Neuro
Anxiolytic and Hypnotic Agents
1. Introduction
Anxiety: A feeling of tension, nervousness, apprehension, or fear involving unpleasant reactions to a stimulus.
2. Psychological States Affecting Anxiolytic and Hypnotic Drugs
Sedation: Loss of awareness and reaction to environmental stimuli.
Hypnosis: Extreme sedation leading to further CNS depression and sleep.
3. Benzodiazepines Overview
Definition:
Benzodiazepines are a class of central nervous system (CNS) depressants.
Used to manage anxiety, insomnia, muscle spasms, seizure disorders, and alcohol withdrawal.
Prescriptive Popularity & Advantages:
Among the most commonly prescribed sedative-hypnotic agents.
Noted for effectiveness, rapid onset, and relatively high safety margin compared with older barbiturates.
4. Benzodiazepines: Mechanism of Action
Working Process:
Benzodiazepines enhance the effects of gamma-aminobutyric acid (GABA), the main inhibitory neurotransmitter in the CNS.
Binding occurs on specific benzodiazepine receptors on the GABA-A receptor complex, increasing the frequency of chloride channel opening.
Chloride ion influx hyperpolarizes the neuron (less excitable), leading to CNS depression—producing sedation, anxiolysis, and muscle relaxation.
Key Concept:
Benzodiazepines do not directly activate GABA receptors; they potentiate GABA's natural inhibitory effect.
5. Pharmacologic Uses of Benzodiazepines
Categories:
Anxiolytic: Reduces anxiety and agitation.
Sedative-hypnotic: Promotes relaxation and sleep.
Anticonvulsant: Controls seizure activity.
Muscle relaxant: Decreases skeletal muscle tension.
Amnesic: Causes short-term memory loss (useful for medical procedures).
6. Actions & Indications of Benzodiazepines
Actions:
Lower doses assist with anxiety; higher doses induce sedation and hypnosis.
Indications:
Anxiety disorders, alcohol withdrawal, hyperexcitability, agitation, and preoperative relief of anxiety and tension for balanced anesthesia.
7. Common Benzodiazepines and Uses
Drug Name (Generic) | Common Brand | Primary Clinical Uses
Diazepam | Valium | Anxiety, muscle spasms, seizure disorders, alcohol withdrawal.
Lorazepam | Ativan | Anxiety, sedation before surgery, status epilepticus.
Alprazolam | Xanax | Generalized anxiety and panic disorders.
Clonazepam | Klonopin | Panic disorders, seizure disorders.
Temazepam | Restoril | Short-term treatment of insomnia.
Midazolam | Versed | Sedation and amnesia before procedures or surgery.
8. Pharmacokinetics of Benzodiazepines
Absorption:
Well absorbed from the GI tract.
Peak Levels:
Achieved in 30 minutes to 2 hours.
Distribution:
Lipid soluble, distributes well throughout the body, crosses the placenta, enters breast milk.
Metabolism:
Primarily metabolized in the liver; excretion is mainly in the urine.
9. Adverse Effects of Benzodiazepines
Common Adverse Effects:
Sedation, drowsiness, lethargy.
Depression.
Blurred vision.
Confusion.
Dry mouth.
Constipation.
Nausea/vomiting.
Hypotension.
Urinary retention.
10. Nursing Considerations for Benzodiazepines
10.1 Assessment
Obtain medication history regarding other CNS depressants (e.g., opioids, alcohol).
Assess level of anxiety, sleep patterns, or seizure activity prior to therapy.
Monitor vital signs, specifically respiratory rate and level of consciousness.
10.2 Implementation
Administer at bedtime for sleep aid.
Avoid abrupt discontinuation (can cause withdrawal symptoms such as tremors, seizures, anxiety).
Use the lowest effective dose for the shortest duration.
For IV preparations (e.g., lorazepam, diazepam), monitor for respiratory depression.
10.3 Patient Teaching
Avoid alcohol, opioids, and other sedatives while on benzodiazepines.
Caution against driving or operating machinery until effects are known.
Rise slowly to prevent orthostatic hypotension.
Do not stop suddenly; taper under provider supervision.
Secure medications due to the risk of misuse and dependence.
10.4 Evaluation
Observational outcomes: reduction in anxiety, improved sleep without excessive sedation, no signs of dependence or withdrawal.
11. Contraindications of Benzodiazepines
11.1 Absolute Contraindications
Conditions:
Known hypersensitivity/allergy (risk of severe allergic reaction).
Severe respiratory insufficiency or sleep apnea (further CNS depression may cause respiratory arrest).
Severe hepatic impairment (toxic accumulation for long-acting agents like diazepam).
Acute narrow-angle glaucoma (increases intraocular pressure).
Shock, coma, or acute intoxication (risk of respiratory and cardiovascular depression).
11.2 Relative Contraindications
Conditions:
Chronic obstructive pulmonary disease (COPD): may worsen hypoventilation; caution advised.
Elderly or debilitated patients: higher CNS sensitivity and fall risk.
Pregnancy and lactation: risks to the fetus or infant.
Substance use disorder (alcohol or drug dependence): high risk of tolerance and dependence.
Renal impairment: may prolong effects.
Depression/suicidal ideation: increased risk of mood worsening; appropriate mental health support required.
12. Drug Interactions for Benzodiazepines
Interacting Substances:
Alcohol: profound CNS and respiratory depression; contraindicated.
Opioids: increased risk of fatal respiratory depression.
Antihistamines, barbiturates, antipsychotics, antidepressants: additive sedation risk.
Drugs affecting metabolism:
Valproate, cimetidine, oral contraceptives can lead to increased drug levels.
Smoking can induce metabolism, potentially reducing effectiveness.
13. Symptoms of Benzodiazepine Withdrawal
Aches/pains, abnormal body sensations, grand mal seizures, nausea, insomnia, delirium/detachment from reality, muscle spasms, anxiety/panic attacks, depression.
14. Other Anxiolytic and Hypnotic Drugs
14.1 Antihistamines
Examples:
Promethazine (Promethegan), diphenhydramine (generic).
Uses: Preoperative and postoperative medications; decrease narcotic need.
Note: Cause drowsiness but do not induce sleep.
14.2 Buspirone (Buspar) (Generic)
Reduces anxiety signs/symptoms without severe CNS effects and adverse effect .
14.3 Dexmedetomidine (Precedex)
Used for sedation in intubated/mechanically ventilated patients.
14.4 Eszopiclone (Lunesta)
FDA approved for insomnia management.
15. Non-benzodiazepine Anxiolytics
15.1 Buspirone Overview
Definition: Prototype and most commonly used non-benzodiazepine anxiolytic.
Mechanism of Action:
Works on serotonin (5-HT1A) and dopamine (D2) receptors.
Does not affect GABA, causing minimal sedation and no dependence.
Onset: Takes 2–4 weeks for full effect (not for acute anxiety).
15.2 Common Side Effects
Dizziness, light-headedness, nausea, headache, nervousness/excitement at treatment start.
15.3 Contraindications / Cautions
Avoid use with MAO inhibitors (risk of hypertensive crisis).
Grapefruit juice can increase drug levels.
Use caution in liver/kidney impairment.
15.4 Nursing Considerations for Buspirone
Emphasize consistent use; not a PRN medication. must be taken consistenly
Gradual relief expectations (2–4 weeks).
No alcohol/sedatives concurrently; monitor dizziness, especially in older adults.
Reinforce adherence, even if anxiety improves.
16. Other Anxiolytics
16.1 Sedating Antihistamines
Examples: Hydroxyzine (Vistaril, Atarax), Diphenhydramine (Benadryl).
Mechanism of Action: Block histamine (H1) receptors producing sedation/anxiolytic effects.
Uses: Short-term anxiety management or sleep promotion when benzodiazepines contraindicated.
16.2 Side Effects
Drowsiness, dry mouth, blurred vision, urinary retention (anticholinergic effects).
16.3 Nursing Considerations for Antihistamines
Avoid driving/operating machinery.
Encourage hydration/oral care for dry mouth.
Caution against concurrent alcohol/CNS depressants.
17. Hypnotics (Non-Benzodiazepines)
17.1 Overview of Hypnotics
Definition: Medications inducing and maintaining sleep, closely related to sedatives.
17.2 Sedatives vs. Hypnotics
Sedative: Reduces anxiety and promotes relaxation. Lower doses
Hypnotic: Induces drowsiness and maintain sleep, usually at higher doses than sedatives.
Subclass of CNS depressants, often related to sedatives (clam with nessarily cauing sleep)
17.3 Non-Benzodiazepine Hypnotics
Examples:
Zolpidem (Ambien), Zaleplon (Sonata), Eszopiclone (Lunesta).
Mechanism of Action: Act on GABA-A receptors but at different subunits than benzodiazepines.
Produce sedation with minimal anxiolytic/muscle-relaxant effects.
17.4 Therapeutic Uses of Non-Benzodiazepines
Short-term insomnia management, preoperative sedation, adjunct to anesthesia, control of anxiety, and treatment of nocturnal awakenings.
17.5 Advantages of Non-Benzodiazepine Hypnotics
Lower risk of dependence.
Minimal next-day sedation if used correctly.
Short half-life is beneficial for sleep onset.
17.6 Side Effects
Drowsiness, dizziness, headache, sleepwalking/sleep-driving (complex sleep behaviors), rare hallucinations/confusion (especially in older adults).
17.7 Nursing Considerations for Non-Benzodiazepine Hypnotics
Administer right before bedtime.
Patient must have at least 6–8 hours to sleep.
Avoid alcohol/CNS depressants.
Educate about potential sleep-related behaviors.
Caution in elderly to reduce the risk of confusion and falls.
18. Melatonin Receptor Agonists
18.1 Examples
Ramelteon (Rozerem), Tasimelteon (Hetlioz).
Mechanism of Action: Mimics the body’s natural melatonin by acting on melatonin receptors (MT1 and MT2) in the hypothalamus to regulate the sleep-wake cycle.
Uses: Sleep-onset insomnia and Tasimelteon for “non-24-hour sleep disorder” in blind individuals.
Advantages: No dependence or withdrawal, not a controlled substance.
18.2 Side Effects
Dizziness, fatigue, endocrine effects (elevated prolactin, decreased testosterone).
Nursing Considerations: Administer 30 minutes before bedtime.
Avoid high-fat meals (delays absorption).
Effects may take several days to become noticeable.
19. Barbiturates
19.1 Examples
Secobarbital, Pentobarbital.
Mechanism of Action: Depress CNS by enhancing GABA and directly opening chloride channels.
Uses: Occasionally used for anesthesia induction, seizure control (not typical for insomnia).
Risks: High potential for tolerance, dependence, and fatal overdose (respiratory depression).
20. Summary Table of Drugs
Drug/Class | Prototype | Key Use | Onset | Dependency Risk | Main Nursing Concern |
|---|---|---|---|---|---|
Benzodiazepine | Temazepam | Sleep induction & maintenance | 30–60 min | High | Respiratory depression, fall risk |
Non-benzodiazepine | Zolpidem | Short-term insomnia | 15–30 min | Moderate | Complex sleep behaviors |
Melatonin agonist | Ramelteon | Difficulty falling asleep | 30 min | None | Hormonal changes, dizziness |
Antihistamine | Diphenhydramine | Mild insomnia | 30–60 min | Low | Anticholinergic effects |
Barbiturate | Secobarbital | Rare use | Rapid | Very high | Respiratory & CNS depression |
Antidepressant Agents
21. Signs & Symptoms of Depression
Low energy levels.
Disturbances in sleep patterns.
Lack of appetite.
Limited libido.
Inability to perform activities of daily living (ADLs).
Overwhelming feelings of sadness, despair, hopelessness, disorganization.
22. Biogenic Amine Theory of Depression
Theory posits that depression results from deficiency in norepinephrine (NE), dopamine, or serotonin (5-HT) due to:
Monoamine oxidase (MAO) may degrade these neurotransmitters affecting recycling/restoration.
Rapid neuronal firing may lead to depletion of neurotransmitters.
Increased number/sensitivity of postsynaptic receptors depletes neurotransmitter levels.
23. Actions of Antidepressant Therapy
Mechanisms:
Inhibit the effects of MAO, increasing NE or 5-HT in the synaptic cleft.
Block reuptake by the releasing nerve, increasing neurotransmitter levels in the synaptic cleft.
Regulate receptor sites and neurotransmitter breakdown leading to increased concentrations in the synaptic cleft.
24. Classifications of Antidepressants
Selective serotonin reuptake inhibitors (SSRIs).
Tricyclic antidepressants (TCAs).
MAO inhibitors (MAOIs).
Serotonin norepinephrine inhibitors (SNRIs).
25. Selective Serotonin Reuptake Inhibitors (SSRIs)
25.1 Overview
Definition: Major class of antidepressant and anxiolytic medications increasing serotonin levels in the brain.
Advantages:
Effective for depression and anxiety.
Safer than older antidepressants (TCAs, MAOIs).
Better tolerated with fewer cardiovascular/anticholinergic effects.
25.2 Mechanism of Action
Process: SSRIs block the reuptake of serotonin (5-HT) into the presynaptic neuron, increasing serotonin availability at the synaptic cleft, enhancing mood, energy, and emotional regulation.
Key Concept for Nursing: SSRIs selectively affect serotonin, not norepinephrine or dopamine minimizing side effects compared to older antidepressants.
25.3 SSRIs Action & Indications
Actions:
Specifically block the reuptake of 5-HT with minimal known effect on norepinephrine or other receptors. (USUALLY TIRED FIRST)
Indications:
Depression, OCDs, panic attacks, bulimia, premenstrual dysphoric disorder, post-traumatic stress disorder, social phobias, social anxiety disorders.
26. Common SSRIs and Brand Names
Generic Name | Brand Name | Common Clinical Uses |
|---|---|---|
Fluoxetine | Prozac | Depression, bulimia, OCD, panic disorder |
Sertraline | Zoloft | Depression, PTSD, OCD, panic, anxiety |
Paroxetine | Paxil | Anxiety, depression, panic, OCD |
Citalopram | Celexa | Depression |
Escitalopram | Lexapro | Depression, generalized anxiety disorder |
Fluvoxamine | Luvox | OCD, social anxiety disorder |
27. SSRI Pharmacologic Profile
Onset of Action: 2–4 weeks for mood improvement, up to 6–8 weeks for full therapeutic effect.
Metabolism: Primarily hepatic (CYP450).
Elimination: Renal.
Dosing: Generally once daily (morning preferred to avoid insomnia).
28. Common Adverse Effects of SSRIs
System | Effect | Nursing Consideration |
|---|---|---|
CNS | Headache, insomnia, nervousness | May resolve after 1-2 weeks; take in AM. |
GI | Nausea, diarrhea, loss of appetite | Take with food if needed. |
Sexual | Decreased libido, delayed orgasm | Discuss openly; dose adjustment may help. |
Weight | Gain (paroxetine) or loss (fluoxetine) | Monitor weight regularly. |
Other | Dry mouth, sweating, tremor | Encourage fluids, oral care. |
29. Life-Threatening Reactions with SSRIs
29.1 Serotonin Syndrome
Cause: Excessive serotonin, can occur from SSRI combinations with other serotonergic drugs (MAOIs, St. John's wort, triptans, tramadol).
Symptoms: Agitation, confusion, tremor, muscle rigidity, hyperreflexia, diaphoresis, fever, tachycardia; severe cases can lead to seizures, coma, or death.
Nursing Priority:
Stop SSRI immediately.
Notify provider.
Provide supportive care (IV fluids, cooling, benzodiazepines for agitation).
29.2 Suicidal Ideation
Monitor especially in children, adolescents, and young adults during early treatment for mood changes, agitation, or self-harm thoughts; report changes immediately.
30. Contraindications and Precautions for SSRIs
Conditions:
Concurrent use with MAOIs or within 14 days of stopping.
Liver disease (reduced metabolism; dose adjustment needed).
Pregnancy (especially paroxetine; possible teratogenic effects).
Bipolar disorder (may trigger mania; requires mood stabilizer co-therapy).
Seizure disorder; glaucoma (SSRIs lower seizure threshold slightly).
31. Nursing Considerations for SSRIs
Before Administration: Assess baseline mood, suicidal thoughts, anxiety levels.
Obtain medication history (especially MAOIs, herbal supplements).
Monitor liver/renal function as indicated.
32. During Therapy Considerations for SSRIs
Check clinical improvement after 2–4 weeks.
Watch for serotonin syndrome with new medications.
Reinforce adherence—missed doses reduce effectiveness.
Educate that energy may improve before mood, increasing suicide risk.
33. Patient Education for SSRIs
Take daily at the same time, preferably morning.
Do not stop abruptly without provider supervision.
Avoid alcohol and other CNS depressants.
Report increased anxiety, agitation, or suicidal thinking.
Avoid St. John’s wort (increases serotonin levels).
Continue even if better; full effect takes time.
34. Tricyclic Antidepressants (TCAs)
34.1 Overview
Definition: Older antidepressants introduced in the 1950s; largely replaced by SSRIs and SNRIs due to side effects but still used for specific conditions.
Key Point: TCAs effective but have more side effects and higher toxicity risk in overdose.
34.2 Mechanism of Action of TCAs
Inhibit reuptake of norepinephrine and serotonin at synapses, thereby improving mood and emotional stability.
Also block acetylcholine (anticholinergic effects), histamine (sedation), and alpha-adrenergic receptors (hypotension)—explains their side effects.
Nursing Tip: Think of TCAs as “nonselective reuptake inhibitors.”
34.3 Common TCAs and Uses
Generic Name | Brand Name | Common Uses |
|---|---|---|
Amitriptyline | Elavil | Depression, chronic pain, insomnia |
Imipramine | Tofranil | Depression, childhood enuresis |
Nortriptyline | Pamelor | Depression, neuropathic pain |
Desipramine | Norpramin | Depression |
Doxepin | Sinequan, Silenor | Anxiety, depression, insomnia |
Clomipramine | Anafranil | Obsessive-compulsive disorder (OCD) |
35. Therapeutic Uses of TCAs
Treat major depressive disorder (MDD) when SSRIs/SNRIs ineffective.
Used for anxiety disorders, obsessive-compulsive disorder (OCD), chronic neuropathic pain, fibromyalgia, insomnia, migraine prophylaxis, and nocturnal enuresis in children (imipramine) IN CHILDREN).
36. Pharmacokinetics of TCAs
Absorption: From the GI tract.
Peak: 2-4 hours.
Binding: To plasma proteins, lipid soluble.
Metabolism: In liver; excreted in urine.
Half-Life: 8-46 hours.
37. Contraindications of TCAs
Known allergy, recent MI, myelography, pregnancy, and lactation.
38. Adverse Effects of TCAs
1. Anticholinergic Effects:
(Drying mouth” symptoms due to ACh blockade)
Dry mouth, blurred vision, constipation, urinary retention, tachycardia, confusion (especially in elderly).
2. Cardiovascular Effects:
Orthostatic hypotension, dysrhythmias, tachycardia (especially in overdose).
Nursing Tip: Monitor BP and heart rate, especially in older patients.
3. CNS Effects:
Sedation, drowsiness, dizziness, confusion, tremors, seizures (in high doses).
Nursing Tip: Administer at bedtime to minimize daytime drowsiness and fall risk.
4. Weight and Metabolic Effects: Weight gain (common) and increased appetite.
5. Sexual Dysfunction: Decreased libido, erectile or orgasmic dysfunction.
(GIVE AT BEDTIME, TO REDUCE DAYTIME DROWSINESS & FALL RISK)
39. Nursing Considerations for TCAs
Before Administration: Obtain mental health history, vital signs, cardiac history, baseline ECG (if older adult) (always monitor BP and HR).
Assess for suicidal ideation—risk highest when energy improves but mood remains low.
Review medication list for interactions.
During Administration:
Administer at bedtime due to sedating effects.
Monitor orthostatic BP changes; teach the patient to rise slowly.
Evaluate for dry mouth, constipation, urinary retention; ensure adequate fluid/fiber intake.
For enuresis, administer 1 hour before bedtime (imipramine).
40. Patient Education for TCAs
Take exactly as prescribed; do not double doses if missed.
Therapeutic effects may take weeks.
Avoid alcohol/CNS depressants.
Report cardiac symptoms (palpitations/chest pain) or urinary retention immediately.
Do not stop abruptly: withdrawal symptoms possible.
Store medications securely due to overdose risk (especially important for suicidal patients).
41. SNRIs (Serotonin–Norepinephrine Reuptake Inhibitors)
41.1 Overview
Definition: Increase serotonin (5-HT) and norepinephrine (NE) levels in the brain; used for treating depression, anxiety disorders, and certain chronic pain conditions.
Mechanism of Action: Inhibit reuptake of serotonin and norepinephrine at the presynaptic neuron, improving mood and reducing anxiety/pain sensitivity.
Its similar to SSRIs but also boost norepinephrine, which improve energy, concentration and pain perception
41.2 Common Drugs in SNRI Class
Generic Name | Brand Name | Key Uses |
|---|---|---|
Venlafaxine | Effexor XR | Depression, generalized anxiety disorder (GAD), panic disorder |
Duloxetine | Cymbalta | Depression, GAD, fibromyalgia, neuropathic pain |
Desvenlafaxine | Pristiq | Major depressive disorder |
41.3 Common Side Effects of SNRIs
Nausea, dry mouth, dizziness, headache, insomnia or somnolence, sweating, increased blood pressure (from norepinephrine), sexual dysfunction.
41.4 Serious or Cautionary Effects
Hypertension: Regular BP monitoring is critical.
Serotonin Syndrome: Particularly with SSRIs or MAOIs; symptoms include agitation and increased autonomic instability.
Withdrawal symptoms can occur if discontinued abruptly; taper slowly.
Suicidal Ideation: Early treatment phase requires close mood monitoring.
41.5 Nursing Considerations for SNRIs
Monitor vital signs regularly—especially blood pressure.
Inform patients about therapeutic effects taking 2–4 weeks.
Avoid sudden cessation; gradual taper needed to prevent withdrawal.
Instruct against concurrent alcohol/CNS depressants.
Look for signs of serotonin syndrome.
41.6 Adverse Effects of SNRIs
Nausea, constipation, hyperhidrosis, erectile dysfunction, tachycardia, vomiting, palpitations, serotonin syndrome, hypertension, abnormal bleeding, angle closure glaucoma, urinary retention.
Drug Interactions: Be cautious with MAOIs, SSRIs, TCAs, serotonergic drugs, aspirin, and NSAIDs.
42. Monoamine Oxidase Inhibitors (MAOIs)
42.1 Overview
Definition: An older antidepressant class for major depressive disorder, particularly for unresponsive cases; requires strict dietary precautions due to hypertensive crisis risk.
Mechanism of Action: Block monoamine oxidase, increasing norepinephrine, serotonin, and dopamine in the brain for improved mood stabilization.
42.2 Common MAOIs
Generic Name | Brand Name |
|---|---|
Phenelzine | Nardil |
Tranylcypromine | Parnate |
Isocarboxazid | Marplan |
Selegiline (transdermal patch) | Emsam |
42.3 Contraindications for MAOIs
Known allergy, pheochromocytoma, cardiovascular (CV) diseases, headaches, renal or hepatic impairment.
42.4 Major Adverse Effects of MAOIs
Hypertensive crisis (tyramine-rich food interactions).
Orthostatic hypotension, headache, dizziness, insomnia, weight gain, sexual dysfunction.
42.5 Drug-Drug Interactions of MAOIs
Concurrent antidepressants lead to hypertensive crisis or coma.
Increased sympathomimetic effects with Methyldopa (sympathomimetic effects increase).
Risk of hypoglycemia with insulin/oral antidiabetic agents (additive hypoglycemia).
42.6 Food Interactions with MAOIs
Tyramine-rich foods: Can cause severe hypertension due to norepinephrine release.
Foods to Avoid: Aged cheeses, cured meats, smoked/pickled foods, red wine, beer, soy products, avocados, overripe fruits, yeast extracts.
Hypertensive Crisis Signs: severe headache, neck stiffness, palpitations, nausea/vomiting, chest pain → medical emergency
42.7 Nursing Interactions for MAOIs
Educate on strict tyramine-free diet.
Avoid concurrent SSRIs, SNRIs, TCAs, or St. John's wort due to serotonin syndrome risk.
Ensure 14 days gap between MAOI and other antidepressants.
Regularly monitor blood pressure.
Teach to rise slowly to prevent orthostatic hypotension.
Do not stop suddenly; taper under supervision.
43. Other Antidepressants
Used when first-line treatments (SSRIs, SNRIs, TCAs, MAOIs) are ineffective, poorly tolerated, or to meet special clinical needs (e.g., smoking cessation, insomnia).
Examples:
Bupropion (Wellbutrin, Zyban)
Milnacipran (Savella)
Mirtazapine (Remeron)
Nefazodone (generic)
Selegiline (Emsam)
Trazodone (Desyrel).
43.1 Bupropion (Wellbutrin, Zyban)
Mechanism: Inhibits norepinephrine and dopamine reuptake; does not affect serotonin.
Uses: Depression, seasonal affective disorder, smoking cessation (Zyban), off-label ADHD treatment.
Nursing Considerations: Contraindicated in seizure disorders/eating disorders (anorexia/bulimia); side effects include dry mouth, insomnia, tremor, weight loss; minimal sexual side effects compared to SSRIs. Take in the morning to avoid insomnia
43.2 Milnacipran (Savella)
Mechanism: SNRI used primarily for fibromyalgia (not in the U.S. for major depression).
Nursing Considerations: Monitor for suicidal thoughts, potential serotonin syndrome, and avoid abrupt discontinuation to prevent withdrawal symptoms; possible side effects include nausea/constipation/increased heart rate.
43.3 Mirtazapine (Remeron)
Mechanism: Enhances norepinephrine and serotonin release by blocking presynaptic α-₂ adrenergic receptors; also blocks histamine receptors.
Key Features: Causes sedation and weight gain; beneficial in depressed patients needing improved appetite.
Side Effects: Increased appetite, drowsiness, dry mouth, elevated cholesterol.
Teaching: Take at bedtime to aid sleep
43.4 Trazodone
Mechanism: Serotonin antagonist and reuptake inhibitor (SARI) with sedative effects from histamine blockade.
Clinical Use: Low doses for sleep for sleep aid ; higher doses for antidepressant effects.
Key Adverse Effects: Sedation, dizziness, orthostatic hypotension, priapism (requires emergency care).
44. Psychothera peutic Agents
Functions: Used to treat psychoses such as schizophrenia, bipolar disorder, narcolepsy, and attention deficit disorder (ADD). * Drug do not cure the disorder
Effectiveness: Help patients manage symptoms, enabling more acceptable functioning and improved ADLs; utilized in both children and adults.
45. Schizophrenia Characteristics
Signs: Hallucinations, paranoia, delusions, speech abnormalities, affective problems.
Causes: Strong genetic association; may indicate a fundamental biochemical abnormality.
46. Bipolar Disorder Characteristics
Signs: Extremes of depression followed by hyperactivity and excitement.
Causes: Reflects a biochemical imbalance leading to neuronal instability.
47. Narcolepsy Characteristics
Symptoms: Daytime sleepiness, sudden loss of wakefulness.
Causes: Relate to stimulation problems by the reticular activating system (RAS).
48. Attention Deficit Disorders
Signs: Inability to focus on one activity for long; characterized by hyperkinesis (excessive involuntary, and often uncontrollably muscular activity or movement); usually diagnosed in school-aged children but can persist into adulthood.
49. Select Antipsychotic Agents
49.1 Traditional (First Generation) Antipsychotics
Examples:
Chlorpromazine (Thorazine), Fluphenazine (Prolixin, Permitil), Haloperidol (Haldol), Loxapine (Loxitane), Mesoridazine besylate (Serentil), Molindone (Moban).
49.2 Atypical (Second Generation) Antipsychotics
Examples:
Aripiprazole (Abilify), Clozapine (Clozaril), Iloperidone (Fanapt), Olanzapine (Zyprexa), Paliperidone (Invega), Quetiapine (Seroquel), Risperidone (Risperdal), Ziprasidone (Geodon).
49.3 Antipsychotic Drugs
Definition: Utilized primarily to treat schizophrenia; effective for more than just psychosis, assisting in manic episodes characterized by grandiosity, paranoia, and delusions.
Efficacy: These agents decrease hallucinations and delusions, aiding functional levels.
50. Overview of Antipsychotic Drugs
Functionality: Treating psychotic disorders (schizophrenia, bipolar disorder, severe depression).
Classification:
Typical (First-Generation): e.g., Haloperidol (Haldol), Chlorpromazine (Thorazine).
Atypical (Second-Generation): e.g., Clozapine (Clozaril), Risperidone (Risperdal).
Goals: controls symptoms such as hallucinations, delusions, agitation, and disorganized thought
50.1 Mechanism of Action
Typical Antipsychotics: Blocks D2 dopamine receptors—reduces positive symptoms of psychosis.
Mechanism: block dopamine D2 receptors in the brain→ reduced postive symptoms of psychosis
Atypical Antipsychotics: Block D2 and 5-HT2 serotonin receptors—addresses both positive and negative symptoms.
50.2 Risks of Antipsychotic Medications
Adverse Effects: Extrapyramidal symptoms (EPS): dystonia, akathisia, parkinsonism, tardive dyskinesia; neuroleptic malignant syndrome (NMS): fever, rigidity, altered mental status; sedation, hypotension, anticholinergic effects.
Nursing Care: Monitor adverse reactions like EPS and NMS; intervene immediately if NMS occurs.
Atypical (Second-Generation)
Antipsychotics
❖ Examples: Clozapine (Clozaril), Risperidone (Risperdal),
Olanzapine (Zyprexa), Quetiapine (Seroquel),
Aripiprazole (Abilify).
❖
Mechanism: Block dopamine (D2) and serotonin (5-
HT2) receptors → treat both positive and negative
symptoms.
❖
Advantages: Fewer EPS, improved mood and cognition.
❖
Major Risks: Weight gain, metabolic syndrome,
diabetes, hyperlipidemia.
❖
Teaching: Encourage healthy diet, monitor glucose and
lipids.
Contraindications
o Underlying diseases that could be exacerbated by
dopamine-blocking effects of these drugs
o CNS depression
o Circulatory collapse
o Parkinson’s disease
o Coronary disease
o Severe hypotension
o Prolonged QT interval
Clozapine (Clozaril)
❖ Special Considerations:
o Reserved for treatment-resistant schizophrenia.
❖ Risk of agranulocytosis (decreased WBCs).
❖ Monitor: CBC weekly for first 6 months, then biweekly.
o Report signs of infection (fever, sore throat)
immediately.
❖
Other effects: Weight gain, sedation, hypotension.
Haloperidol (Haldol)
❖ Use: Acute psychosis, agitation, Tourette’s syndrome.
❖
Adverse Effects:
❖ High risk for EPS and NMS.
❖
Nursing Interventions:
❖ Assess for muscle stiffness, rigidity, fever, and confusion.
❖ If NMS suspected → stop drug, maintain airway, apply
cooling measures, administer dantrolene or
bromocriptine per protocol.
Adverse Effects
o Sedation
o Weakness
o Tremors
o Constipation
❖ Drug-Drug Interactions
o Beta blockers, alcohol, anticholinergics, ziprasidone,
thioridazine
o Drowsiness
o Extrapyramidal
effects
o Dry mouth
o Nasal congestion
51. Common Adverse Effects of Antipsychotics
Sedation, weakness, tremors, constipation; specific drug-drug interactions (e.g., beta blockers, alcohol may enhance sedative effects).
52. Extrapyramidal Symptoms (EPS)
Types:
Dystonia: Involuntary muscle spasms (face, neck).
Akathisia: Restlessness, inability to remain still.
Pseudoparkinsonism: Tremors, rigidity, bradykinesia.
Tardive Dyskinesia: Involuntary movements (e.g., lip smacking).
Treatment: Introduce anticholinergic drugs (benztropine, diphenhydramine) for management; education on early recognition is critical for prevention.
53. Neuroleptic Malignant Syndrome (NMS)
Definition: A life-threatening emergency characterized by symptoms such as high fever, muscle rigidity, altered mental state, and autonomic instability.
Management: Immediate medication immediately , supportive therapies (fluids, cooling). Administer dantrolene or bromocriptine as necessary. Monitor: vitals signs, Ck levels, renal functions
54. Nursing Responsibilities for Antipsychotic Therapies
Baseline Assessment: Include mental status, vital signs, weight, lab values (glucose, lipids, CBC).
Monitoring: Observe for EPS, orthostatic hypotension, sedation, and metabolic changes.
Educations: adherence is critical, sudden withdrawal may worsen symptoms
Promote Safety: slow position changes, fall precautions
55. Overview of Bipolar Disorder
Definition: A chronic mood disorder with alternating episodes of mania and depression.
Goals of Treatment: Mood stabilization, relapse prevention, functional improvement.
Medication Classes: Include mood stabilizers, anticonvulsants acting as mood stabilizers, atypical antipsychotics, cautiously administered antidepressants.
56. Drugs for Bipolar Disorders
Medication | Uses |
|---|---|
Lithium (Lithobid) | Main mood stabilizer |
Aripiprazole (Abilify) | Atypical antipsychotic |
Lamotrigine (Lamictal) | Anticonvulsant/mood stabilizer |
Olanzapine (Zyprexa) | Atypical antipsychotic |
Quetiapine (Seroquel) | Atypical antipsychotic |
Ziprasidone (Geodon) | Atypical antipsychotic |
57. Mood Stabilizer: Lithium Carbonate
Mechanism: Alters sodium transport in neurons, stabilizing neurotransmission.
Therapeutic Range: 0.6–1.2 mEq/L; toxicity signs begin above >1.5 mEq/L.
Nursing Interventions: Regularly monitor lithium serum levels, renal, and thyroid function; maintain consistent sodium and fluid intake; educate on hydration to avoid dehydration.
58. Lithium: Key Nursing Considerations
Levels | Symptoms | Nursing Actions |
|---|---|---|
Less than 1.5 | Lethargy, muscle weakness | Assess for toxicity |
1.5-2 | ECG changes, nausea | Monitor regularly |
2-2.5 | Ataxia, seizures | Review patient status immediately |
>2.5 | Multiorgan toxicity | Push for immediate medical approval |
Lithium
❖Pharmacokinetics
o Absorbed from GI tract
o Peak in 30 minutes
o Distribution pattern in the body as water
o Slowly crosses the blood-brain barrier.
o Excreted from the kidney, 80% is
reabsorbed
o Crosses the placenta – associated with
congenital abnormalities
o Enters the breast milk
❖Contraindications
o Allergy, renal, cardiac disease, leukemia,
metabolic disorders, pregnancy, lactation
Assessment Action
Dehydration → Encourage fluids
Diuretics/NSAIDs → Avoid- raises lithium levels
Tremor, confusion → Assess for toxicity
Renal/thyroid → Monitor every 6 months
Nursing Considerations for
Antimanic Drugs
❖Assess:
o History and Physical Exam, known allergies
to lithium; renal or CV disease; dehydration;
sodium depletion, use of diuretics
o Protracted sweating, or diarrhea; suicidal
or impulsive patients with severe
depression; pregnancy or lactation; and
infection with fever CNS orientation, affect
o Urinary output, liver and renal function tests
o Serum Lithium levels
59. Nursing Responsibilities for Antimanic Drugs
Assess: mental and physical health history, allergies, kidney disease, CV disease, dehydration status; monitor urine output and lab levels carefully.
60. Anticonvulsants as Mood Stabilizers
Examples: Valproic acid (Depakote), Carbamazepine (Tegretol), Lamotrigine (Lamictal).
Mechanism: Modulate GABA and glutamate levels to stabilize mood.
61. Valproic Acid (Depakote)
Mechanism: Increases GABA levels for stabilize mood
Adverse Effects: Monitor renal function due to hepatotoxicity and pancreatitis; report weight gain and GI upset in patients.
62. Carbamazepine (Tegretol)
Mechanism: Reduces neuronal excitability via sodium channel inhibition.
Adverse Effects: Monitor CBC for possible bone marrow suppression; report signs of rash or fever.
63. Lamotrigine (Lamictal)
Mechanism: Modulates glutamate release in the brain.
Adverse Effects: Beware of rashes; Stevens-Johnson syndrome risk requires immediate action if detected.
Teaching: titrate slowly, stop immediately if rasg develops
64. Atypical Antipsychotics Overview
Examples: Olanzapine, Risperidone, Quetiapine, Aripiprazole.
Mechanism: Block both dopamine and serotonin receptors for effective amenity.
Uses: Treat acute mania, bipolar depression, and maintenance therapy.
Adverse Effects: Pay attention to weight loss/gain, monitoring glucose for hyperglycemia /lipid changes in high-risk patients.
65. Antidepressants in Bipolar Disorder
Use only short-term for depressive episodes and always in combination with mood stabilizers to prevent mania.
Examples: Fluoxetine (Prozac), Sertraline (Zoloft).
66. Key Takeaways
Be alert for lithium toxicity; withhold dose upon suspicion.
Regularly monitor liver functions for those prescribed valproic acid.
Report fever/sore throat in patients administered carbamazepine → possible agranulocytosis.
Titrate lamotrigine slowly, with immediate discontinue if upon rash appearance.
Central Nervous System Stimulants
67. Actions of CNS Stimulants
Mechanism of Action:
Act on cortical and the reticular activating system (RAS), potentially through releasing catecholamines from presynaptic neurons, leading to increased stimulation of postsynaptic neurons.
Indications:
Treatment of attention-deficit syndromes; narcolepsy management.
68. Overview of CNS Stimulants
Mechanism: Increase the levels of dopamine, norepinephrine, and serotonin in the CNS.
Therapeutic Uses:
ADHD, narcolepsy, and short-term obesity treatments (appetite suppression).
Note: These are controlled substances with a potential for high abuse.
69. Amphetamine and Dextroamphetamine (Adderall)
Mechanism: Promotes norepinephrine and dopamine release, increasing alertness and focus.
Uses: Effective for ADHD and narcolepsy.
Side Effects: Insomnia, weight loss, tachycardia, hypertension, irritability.
Teaching Points: [Take in the morning, monitor appetite/weight, avoid caffeine/stimulants, do not discontinue abruptly].
70. Methylphenidate (Ritalin, Concerta)
Mechanism: Blocks reuptake of dopamine/norepinephrine.
Uses: Indicates ADHD and narcolepsy; assess growth in children.
Adverse Effects: Decreased appetite, insomnia, tachycardia, nervousness; follow signs of abuse.
71. Modafinil (Provigil)
Mechanism: Enhances wakefulness by altering dopamine pathways.
Uses: Effective for narcolepsy, shift-work sleep disorder.
Side Effects: Headache, insomnia, nausea, anxiety.
Teaching: Administer in the morning; caution for driving until side effects are clear.
72. Phentermine (Adipex-P, Suprenza)
Mechanism: Enhances norepinephrine/dopamine release and suppresses appetite.
Use: Short-term obesity management alongside dietary changes and exercise.
Adverse Effects: Increased heart rate, elevated BP, insomnia, nervousness, dry mouth; contraindications include cardiovascular conditions and diabetes.
73. Phentermine Teaching Points
Administration must be in the morning to preempt insomnia.
Avoiding caffeine/stimulants; short use duration only (few weeks) with dietary/exercise integration needed.
74. Non-Stimulant ADHD Medications
Example: Atomoxetine (Strattera).
Mechanism: Functions as a selective norepinephrine reuptake inhibitor (SNRI).
Advantages: Lower abuse potential; less controlled substance nature.
Adverse Effects: Fatigue, GI upset, and potential suicidal ideation risks in children.
Nursing Care: Monitor mood changes and liver toxicity.
75. Stimulants Nursing Implications
Monitor: HR, BP, weight, overall growth.
Assessment: Quality of sleep, appetite, psychiatric changes.
Teaching: Restrict evening dosing, limit caffeine intake, report chest pain or palpitations.
Promote adherence: Safety protocols around controlled dosing.
76. Stimulants Contraindications & Precautions
Contraindications: Severe anxiety, agitation, cardiac disease or arrhythmias, hyperthyroidism, history of substance abuse.
Caution: MAO inhibitors risk of hypertensive crisis; standard protocol should be maintained.
77. Commercially Available Stimulants
Drug (Brand name) | Indication | Risks |
|---|---|---|
Dextroamphetamine (Dexedrine, others) | ADHD | Contraindicate in substance abuse, cardiac disease, hyperthyroidism |
Amphetamine/dextroamphetamine combinations (Adderall, others) | ADHD | |
Methyphenidate (Ritalin, Concerta, others) | ADHD, narcolepsy | |
Phentermine (Adipex-P, others) | Obesity | |
Phendimetrazine (Bontril, others) | Obesity | |
Modafinil (Provigil, others) | Narcolepsy |
78. Key Takeaways
CNS stimulants significantly boost CNS activity, improving suspension.
Major risks include adverse effects and the potential for abuse.
Nurses play pivotal roles in monitoring growth, vitals, and mental health side effects, ensuring safe compliance.
Pain
Sensory and emotional
experience associated
with actual or potential
tissue damage
❖ Acute or chronic
❖ Drugs Used to Relieve Pain
o Narcotics: Opium
derivatives used to treat
many types of pain
o Antimigraine Drugs:
Reserved for the
treatment of migraine
headaches
Pain Receptors
❖ Opioid receptors
o CNS
o Nerves in the periphery
o Cells in the
gastrointestinal (GI) tract
Pain is a subjective experience mediated by nociceptors.
❖ Drug classes used for pain:
o Narcotic (opioid) agonists.
o Narcotic antagonists and mixed agents.
o Non-opioid analgesics (NSAIDs, acetaminophen).
o Anti-migraine agents (triptans, ergots).
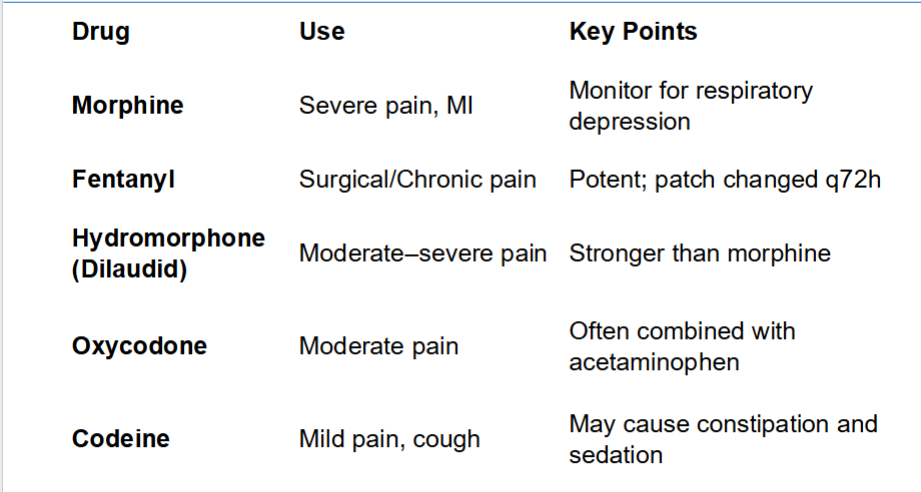
Narcotic (Opioid) Agonists
❖ Examples: Morphine, Fentanyl, Hydromorphone,
Oxycodone, Codeine.
❖
Mechanism: Bind to mu and kappa opioid receptors,
altering perception and response to pain.
❖ Therapeutic Uses: Moderate to severe pain, anesthesia
adjunct, acute MI, cancer pain.
❖ Adverse Effects: Respiratory depression, constipation,
sedation, hypotension, urinary retention.
Nursing Responsibilities for Narcotics
❖ Assess pain level, respiratory rate, and sedation level
before administration.
❖ Hold if RR < 12/min; notify provider.
❖ Administer slowly IV to prevent respiratory depression.
❖ Encourage fluids, fiber, and ambulation to prevent
constipation.
❖ Use stool softeners as needed.
Narcotic Antagonists
❖ Example: Naloxone (Narcan).
❖
Mechanism: Competes with opioids at receptor sites,
reversing respiratory and CNS depression.
❖ Use: Opioid overdose, postoperative respiratory
depression, newborn resuscitation.
❖ Nursing Care:
o Administer IV, IM, or intranasal.
o Onset 1–2 min IV.
o Monitor for return of pain and withdrawal symptoms.
Mixed Agonist-Antagonist Opioids
❖ Examples: Butorphanol (Stadol), Pentazocine (Talwin).
❖
Mechanism: Stimulate kappa receptors, block or weakly
stimulate mu receptors.
❖ Use: Moderate pain, labor pain, pain with lower risk of
respiratory depression.
❖ Nursing Note: Can precipitate withdrawal in opioid-
dependent patients.
Opioid overdose- Key actions
❖ Signs: Respiratory rate < 10, pinpoint pupils,
unresponsiveness.
❖
Nursing Interventions:
❖ Administer Naloxone immediately.
❖ Support airway, oxygenation, and monitor vital signs.
❖ Reassess frequently—Naloxone’s half-life is shorter than
many opioids.
Migraine Headaches
o Severe, throbbing
headaches on one
side of the head
o Common
o Classic
❖ Cluster Headaches
o Begin during sleep; involve sharp, steady
eye pain, sweating, flushing, tearing, and
nasal congestion
❖ Tension Headaches
o Usually occur at times of stress; dull band
of pain around the entire head
Anti-Migraine Medications: Overview
❖ Pathophysiology: Migraine pain caused by cranial
vessel dilation and inflammation.
❖
Drug Classes:
o Triptans (Serotonin 5-HT1 agonists) – cause
vasoconstriction.
o Ergot derivatives – older drugs, constrict
intracranial vessels.
o Preventive agents – beta-blockers,
anticonvulsants, supplement “cocktails”
Triptans (Sumatriptan, Rizatriptan)
❖ Mechanism: Stimulate 5-HT1 receptors → cranial
vasoconstriction and decreased neuroinflammation.
❖ Use: Acute migraine attacks (not prevention).
❖
Adverse Effects: Chest tightness, dizziness, tingling,
hypertension.
❖ Contraindications: Coronary artery disease,
uncontrolled hypertension.
Ergotamine (Ergomar) and
Dihydroergotamine (DHE)
❖ Mechanism: Vasoconstriction of dilated cranial blood
vessels.
❖ Adverse Effects: Nausea, vomiting, muscle pain,
tingling in extremities.
❖ Toxicity (Ergotism): Peripheral ischemia—cold, pale
extremities, numbness.
❖ Teaching: Avoid use with triptans within 24 hours
(severe vasospasm risk).
Nursing Responsibilities for Pain
Medications
❖ Assess pain and sedation before/after administration.
❖ Monitor vital signs and level of consciousness.
❖ Evaluate for side effects: respiratory depression,
constipation, orthostatic hypotension.
❖ Educate on safe storage, use, and risk of dependence.
❖ Teach early intervention for migraine and avoidance of
triggers.
Key Takeaways
❖ Opioid agonists: effective for severe pain; monitor for
respiratory depression.
❖ Naloxone: life-saving reversal agent.
❖ Anti-migraine meds: triptans for acute attacks, ergots as
older options.
❖ Nurses play a vital role in assessment, safety, and
education.