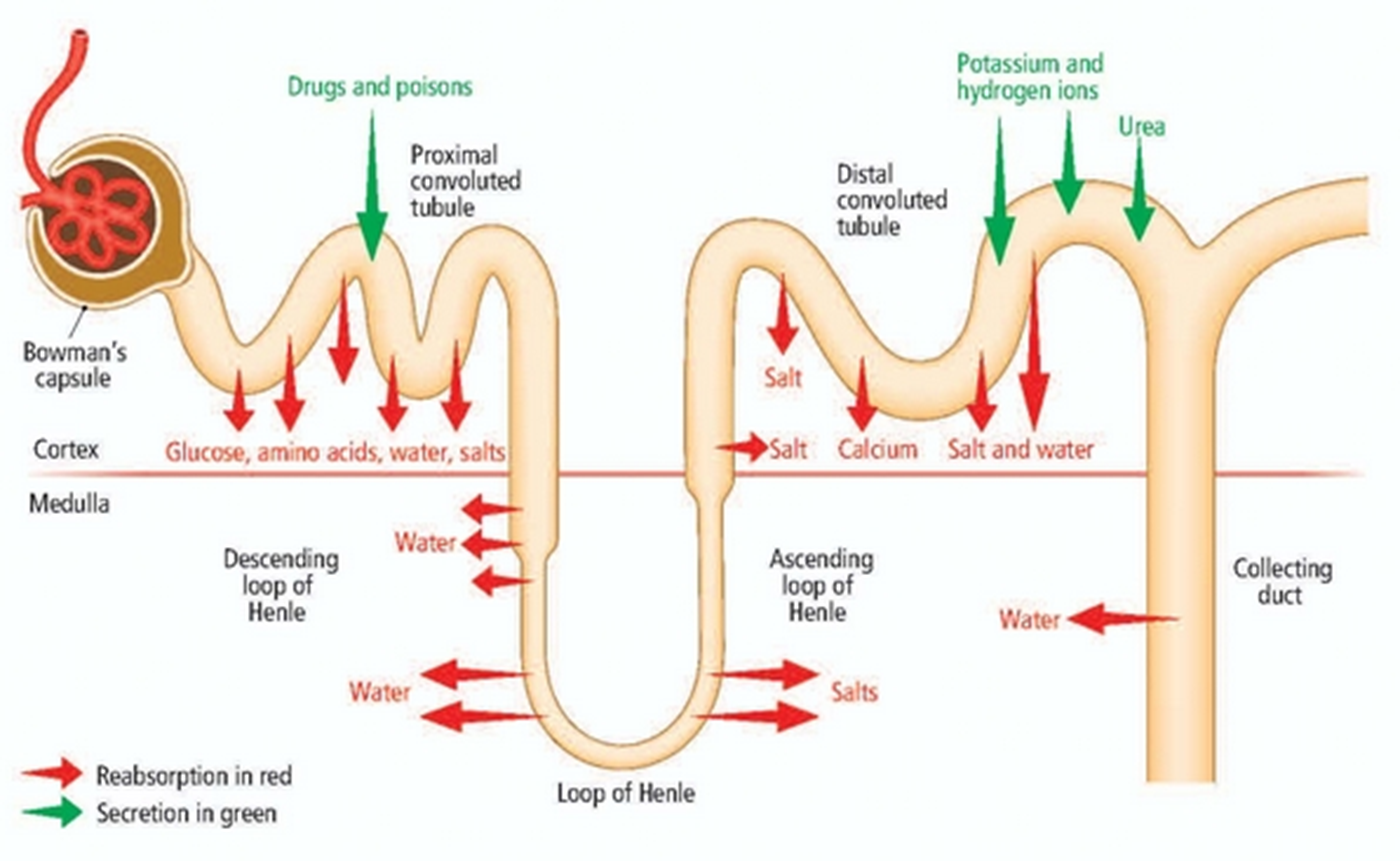
Reabsorption & secretion
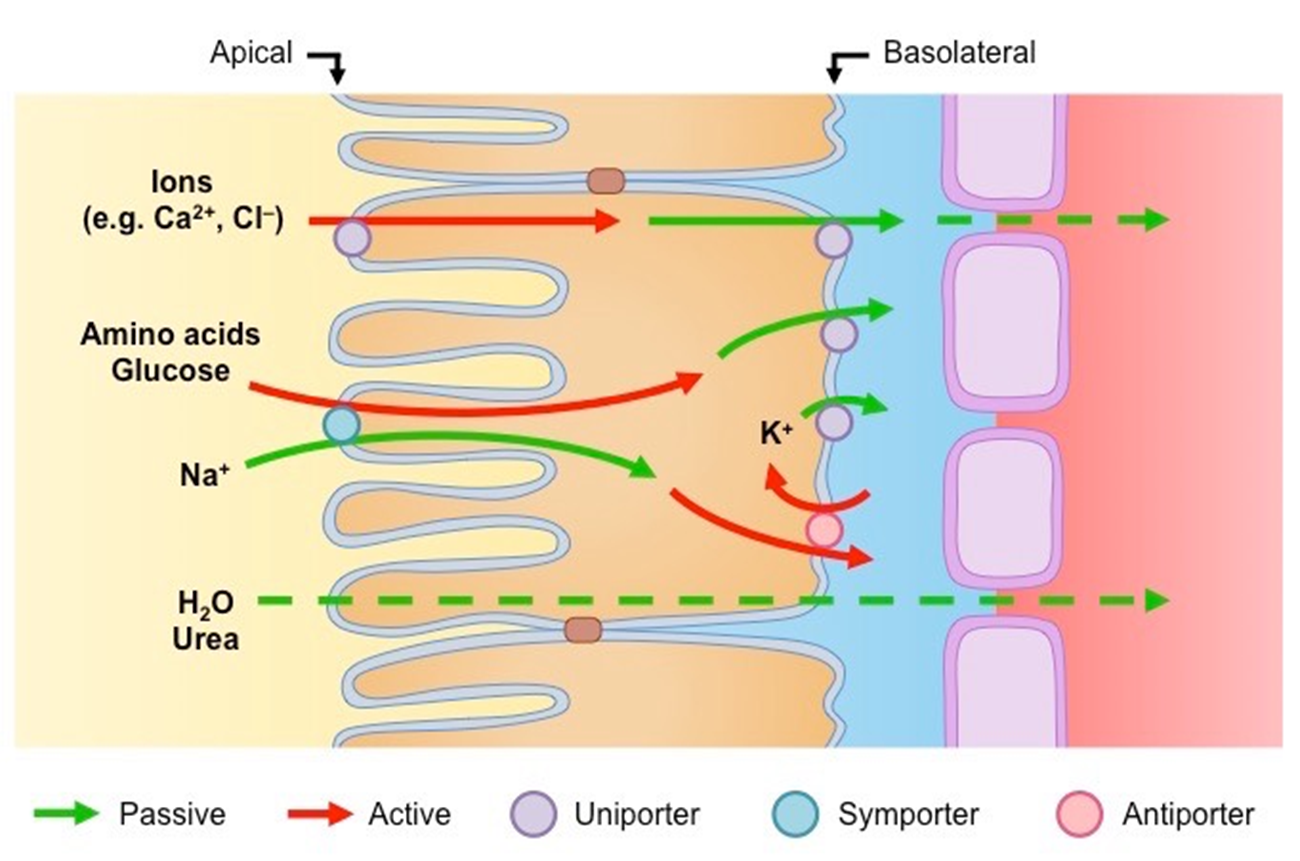
Tubular renal cells
polar
Apical / tubular cells: urine side
basolateral cells: interstitial side and peritubular capillaries
Maintains a concentration gradient for movement of solutes
Inside of cell = low concentration of Na
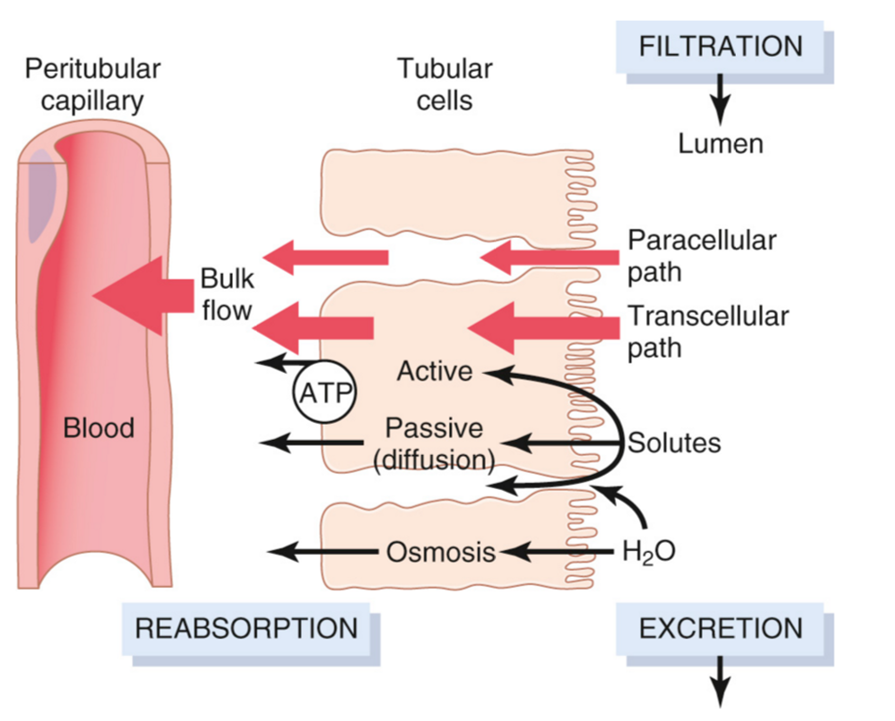
Paracellular transport
in between cells
channels
Transcellular transport
moves across cell membrane
simple diffusion
CO2/ water
transporters
Active transport
low to high
primary
uniport / cotransport
FORMS GRADIENT
BASOLATERAL SIDE
pump mediated
ATP requires
secondary
antiport / symport
APICAL / URINE SIDE = REABSORBSION
can be on basolateral as well
carrier mediated
facilitated by concentration gradient of carrier
carrier = Na
Passive transport
high to low
Facilitated diffusion
carrier mediated
channel mediated
simple diffusion
water and Urea

Diuretics
do not cross glomerulus
theyre secreted
Amino acids
reabsorbed in PCT
Carrier mediated w Na+ or H+
Apical and basolateral are both secondary active transport
Intact proteins
reabsorbed in PCT
rare in filtrate but can happen
endocytosis to get in and broken down into AA then back to blood
Metabolic intermediates
reabsorbed in PCT via cotransport w Na on Apical side
exchanged on basal side for anions
secondary active transport
PCT cation/ anion secretion
tertiary active transport
low specificity, high rate (100%)
Glomerular-tubular balance
Ability to adjust reabsorption rate to match the filtered load that comes across the glomeruli, and through the peritubular capillaries
Excretion > filtered load = net secretion
Excretion < filtered load = net reabsorption
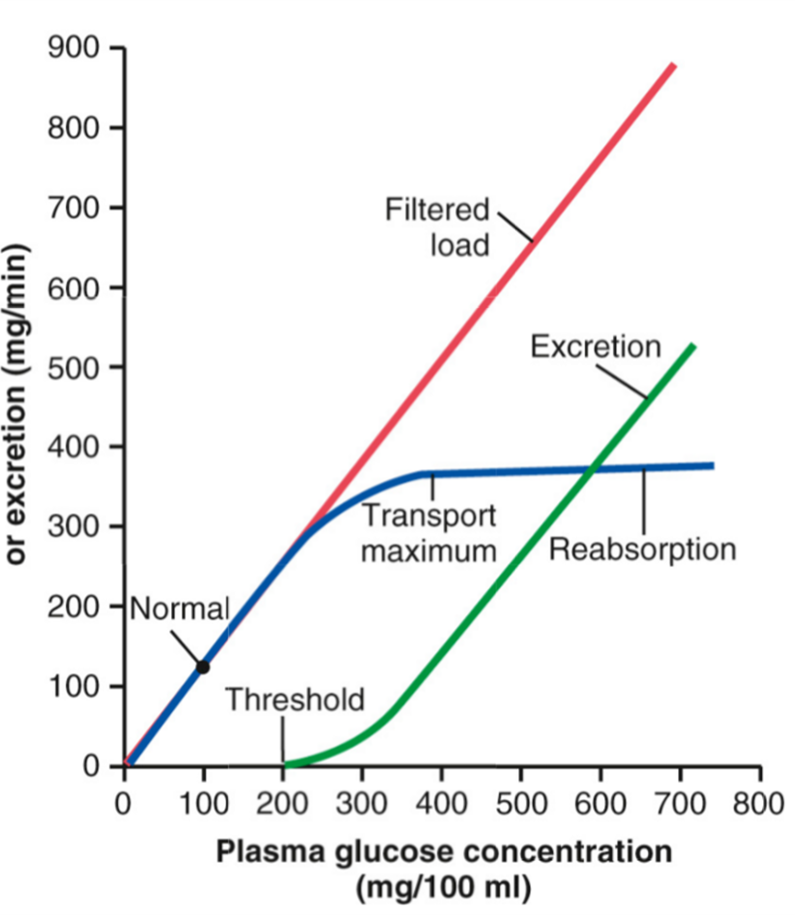
Glucose
100% reabsorbed in PT SHOULD NOT BE IN URINE
carrier mediated transport
Apical transport:
secondary active, coupled to sodium
SGLT2 in early PCT
SGLT1 in late PCT
Basolateral transport:
is facilitated diffusion
GLUT2 in early and GLUT1 in late
Both are insulin-insensitive transporters
Transport maximum
excess glucose youll reach trans max, and cannot reabsorb anymore glucose so its excreted in the urine (not good)
reabsorption matches filtered load
transports are 100% saturated at blood sugar of 350
excretion raises linearly w filtered load
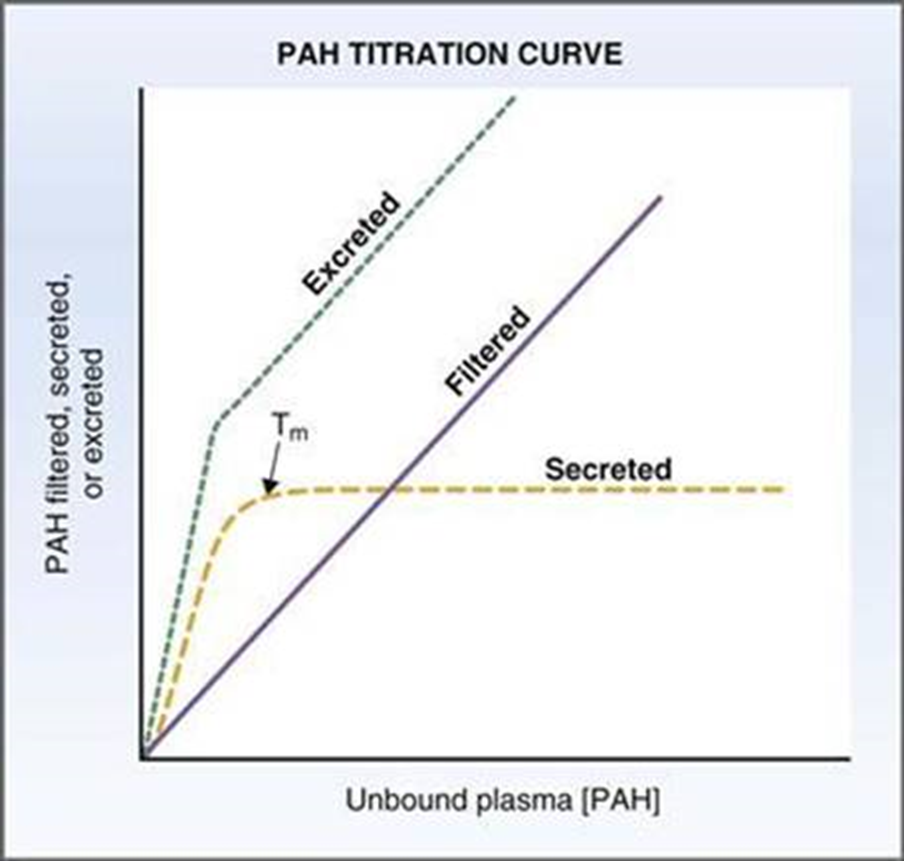
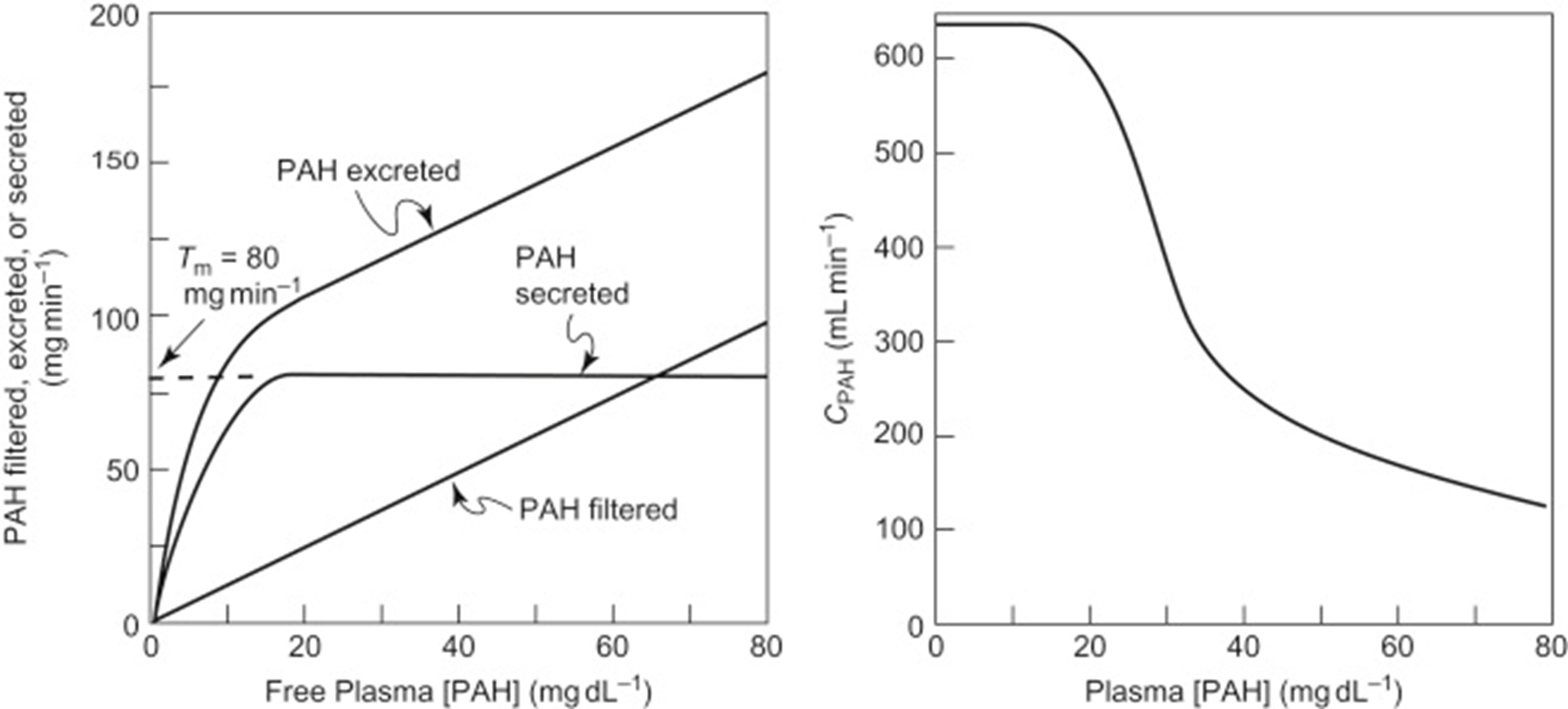
PAH
also has transport max
filtered and secreted 100% but NOT REABSOBED
when transport max is reached = saturation = no more secretion and its excreted linearly w filtered load
Creatinine
not 100% filtered
about 10% is secreted in PCT
H2 blockers can block secretion
competes w creatine for secretion channels
increases serum creatinine in blood
Fanconi syndrome
deficit in PCT reabsorption
causes lot of solutes that should have been reabsorbed to be excreted in the urine