Pharmocology phisology final
Digestive system
Hydroylsis reaction- is the use of using water to break down molecules
The digestive enzymes are normally within the lumen of the GI tract
this way they dont digest our own tissues
An example of this is Pancreatitis- where the inflammation of the pnacreas is mostly due to te preamture activation of digestive enzymes within the pancreas, which leads to autodigestion
this causes Edema and tissue damage, and abdominal pain with tenderness
Important concepts of the digestive system
The lumen o the digestive tragct is open at both ends, from the mouth to the anus
Digestion occurs outside the body, in hard enviorments
Permit one way transport: different regions within the GI tract are specialized for diffrent functions, so they act like a disassembly line
Indigestible materials pass from one end of the lumen to the other without crossing the peithelial lining of the GI tract
Clinical application- Acute oral intoxications
Activated charcol
Activated charcoal is used to bind toxins that have been ingested so that htey arent absorbed by the Gi tract
The charcoal is higly porous form of carbon which allows these toxic molecules to bind within the carbon matrix and stay there until excretted in feces
While there are benifits, ingestion of the charcoal must be taken within 1 hour of toxin ingestion
Charcoal dosnt bind to all toxins like: Metals, Alchols, Cuastic and corrosive chemicals, and cynide
it also comes with the risks of vomiting and aspiration
The digestive system is divitded into two functional partsL the tubular alimentary and Gastrointestinal tract and accesory digestive organs
The GI tract is 30 ft and includes the oral cavity, pharynx, esophagus, stomach, small instestine, large intestine, and anus
The accessory digestive organs include: Teeth, Tongue, Salivary glands, liver, gallbladder, and pancreas
Layers of the GI tract
The GI tract is made up of Four layers also called tunics
each tunic consitains a dominat tissue type that performs specific fucntions within the digestive system
From the inner to outer: Mucosa, Submucosa, uscularis, and serosa
however its not all the same in all regions of the GI tract
The Mucosa
The lines of the lumen contains villi and lacteals and has three sublayers (Protects, digests, and absorbs)
the first sublyaer is called thed Epithelium
it is adjacent cell sealed together by tight junctions with channels for selected ions
There are two types of Epitheliums
One is stratified squamous: found in the mouth, Esophagus and anus, this is to protect against the friction
Second is the Simple Columnar; rest of the GI tract which secretes mucus and digestive enzymes
The second sub layer is called lamina propria; its a thin layer of connective tissue that contains lymp nodules and capillaries
The third layer is called Muscularis mucoseL its a thin layer of smooth muscle that moves the mucosa to nechnace the contact with contents
The subucosa (structure, Flexibilitym and vessal supply)
Dense Irregular connective tissues
Highly vascular layer that serves the mucosa
absorbed molecules that pass through the comunar epithelium enter the blood and pymphatic vessels of the submucosa
Also contains the submucosal plexus, which is part of the enteric nervoys sytem that proides nerve supply to the muscularis mucosae
The muscularis ( Major movments)
Composed by inner circular and outer longitudinal layers of hte mooth muscles
is repsonsible fro segmental contractions (pulverization and mixing) and peristaltic movment (propelling)
The myenteric plexus (auerbacs plexus) which is located between the two muscle layers, this provides the nerve supply
it includes fibers and ganglia from both the lympatehtic and parasymapthetic systems
The Serosa (Protection, Strucutre, and lubrication)
Composed by a thin layer of loose connective tissue covered by a simple squamou epithelium
Mesotehlial cells are specialized to secrete a thinm watery (serous) fluid into the peritoneal cavity
GI tract- Oral Cavitiy
-Mechanical and chemcial rpcoesssing of food formation of food bolus
Teeth
Incisors: Sharp; used for cutting and slciing food
Canines:pointed; used for tearing adn ripping food
Premolars and molars; flat surfaces used for cursshing and grinding food
Tounge
moves the food around the mouth for effective matication a nd to create a food bolus (mix with saliva)
Pushes the food towards the orpharnyx (the voluntary phase of swallowing)
Ebners glands secretes lingual lipase; which begins lipid digestion; this is a very limited action
Salivary glands
Parotid glands produce 25% of total saliva and watery and rich in salivary amylase; which begins the process of digestoin of startch
submandibular glands: produces 70% of total saliva mixed secretion
Sublingual glands; produces 5% of total saliva rich in mucins of thick and lubricating saliva
Mastication and food bolus
The mecanical breakdown of food in the mouth into smaller pieces, mixing it with saliva to form a soft food bolus ready for swallowing
Food bolus: round mass of a size to be swallowed
Salivia composition
Salivary amylase: begins the digestion of startch
Lingual Lipase: begins fat digestion (limited)
Mucins: lubricate food
Lysozyme and IgA: antimicrobial defense
Gi tract- Pharynx and Esophagus
Pharynx
Connects the nasal and oral cavities to the larnyx and esophagus
diveded into three parts
nasopharynx: air only
Orpharnyx and larngopharynx: air and food
Swallowing/Deglutition
this is divided into three steps: oral, Pharyngeal, and esophageal
The oral phase is under voluntary control, while the pharyngeal and esophageal phases are automatic and controlled by the swallowing center in the brain stem
Receptors in the posterior portion of the oral caviyy and orpharynx stimualte the pharyngeal phase of swallowing reflex
1- the soft palate lifts to close off the nasopharnyx
2- the epiglottis covers the windpipie
3- the upper esophageal sphincter relaxes
Esophagus
This is the tube which transports the food and liquids from the pharynx to the stomach
Esophageal peristalsis (involuntary):
muscle contraction behidn the bolus
muscle relaxation ahed of the bolus to allow passage
secondary peristalsis
peristaltic reflex: stretch recetpors of sensory neurons in the wall detect distension and send singals to the myenteric plexus that coordinates movment
The upper esophageal sphincter and lower esophageal sphincter
contract to prvent air from entering the gastic refulx
relax during swallowing
Diigestion requires sufficient time of contact between food and active digestive enzymes
Stomach- Processes food with HCL and enzymes, forming chyme
j-shaped organ loacated between the esophagus and the duodenum
Its function is to store food, intiate digestion of proteins, kills pathogens with strong acidity of gastric juice, and to move the food int o the small interstines as a material called Chyme
semi-fluid very acidic mixture
Has three layers of smooth mucles with diffrent functions
1- Longitudninal muscle: propels the contents forward toward the duodenum
2- Circular muscle: mixes food with gastric juice
3- Oblique muscle: generates a twisting force that helps grind food
Gastic rugae are visible folds of the mucosa and submucosa that line the inner surface of the stomach
Empty vs when filled with food: the great epansion capacity without a large rise in pressure
Gastric pits are microscopic indentations in the mucoslal surface of the stomach; where each pit leads into gastic glands that contain several types of cells to secrete different products
Cells of the gastric glands
The Chief cells within the stomach; secrete pepsinogen and also produce gastric lipase
Parietal cells; secrete hydrocholoric acid, which helps maintain stomach acidity, kills pahtogens, and activates pepsinogen into pepsin
this begins hte protein digestion (partially)
this also secrete intrinsic factor, esstenial for vitamin B12 absorption
Mucous cells; secrete mucos to protect the gastric linings from pepsin and the acidic enviorment
Enerochromaffin like cells; secrete histamin and seotonin
histamine stimulates HCL secretion from Parietal cells
serotonini increase gut molitily
G-cells; secrete the hormon gastrin and stimulates acid secretion and gastric molitlity
D-cells secrete the hormone somatostatin
inhibits acid secretino and molitlity
PD1 cells; secrete the hormone ghrelin
stimualtes appetite
The secretions of Gastric cells togehter with a large ammount of water forms a highly acidi solution called Gastric juice
Protein are only partially digested in the stomach abyt the action of pepsin
Digestion of startch begins in the mouth wit hte action of salivary amylase bu the enzyem becoems in activated by the strong acidity of the gastric juice in the stomach
Ile salts are not present in the stomach to help with the digestion of fats
GI Tract- Small intestines (extensive digestion and abosop[rtion of nutreints form the chyme. Divided into the duodenum,jejunum, and ileum)
Pancreatic juice from the pancreas:
sodium bicarbonate to neutralize the stomach acid
Several digestvie ennzymes; Pancreatic amaylase, Trpysinogen, nucleases, adn pancreatic lipase (this does 70-90% of all dietart fat digestion) and is activated by the enzyme Enterokinases
Bil salts produced in the liver adn stored in the gallbladder
function as detergents for fat emulsification
Fat emulsification (fat is abosorbed into intestinal laceteals not into bloood cappillariers)
Lipase digests triglycerides into monoglycerides and fatty acids which are then diffused int othe epithelial cells
once abosrobed fatty acids recombine adn mix with cholesterol and lipoproteins which are also caled Chylomicrons (large)
lacteals have more permeable endothelium
What happens once the Gallbladder is removed?
Gallstones are solid particles that are formed in excess of cholesterol and biliruibin in bile
these produce sever abdonominal pain and risk for infections
The intestines recieves a steady trickel of dilute bile rather than large bursts during meals
this makes fat digestion less efficeient espeically when eating large and fatty meals
also have deficienceis of fat solbulbe vitamins
GI Tract- small intestines
Brush Border enzymes
these are enzymes located on the membrane of the microbilli in the small intestin
these do no secrete into the lumen, but they reamin attatche to the plasma membrane
Examples of these enyzmes are; Peptdiases, enterokinase, and maltase
Intestin motility
intestinal motoloty os spw as required for proper digestion and abosorption of nutrients
Peristalsis is much weaked in the small instestin compared to esophagus and stomach
Segmentation
Alternating conractions of circular muscle segmants at different sites
Contents are push back and ofrth, creating local mixing without net forward movment
Contractions of intestinal smooth muscle occur automatically and rhythmically
this rhythmicity is generated by pacemaker cells known as interstital cells of cajal
ICCS produce electericlal “slow waves” that spread only a short distance and thus must be regenerated by the next pacemaker region
autnomic nervous sytem modulates muscle deoplarization
GI tract- Large intestines- (abosroption of water and electrolytes from the chyme, and is divided into the cecum, asceding colon, Trasverse colon, decseding colo, sigmoid colon, and rectum)
Colon
Epitehlium has many transporters for sodium, chloride, and water
Gut microboiome/Microflora
trillions of microorganisms reside in the colon with a biomass greater than 1.5kg
only about 1% of gut speices are shared between individuals
How do we benifit from the microrganisms which residue in the gut
they produce vitamin K and some B vitmains and short chain fatty acids
break down dietary fibers that humans cant digest
comepte with harmful bacteria
and supports the immun system
How does the microbiome form?
at birth
Vaginal birth; the newborn is immedialtey colnized by vaginal and intestinal microbes form the motehr
C-section; colonziation comes mianly from skin and hospital enviroemnts which alters metabolic and immun profiles
breast feeding vs formula feeding
early chidhood diet and exposure to pets, rural enviroenments and antibitotics affect microbial diversity and immune tolerance
Has a 0-3 year critical peroid
Rectum
Feces storage until elimination
Stretch receports in the rectal walls detecet distension from fecal mass and send singals to the brain, initiating the urge to defecate
Anus
is controlled by two sphincters
1- internal anal sphincter- which is involuntary smooth muscle
2- External anal sphincter- which is voluntary skeletal msucle
ensures defcation when appropriate
Liver (metabolism, detoxification, and exocrine secretion)
Lheaviest inernal organ, located in the upper right side of the abdomen
Nutrient rich blood fro the gut passes through the liveer first thorugh a protal system
metabolizes and detoix=ifcaiton of compoudns
which risks liver damage
A liver lobule is the most basic strucural and functional unit of the liver
Hepatocytes; main functional cells of the liver
they remove toxins, process medications, store nutrients, adn secrete bile salts
Bile canliculus- is the bile duct
other cells are kupffer cells (immun syststem) and stellate cells (vitamin A storage)
Metabolism
stores glucose and releasesit when needed
synthesize nad brekads down and packages fats for transport
converts ammonia to urea
bilruibin metabolism
prouces essentail plasma proteins, including albumin and cmost clotting factors
Detoxifcation
uses CYP450 enzymes to modify drugs, toxins, and gormones
converts nonpolar molecuels into polar forms for kidney excretion
kupffer cells clear pathogens and debris
exocrine function
bile production
Liver Blood detoxicfication
TOxic molecule cans be cheimcally altered withi nthe hepatocytes by CYP450
these enzymes convert nonpolar molecules into more polar forms hy droxylation and by conjucation with highly polar gorups such as sulfate and glucornoic acid
polar derivatives are more easily excreted by the kidneys
Orally take drugs encounter CYP450
Bioavailbilty is the fraction of an admistered drug does that reaches the system circulation in an unchanged form
This can be altered by lvier diseases and enzyme inhibitoers or inducers
Route of administration can bypass it
Bile production
the liver produce and seretes 250 to 1500 ml of bile per day
The major constituents of bile are bile p[igment, ible salts, phosphjolipids, cholesterol, and inorganic ions
essential for the difgestion of fats
The liver has remarable rengerative apacity
after injury, mautre hepatocytes re enter the cell cycel and divide to resotre liver masss
when the required mass ire regained, proliferatiuon stops
Chronic injury to the liver leads to fibrosis and cirrhosis
this comes from lachol, hepatitits, toxins
Stellate cells transfoorms into myofriborblast like cells which produce collagen and create scare tissue
Pancreas:Amphicrine Gland
Exocrine Pancreas (98%): composed by acinar cells (Mylases, Proteases, Lipases, and nucleases) and ductal cells (bicarbonate)
Endocrine pacreas (2%) mainly composed of a and b cells which are forms of islets of langerhasn
Alpha cells are (25%) and secrete the hormon glucagon which increases blood glucose
Beta cells (75%) secetres the hormon insulin which decreases the blood glucose
How do cells intake Glucose
GLucose requries GLUT transporters to enter the cells
skeletal muscle and adipose tissue contain GLUT4 insluin dependent
Liver nad pancreas use GLUT2 Insulin independent (allows sensing of glusoe)
Brain and smooth muscle use GLUT1/3 Insuline independent
Insulin Phisiology
Secreted in repsonse to high blood glucose (after meals)
Insulin Translocate GLUT4 transporters from the cytoplasm to the membrane of cells
Promotes storage and anabolism
glycogen synthesis
inhibits heptaic glucsoe production
stimulates fat stroge and inhibits lipolysis in adipose tissue
Glucagon Physiology
secreted when glucsoe is low (fasting, sleeping)
Raises the lbood glucsoe by mobilizing store dneergy
increase glycogenylysis and gluconeogensiss
2 ways to regulate glucagon releases
inthe fesstate insluin supresses a-cells. When glucsoe levels drop removal of inhibtion on a-cells
Over depolarizaiton inhibits glucagon release
Clinical application
Type 1 diabites: destrruction of pancreatic beta cells, leading to absolute insulin deficiency
cant make insluin
Type 2 diabites: whic is the desentization of insulin
has insulin but cant use it
Accumulation of glucose in the blood (hyperglycemia) white it is lacking the cells
Urinary system
Major functions
Main system for removing the metabolic wastes
pH regulation via bicarbonate reabsorption and H+ secreation
Blood pressure control via RAAS, sodium balcne ,adn fluid volume regulation
The strutcutre of the system consists of two kidneys, two ureters, one bladder, and one urethra
The kidney is the functional orga nresponsible for filtration, reabsoprtion, secretion, and horomn production
the ureters and urethra are passageways
the bladder is a storage organ
Kidney
The outer region is the cortex and the beneath it is the medulla, which is organized into renal pyramids and speerated by renal columns
The tip of each pyramid forms the renal papilla, where the urine drains into minor calyces and then into the renal plevis
Inside the kidneys are millions of functional units called nephrons
Nephron Strucutre
Glomerular (or bowmans) capsule
its a cup shapped sturcutre surrounding the glomerulus
filters blood in to the nephron
Proximal Convoluted tubule (PCT)
reabsorbs most nutrients, some water and electrolytes
Nephron loop (of Henle) builds the gradient thati sed to conentrate the urine
Descending Limb: permeable to water
asecending limb: impereable to water, actively transports sodium and chloride out
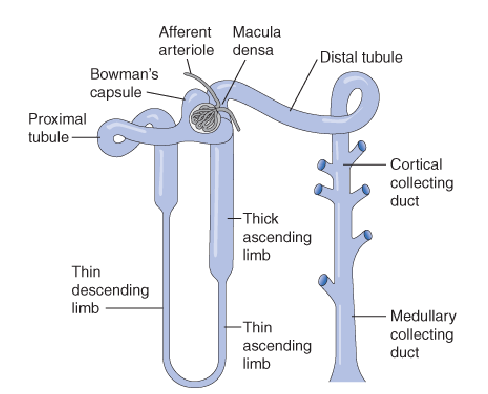
Distal confulted tubule (DCT)
fine tunes electrolytes and nutrients reabsorption
secrertion of H+ ions
Collecting duct
Collects and concentrates the filtrate from multiple nephrons
urine is funnled through th erenal pelvis and out hte kidney
Nephron types
Cotrical Nephrons (85%)
Location:glomeruli are located high in the cortex far from the medulla
nephron loop: short,rarley reah the inner medulla
function: filtration and solute reabsorption
Juxtamedullary nephrons (15%)
location: glomeruli are located near hte corticomedullary junction
Nephron loop: long, extends deep into the medulla
function: urine concentration
Ureter
A tube formed by smooth muscles which carrieres urine form the kidneys to te bladder
the Ureter undergoes peristalsis (wave like rhythimic contractions)
Intense pain occurs when a kidney stone passes through
The pace maker regions are located at the renal calcyes and pelvis
Bladder
Stores urine and expels it by coordiated contraction during urination
stretch recetpros in the bladder detecet increase volume and sendsignals ot the pina lcord and brain
Parasympathetic system
contraction of the derusor muscle
realction of the interl urethral sphincter
Urethra
conducts urine from the bladder to the exterior of the body
Uretheral length varies by the gender
greater risk of UTS within females
Two sphincters: internal and external
internal sphinceters have smooth muscle and are involuntary
this helps prevent urin leakage
External sphincter: is skeletal msucle which is voluntary
allows control of urination
Clinical application: Urinary incontinence
Uncontrolled leakage of urine due ot the dysfunction of the bladder, ureathral sphincers, or neurla contol
Babies and small chidlren have nureal pathways that arent full developed so the urination is reflexive
stress incontinence, inrease the abdominal pressure or trama
Urge incontinence: due to the overatcive detursor muscle
Renal Physiology
Filtration: movment of plasma (not including proteins) from the glomerular capillaries into the bowmans capsule
Reabsorption: movment of substances from the tubular fluid back into the peritubular capiullaries to return them into the blood stream
secretion: movment of substances froim the peritubular capillaries into the rena ltubule to be elimiated in the urine
Organic anion transporters: penicillin, Antivirals, Prostaglandins
Organic cation transporters: metformin, Cimetidine, Dopamine
Cruical for lcearing protein bound drugs that cannot be filtered
Major site of drug drugeinteractions especailly via comeptition
Glomerular Filtration
Water and dissolved solutes move from vlood plasma into the glomerular capsule tand then into the nephron tubules
This is driven by a net filtration pressure of 10mmHg at rest
Flomerular filtration rate is the voume of filtrate produced by both kidneys per minute
usually around 7.5 L/hr
the total blood volume averages about 5.5L
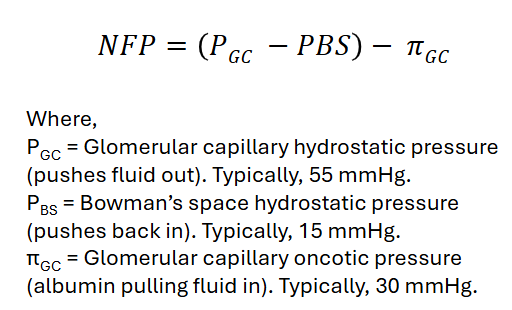
The bowmen capsule has three barrieres that serve as the selective filters
Capillary fenestrae
It has large pores that allow water and small oslutes to pass easily. This is coated with negatively charged glycoalyx that exctrostatically repels plasma proteins
Glomerular Basement Membrane
This is rich in Type IV collagen and negatively charged proteoglycans
Major rate limitying layer for fitration (size and charge barrier)
Podocytes (epthielial cells)
food precess (pedicels): interlocking like fingers
Filtration slits; Gpas between pedicels covered by a slit diaphgragm that allows only small molecuels to pass thorugh
Dissolved plasma solutues pass easily thorugh the three barrieres to enter the interior of the golmerular capsule
Formed elemnts of the blood are excluded
Plasma proteins are excluded from the filtration beacuse of hteir large sizes and net negative charges
Proteinuria: proteins in the urine
Meaturia: RBCs i nthe urine
Regulation of Glomerular Filtration Rate
Afferent Arteriole constriction or dilation changes GFR
constriction decreases blood flow which decreases GFR
Dilation increases blood flow which increases GFR
This is controlled by extrinsic and intrisic mechansims
Extrinsic Mechanisms: sympathetic nervous system
vasoconstriction
Intrinsic mechanism (or renal autoregulation)
Myogenic reflex: vasoconstriction in response to stretching of the afferent arteriole
Tubuloglomerular feed back: group of specialized cells called the macula densa, which is located at the top part of the ascending limb, these snese NaCl conecntration in the filtrate
High NaCl afferent arteriole constircftion to decrease GFR
Low NaCl afferent ateriole dilation to increase GFR
Juxtaglomeular Apparatus
a speciallized strucutre where the thick ascending limb commiunicates with teh afferent arteriole to regulate GFR
composed by main cells
Granculer Cells
Synthesize , store, and secrete renin in the blod
responds to low renal perfusion presure and prostanglandisn fro the macula densa
Macula densa
When NaCl is high (high GFR) it releases adenosine; causes afferent arteriole constriction and decreases renin releases from grandular cells
when NaCl is low (low GFR) releases nitric oxide and prostalgandins (stimulate renin relases from granular cells)
Reabosorption of Glucose
occurs in hte proximal convulted tubule by secondary active transport
Proeprty of saturation: when the transported molecule is present in sufficiently high conecntrations all of the carrier be come occupied and the transport reaches a maximal value
The average Tm for glucsoe is 375 mg/min
the average trate of glucse filtration is 125 mg/min
glycosuria: presence of glucsoe in the urine which leads to diabetes mellitus
Reaboorption of bicarbonate and secretion of H+
Bicarbonate is absorbed indriectly mostly in the proximal convuoluted tubule.
80-90% of the bicarbonate is reabosrobed to rpevent blood acidosis
H+ is sexcerted in the distal conluted tubule using two additional buffer systems present in urine to prevent urine from becoming to accidic
Reabsorption of NaCl and Water
the filtrate is somotic with the plasma
the proximna convoluted tubule reabsorbs 65% of all filtered The loop of henle creates a Corticomedullary gradient that enables urine conentrations
Na,Cl and Water
this occurs through active transport of the sodium and passive momvment of water and Cl ion
The filtrate stays isomotic because salts adn water are removed in apoprotionate ammounts
300mOsm entering adn 300 mOsm leaving the proxima convoluted tubule
The loop of Henle creates a corticomedullary gradient that enables urine concentration
super salty interstital fluid in the medullla and less salty in the coretx
Descending limb: permebale to water not to salt; so the filtrate becoems hyperosmotic
Ascending Limb: imperable to water but permable to salt. filtrate becoems hypoosmotic
This gradient provides a driving force for water reabsportion by osmosis in the collecting duct
The filtrate that enters the distal conoluted tubule in the cortex is made hypotonic, whearas the interstitatl fluid in the medulla is made hypertonic
The collectin gduct runs through the salty remnal medulla
this losses water by osmosis but solutes mostly remain= urine concentration
Effect of ADH in Urine Concentration
Antidiuertic hormone is produced by the hypothalmus and secreted by the pitutiary gland
it binds to the V2 receptors on collecting duct cells
this triggers inseration of aquaporin 2 water hcannels in to the apical membrane
Water is reabosrobed from the tubular fluid into the hypersomomtic medullary intersitium
Effect on urine: Decreases the voblume and osmolality increases
Measurment of Glomerular Filtration Rate
rate clearance of inulin
Freely filtered by the glomerulus, not bound to plasma proteins, not secreted, bit reabsorbed, not metabolized by the renal tubules
Becuase all inulin filtered at th eglomerulues appears in the urin, its teh renal clearns is exactly equal to GFR
not used routinley to access kidney function
Estimated GFR (eGFR)
Creatinine
this is produced in the muscles from creatine and relaeased into th eblod plasma and is measured t oasses kdiney function
easy to measure, cheap, and provides constant relative results
Creatinine is mostly elimated by glomerular filtration and its levels are measured in the serum
How do we know the kidneys only filter 20% of the blood plasma
Clearance of para-aminophippuric acid
exogenus moelcules infused into the blood
Some PAH is filtered into Bowmans space remaning PAH in pertiubuler capillaries is actively secreated using OATS the kdiney removes almost all PAH from the blood in one pass
the norma lPAH clearance has been found to average 625 ml/min the glomerular filttration average 120 ml/min this indicates that the only 120/65 of the renal plasma flow is filtered
Reproductive System
Gametes
Gametes are cells responsible for sexual reproduction
Two main types: sperm cells (produced by males) and oocytes (produced by females)
The two production systems evolved very differently
Males
Produce millions of sperm cells per day
Strategy: high quantity, low-cost gametes — success depends on numbers and competition
Sperm production continues throughout life, but quality tends to worsen with age
Why Sperm Quality Declines With Age
Spermatogonial stem cells divide continuously from puberty onward
More cell divisions = more replication errors
Older paternal age is linked to:
Decreased sperm motility
Increased number of mutations
Increased DNA fragmentation
Increased risk of infertility
The stages of sperm development: Spermatogonia → Primary spermatocyte (first meiotic division) → Secondary spermatocytes (second meiotic division) → Spermatids → Spermatozoa (spermiogenesis)
Females
Born with a finite pool of primary oocytes (1–2 million at birth)
Strategy: high-quality, resource-rich gametes (energetically expensive)
Oocytes are produced mostly during fetal development:
6–7 million at mid-gestation
Reduced to 1–2 million at birth via oocyte atresia (a form of apoptosis)
Ovulation: one mature oocyte released per month → only 400–500 are ovulated in a lifetime
Why Oocyte Quality Declines With Age
All primary oocytes are formed before birth and remain arrested in meiosis I for years to decades
Each cycle, a small group is recruited, but only one ovulates
Consequences of prolonged arrest:
Gradual loss of cellular integrity
Cohesin proteins degrade over time → loss of chromosome cohesion
Microtubules become less stable → increased risk of chromosome mis-segregation (aneuploidy)
Example: risk of Trisomy 21 (Down Syndrome) increases sharply with maternal age
Gametes and Fertilization
A gamete is a haploid cell formed by meiosis
Contains half the chromosomes of a normal somatic (body) cell
During fertilization, two gametes combine to form a zygote:
23 (sperm) + 23 (oocyte) = 46 chromosomes (complete human genome)
Important notes:
A single gamete does NOT contain all of a parent's genetic information — their combination makes a "complete" human
No two gametes are identical because of DNA recombination
Sex Determination
The first 22 pairs of chromosomes are called autosomal chromosomes (homologous pairs that look alike and contain similar genes)
The 23rd pair are the sex chromosomes:
Female: two X chromosomes (XX)
Male: one X and one Y chromosome (XY — not fully homologous)
The X and Y chromosomes look different and contain different genes
Formation of Testes and Ovaries
Following conception, the gonads of males and females are indifferent for the first ~40 days
The SRY gene on the Y chromosome encodes the testis-determining factor (TDF)
TDF triggers the undifferentiated gonad to develop into testes
Females: have delayed structural development and are hormonally inactive in fetal life
Follicles do not develop until the third trimester
Males: testes become functionally active early
Develop seminiferous tubules and interstitial cells in early embryo
Testosterone in the fetus is crucial for forming male internal and external genitalia
Internal Genital Ducts
Two duct systems are present in every early embryo:
Mesonephric ducts (Wolffian ducts) — male potential
Paramesonephric ducts (Müllerian ducts) — female potential
In Males (with testosterone)
Testosterone → mesonephric ducts develop into epididymides, ductus deferentia, ejaculatory ducts
Anti-Müllerian hormone (AMH) → paramesonephric ducts regress
Other embryonic structures → form the prostate and penis/scrotum with testosterone
In Females (without testosterone)
No testosterone → paramesonephric ducts develop into the uterus and uterine tubes
No AMH → mesonephric ducts regress
No testosterone → other structures form the vagina, labia, and clitoris
External Genitalia
Early external genitalia are indifferent — derived from homologous structures
DHT (dihydrotestosterone) is mainly responsible for fetal male external genital development
Testosterone is converted into DHT
Homologous structures:
Genital tubercle → glans penis (male) or glans clitoris (female)
Labioscrotal swellings → scrotum (male) or labia majora (female)
Urethral folds → fused to form urethra (male) or labia minora (female)
Female Reproductive System
Divided into internal, external, and accessory organs
Internal Organs
Ovaries
Two main functions:
Reproductive: produce and release oocytes (ovulation once per month after menarche)
Endocrine: produce estrogen and progesterone
Uterine Tubes (Fallopian Tubes)
Site where fertilization usually occurs
Lined with ciliated epithelium to help move the oocyte toward the uterus (whether fertilized or not)
Tubal implantation = ectopic pregnancy (pathological)
Uterus — composed of three layers:
Perimetrium: outer connective tissue layer
Myometrium: smooth muscle layer
Responsible for uterine contractions: labor, sperm transport, menstruation
Endometrium: inner functional layer; highly vascularized mucosal tissue
Thickens each cycle to prepare for implantation
Shed during menstruation if no pregnancy occurs
Vagina
Muscular canal (smooth muscle) containing lubricating mucus glands
Reduce friction during intercourse
Produces an acidic environment (pH 3.5–4.5) to protect against pathogens
External Organs
Vulva
Labia majora and minora: protect internal genital structures, maintain moisture and barrier protection
Clitoris: highly innervated erectile tissue; main role is sexual arousal and sensory function
In females, the urethral opening and vaginal opening are separate (unlike in males)
Accessory Organs
Mammary Glands (Breasts)
Produce milk during lactation
Organized in ducts containing alveolar cells, which are the functional milk-producing units
Milk flows through ducts into the nipple
Regulated by:
Prolactin → stimulates milk production
Oxytocin → stimulates milk ejection
The first milk produced is colostrum, which is rich in antibodies (IgA) and immune factors
Ovulatory and Menstrual Cycle
Follicles are fluid-filled structures surrounding the oocyte — usually one dominant follicle matures per cycle
Pituitary Hormones
FSH (follicle-stimulating hormone):
Promotes follicle growth and maturation
Increases estrogen production
LH (luteinizing hormone):
Triggers ovulation at around day 14 by inducing rupture of the follicle
Ovarian Hormones
Estrogen: drives endometrial growth (proliferative phase)
Progesterone: maintains and stabilizes the endometrium (secretory phase)
Phases of the Cycle
Follicular Phase (Days 1–14)
FSH stimulates follicle development
Estrogen levels rise → endometrium thickens
LH surge at day ~14 → triggers ovulation
Ovulation (Day ~14)
Dominant follicle ruptures and releases the oocyte
Luteal Phase (Days 14–28)
Ruptured follicle becomes the corpus luteum, which produces progesterone (and some estrogen)
If fertilization occurs:
Embryo implants in endometrium
Corpus luteum is maintained
If fertilization does NOT occur:
Corpus luteum degenerates into corpus albicans
Progesterone and estrogen levels drop
Endometrial shedding = menstruation
Male Reproductive System
Internal organs: testes, epididymis, vas deferens, urethra
External organs: penis, scrotum
Accessory organs: seminal vesicles, prostate
Important distinction: the male urethra is shared by the urinary and reproductive systems (unlike females)
Testes
Part of both the reproductive system (sperm production) and endocrine system (testosterone production)
Two main functional components:
Seminiferous tubules: produce sperm (spermatogenesis)
Interstitial (Leydig) cells: produce testosterone
Hormonal regulation:
FSH → stimulates spermatogenesis
LH → stimulates testosterone production
Testes are located in the scrotum to maintain a temperature 2–3°C lower than body temperature (required for sperm production)
Epididymis
Site of sperm maturation (where they gain motility) and storage (1–2 weeks)
Vas Deferens
Muscular tube that transports sperm from the epididymis via peristaltic contractions
Seminal Vesicles
Produce the majority of seminal fluid (up to 70%)
Rich in:
Fructose (energy source for sperm)
Prostaglandins (aid sperm movement)
Clotting proteins
Prostate
Produces prostatic fluid (20–30% of semen)
Fluid is slightly alkaline — helps neutralize the acidic vaginal environment to protect sperm
Prostate tends to increase in size with age → can compress the urethra
Leads to difficulty urinating = benign prostatic hyperplasia (BPH)
Prostate cancer: malignant growth of prostate cells — one of the most common cancers in men
PSA (prostate-specific antigen): a protein produced by prostate cells used clinically as a biomarker for prostate disease
Checked via blood test, prostate can also be assessed via digital rectal exam