Forensic Psychology and Speech and Language Therapy
Definition of Forensic Psychology
According to the British Psychological Society, Forensic Psychology is defined as:
“the application of psychology within the legal system to create safer communities and to assist people to find pathways away from criminal behaviour.”
Forensic Psychologists operate in various settings, including:
HM Prison and Probation Service
Hospitals
Secure children’s homes
Police forces
Courts
Universities
Responsibilities of Forensic Psychologists:
Assess (the level of risk- risk of offending), formulate (working hypothesis- understand the reasons), and intervene (personalize individualized treatment) with people engaging in harmful behaviours.
Provide advice and expertise to other professionals.
Develop and deliver training programs.
Provide therapeutic interventions aimed at contributing to a safer society. Manage in a custodial and community environment
Psychiatry versus Psychology
Psychology
Focuses on the study of the mind, emotions, and behaviour.
Examines cognitive and social factors that influence actions, reactions and behaviour.
Primarily offers therapeutic interventions. Self skills and managing behaviour.
Psychiatry
Concentrates on diagnosis and treatment of mental health disorders.
The term psychiatry is defined as:
“medical treatment of the soul.”
More likely to offer medications compared to psychologists.
Forensic Psychology vs Clinical Psychology
Clinical Psychology
Focuses on diagnosis and treatment of mental health disorders similar to forensic psychology, with the addition of therapeutic interventions aimed at individual well-being.
Clinical psychologists may not always work in criminal contexts as forensic psychologists do. Work more on the treatment.
Both forensic and clinical psychologists in settings like NHS and HMPPS are trained in trauma therapy, including EMDR (Eye Movement Desensitization and Reprocessing)- who have traumatic experiences and to deal with that trauma.
Forensic and clinical psychologists may engage with different types of trauma or different impacts of trauma. Depending on the risk determines who works with the service user.
Other Areas of Psychology
Psychologists specialize in various fields, including:
Educational psychology
Counselling psychology
Occupational psychology
Neuropsychology
Sports psychology
Role of Speech and Language Therapists in the Criminal Justice System
Have a communication need. Can self-refer or be referred with who is working with the service user.
What do Speech and Language Therapists (SLTs) look for?
Attention and listening skills- ADHD (impulsive behaviour). Undiagnosed can have an impact.
Age-appropriate vocabulary
Ability to decode sentences
‘Thinking time’ to process information
Ability to find words and construct sentences matching thought
Following rules of social interaction
Memory capabilities- OT.
Reading body language and tone of voice
Reasonable adjustments. Becoming neuro-affirming and what is typical for that individual. Educating others.
DLD
Stroke, huntingtons, parkisons.
Challenges faced by individuals in the Criminal Justice System (CJS):
Often people have experienced:
Social disadvantage
Poor education
Adverse childhood experiences (ACEs)
Head injuries
Substance misuse
ADHD, Learning disabilities, Autism- working with learning disability nurse.
Poor mental health- how does it impact on their communication.
SLT Interventions:
Create an engaging environment for comprehension and engagement- universal level. What can other people do in that environment to support the service user. Consistency of staff may be a challenge- continuity of making it a communication friendly environment.
Gather pertinent case history information- individual, referrer.
Make a profile about the service user and a report with reasonable adjustments. Consent to share the report and profile e.g. probation offender manager, community offender manager (will need to do interventions once they are released)
Conduct assessments.
Set goals and support skill acquisition.
Communication access training and ‘‘The Box’ training. Working with the youth justice system.
SLT’s deliver training for the forensic psychology team to support with interventions. Also helps with understanding the concepts.
Collaboration Between Forensic Psychologists and SLTs
SLT Perspective on Presenting Problems:
Is the issue related to communication needs?
How can we enhance the communication environment for the individual?
What knowledge needs to be shared for successful interactions?
Using the “what works for me” to device strategies for interventions e.g. understanding concepts (blank levels), executive disfunction.
Forensic Psychologist Perspective on Presenting Problems:
Is the issue related to thoughts, feelings, and choices? Internal feelings that influence their choices? Managing their behaviour.
Is the individual at risk? Financial, relationships?
What factors are keeping the problem going?
Conduct a “what works for me” form to enable them to understand the individuals risk factors and tailoring these to meet their individual needs.
Collaborative Goal:
Combine ideas to achieve the best outcomes for individuals in the CJS.
Formulation in Psychology
Definition of Formulation:
A case formulation is a hypothesis (working narrative) describing the nature and causes of an individual's harmful behaviour.
Aims to identify influences on behaviour to explain development and progression of that behaviour. Genetic dispositions, physical or mental health conditions, trauma, substance misuse, psychological, environment, social support and relationships, cultural backgrounds.
Targets specific factors to help reduce risk associated with harmful behaviour. Can be revisited and adapted as the person changes or journey evolves.
Formulations can be revisited and amended as new information becomes available.
Interviews, observations, reports (ways of gathering information).
Objectives of Case Formulation:
Identify patterns or themes in an individual's life related to harmful behaviour.
Key question: What does the individual gain from their harmful behaviour? Explain the why.
This is known as the ‘function’ of their behaviour. What is it serving that person? What can it be giving that education (communication).
Benefits of the Formulation Process
For Service Users:
Enhances the therapeutic relationship with professionals- good working allience. Moving away from the clinical exercise. Provides a personalized understanding of the client's needs and encourages active participation in their own treatment plan.
Increases motivation for engagement in therapy.
Fosters hopefulness reduces self-blame/ shame. Normalizing those experiences- giving a sense of empowerment of their story. Help them make the connections. Helps release the anxiety.
Provides a sense of support.
Helps visualize a way forward.
For Professionals:
Improved understanding of service user problems.
Facilitates more positive interactions with service users. Provides them a better understanding of the individual. Helping them understand their behaviour.
Encourages greater empathy for service users.
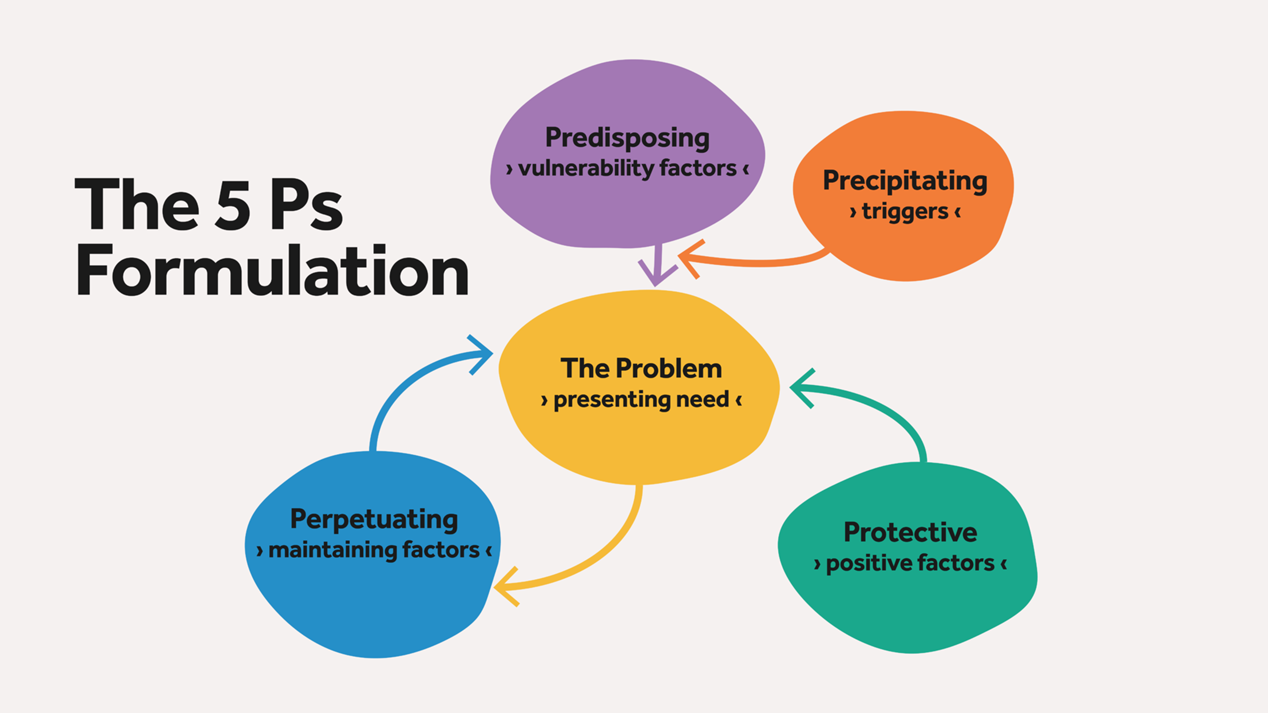
The 5P’s Model of Formulation
Components of the 5 Ps in Formulation:
The Problem- presenting: The specific presenting need or issue.
Predisposing factors: Vulnerabilities that may contribute to the individual’s issues e.g. genetic disposition, events that have happened and how they have reacted to these, educational history. What happens in the early years.
Precipitating factors: Triggers that bring about the harmful behaviour. What happens before to the triggering behaviour. Triggering problems that they have been facing, the individuals coping strategies that they have learnt to use.
Perpetuating factors: Elements that sustain the problem (making it worse), how they view themselves, others or the world. The use of substances.
Protective factors: Aspects that can aid in the individual's coping mechanisms- this can get lost when all of the harmful behaviours take over. Engaging well in interventions, good relationships with others. Important to look out for these.
Example Formulation: Tom’s Case
Background of Tom (20 years old):
Placed in care at 3 months old; siblings placed in separate care.
Violent treatment by father; returned to care after an unstable upbringing.
Homelessness for two years post-17 years.
Substance use began at 8 (cannabis) and 11 (alcohol); has used various hallucinogens.
Diagnosed with ADHD; previously received Concerta medication but currently not taking it.
Traits of autism not diagnosed.
Engaging in self-harm since age 15; currently in prison for violent offences.
Struggles with prison environment; displays aggression and self-harm as coping mechanisms.
Relationships with certain staff help manage interactions.
Presenting Problems:
Damaging furniture, self-harming, aggression towards staff.
5P’s in Tom’s Formulation:
Predisposing Factors:
History in care; lack of attachment; exposure to violence; potential brain injury.
Precipitating Factors:
Substance use; ADHD; possible autism; lack of communication about changes; aggression from staff.
Perpetuating Factors:
Lack of medication; inability to express needs; distress management issues; negative relationships with staff.
Protective Factors:
Positive relationships with specific individuals; engagement with therapy.
The Importance of Developing a Formulation
Strategic Interventions:
Fine-tuning the environment to reduce triggers and pressures on the individual.
Maintenance of protective factors to enhance coping abilities- see the worth of these and to monitor/ self-reflect on these.
Formulation leads to intervention plans aimed at helping the individual navigate their issues.
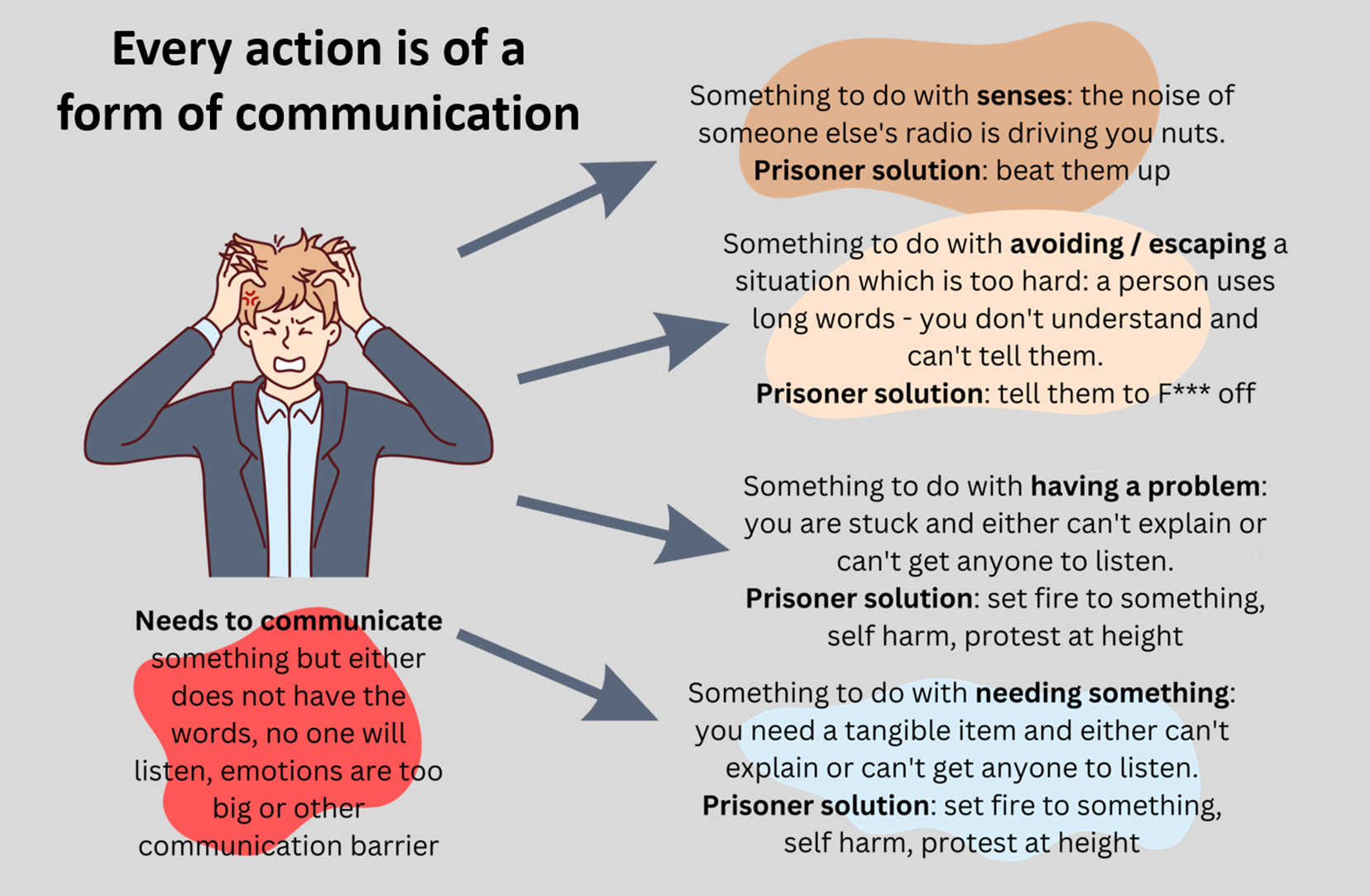
Communication and Behaviour
Type of Communication as Behaviour:
Every action is considered a form of communication. May not have the words, no one will listen, emotions are too big or a communication barrier.
For example:
Disturbances of the senses (noisy neighbors) leading to negative reactions (violence).
Misunderstanding language leading to frustration and aggression.
Ultimately, many communication barriers may result in harmful actions as reactions to unmet needs.
Behaviour is managed with an IEP.
Encourage staff to look deeper at what is going on - formulation on what is driving their behaviour. What could they be doing that triggers or perpetuate their behaviour.
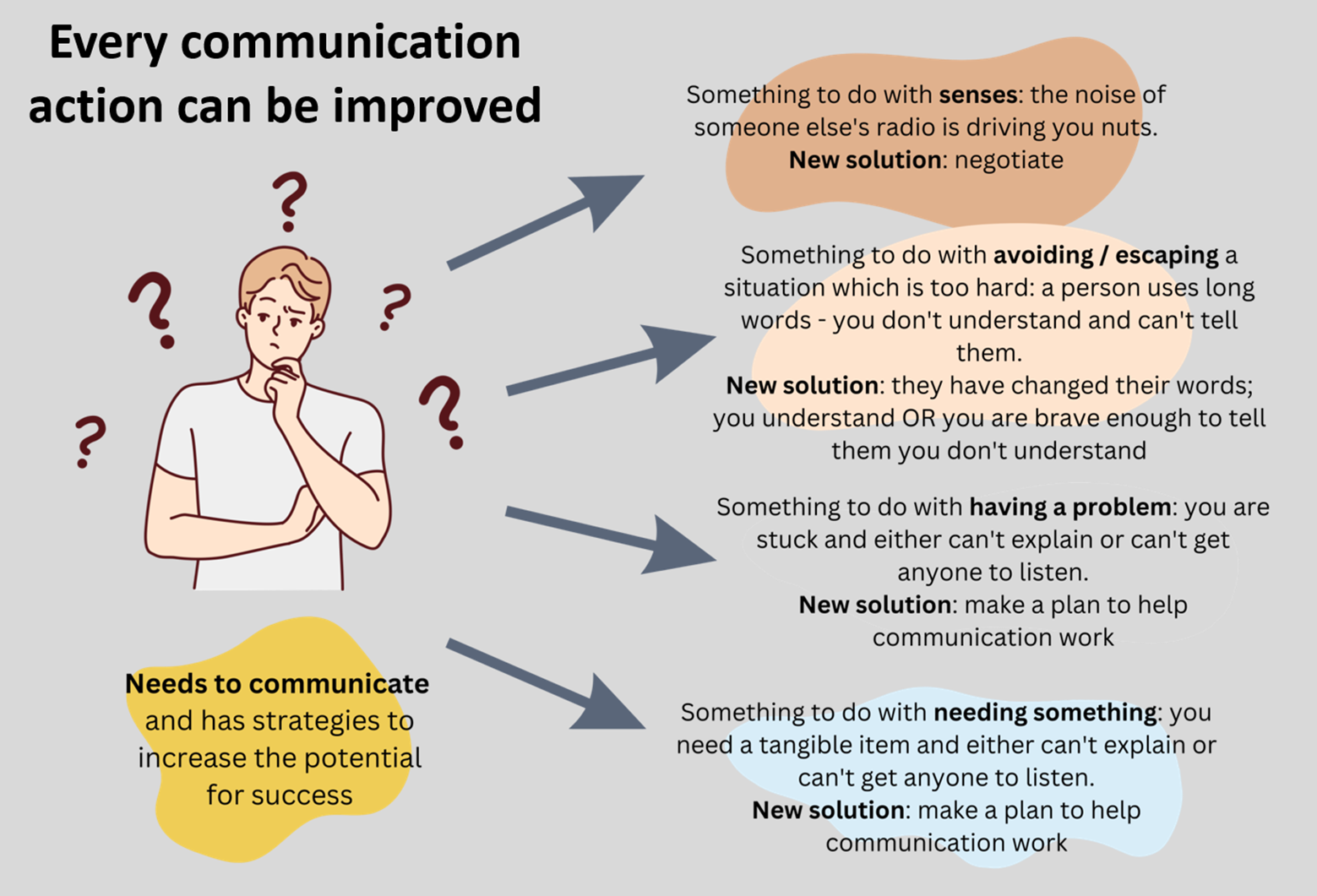
Improving Communication Strategies
Strategies to enhance communication:
Learn to problem solve and deal with a situation.
Engage in negotiation rather than aggression.
Simplify language to ensure understanding.
Develop communication plans that aid expression and comprehension.
Ability to mask difficulties.
Advocate for themselves.
Understanding the Limbic System
Orientation to Limbic System's Role:
Consider how personal experiences affect emotional and behavioral responses.
Links between experiences of violence, care, and subsequent behavior manifest in the limbic system.
Neurological- emotional and cognitively. This will affect how to interact and support them.
Hypervigilance- always heightened.
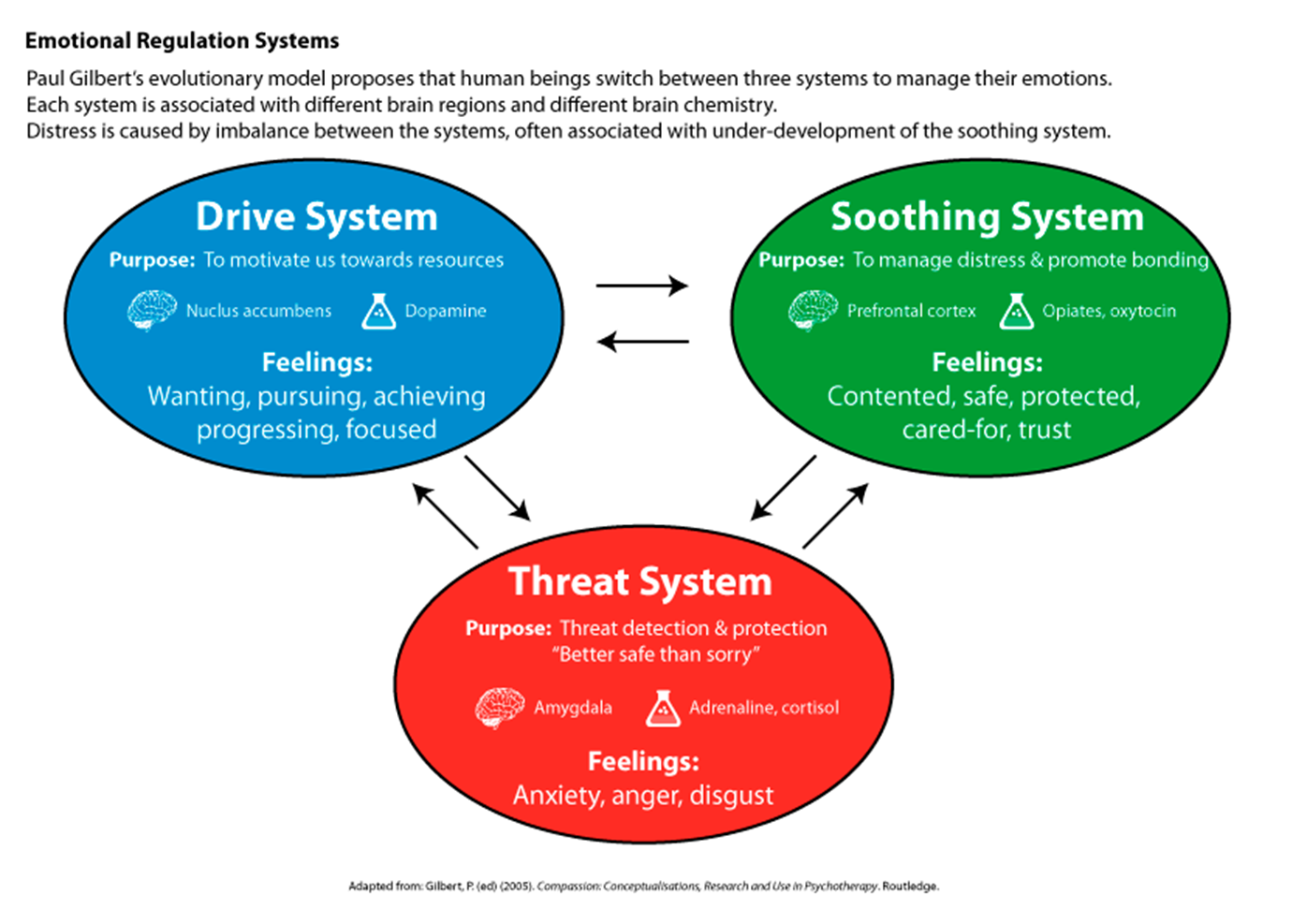
Emotional Regulation Systems
Paul Gilbert's Evolutionary Model:
Human beings utilize three systems for emotional management:
Drive System: Motivation toward resources; associated with dopamine.
Feelings: Want, achievement, focus. Pleasure response. Motivating. Seen as a positive.
Soothing System: Manages distress, promotes bonding; associated with opiates, oxytocin. Contentment, protection.
Feelings: Safety, trust, caring.
Threat System: Detects threats, protects; associated with adrenaline, cortisol.
Feelings: Anxiety, anger, disgust, appease against perceived threat
Consequences of Imbalance:
Distress may arise from underdevelopment of the soothing system leading to maladaptive behaviors.
The model helps identify what is going on in the individuals life. See how past experiences can impact their behaviours. Can get them to map out to see what the stresses they have experienced.
Relevance to the Role of SLT
Interventions focusing on self-advocacy and acceptance therapy may benefit service users- clinical psychologist.
SLTs should employ trauma-informed approaches during involvement. Nurturing relationship and consistently supporting. Advocating to others what they need.
Visual resources (like comic strips) can aid understanding and communication breakdowns. Talking mats. Consequences of actions.
Consideration of emotional literacy
Non-verbal communication skills is imperative. How skilled are they?
Recall past memories and form memories- use of visuals and strategies.
Joint Working in the Criminal Justice System
Collaboration Opportunities:
Referrals to SLT when appropriate- clinical psychologists?
Consultation and information sharing- how they can support the person.
Provision of insight from SLT to inform patient interactions.
Support engagement in therapeutic interventions
Conduct case reviews- building a person’s profile.
Multi-disciplinary team working (MDT)