lect 8: airborne bacterial diseases
Transmission Introduction
spread of infection affected by 2 major factors: reservoir (where bact grow) and mech of transmission (how they move from reservoir)
3 main types of pg transmission
1. contact - indiv are exposed by touching or being close to something infected, 3 subtypes:
direct - no intmd btwn infected and healthy, shared thru kissing, sex, etc
indirect - nonliving articles called fomites used as intmd like needles, tissues, bedding, etc
droplet - usually for respiratory diseases, spread thru sneaking, coughing, or laughing. the size of the droplet is important as smaller ones stay airborne longer = dangerous
2. vehicle - use something like a doorknob, table, or nonliving surface to spread, pg rides on “clean” components like air, food, water, bodily fluids, drugs, blood, etc.
3. vector - use intmd like animal to spread to the target host, not responsible for only carrying but plays role in life cycle, codept on intmd
Airborne Diseases
can breathe in or have on skin
usually transmitted via short distances
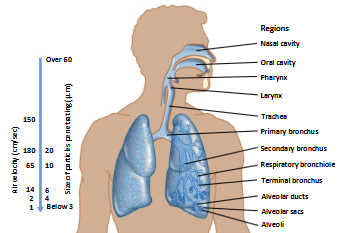
diff pg infect diff parts of respiratory tract → diff environ that favor diff mo
impacts how far they’re expelled and the droplet size
upper resp tract - expelled faster, droplet size is larger
lower resp trast - expelled slower, droplet size is smaller
Corynebacterium diphtheriae → Diphtheria
most well known for an endemic in Nome, Alaska - used sled dogs to transport antitoxin (movie Balto based on)
disease manifests diff based on colonization site
nasal - common cold, mild
tonsillar - most common, low grade fever, pdce membrane in throat, can progress to cause severe symptoms, can kill
laryngeal - can also be deadly, extension of pharyngeal / tonsillar infection
can damage heart, nerves, etc
only known reservoir is humans
associated with IV drug use
transmitted via droplets or contact with an open wound / skin infection
usually co-infects with staph. aureus and strep. pyogenes
pdces an AB toxin when infected by a phage that causes it to be a pg
without the phage, there’s no infection bc the phage gives the vf
tox+ phage integrates into the bact genome, activating vf and pdces AB toxin
it inhibits EF2 and stops protein synthesis
bact requires Fe for growth so it uses its own Fe scavenging protein (corynebactin)
the tox gene in the phage is activated by low [Fe] so corynebactin and tox expr is activated at same time
tf that represses tox gene is activated by high [Fe]
Diphtheria Immunization
using a toxoid can generate ab that neutralize the active toxin
want toxoid against active toxin not just the A, B, or T su cause then it won’t be effective in active infection
neutralizing ab - block toxin’s function by binding to critical sites
precipitation ab - toxins form insoluble complexes with ab
mechs of neutralization of Cd toxin
1. binding at or near A su active site
2. blocking the receptor binding site on the B su
3. inhibit endosomal transl by binding hydrophobic domain (T)
Focus On
upper vs lower resp tracts
diphtheria manifests diff dept colonization site
reg of toxin expr and mech of diphtheria toxin action
immune protection against diphtheria