Musculoskeletal Block: The Skull and Vertebral Column
L.O. Describe the major features of the bones of the skull, mandible and the temporomandibular joint (TMJ)
L.O. Describe the major groups that the major muscles of the head and neck fall int - muscles of facial expression, muscles of mastication etc.
‘Adduction is the movement of a limb or body part towards the midline of the body, while abduction is the movement away from the midline’
The Skull
Bones of the Skull (10 all together)
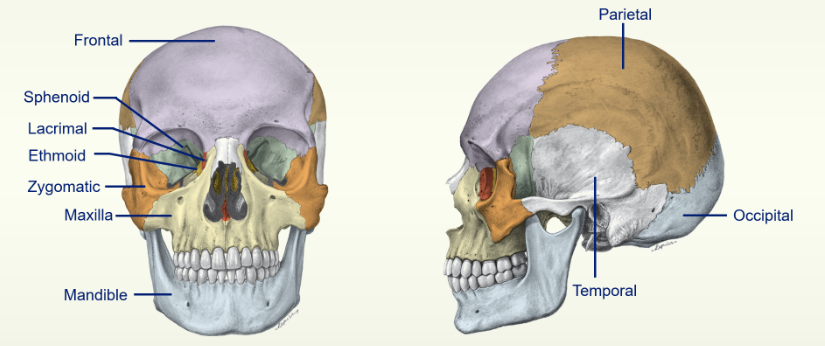
Sutures of the Skull: (6 all together)
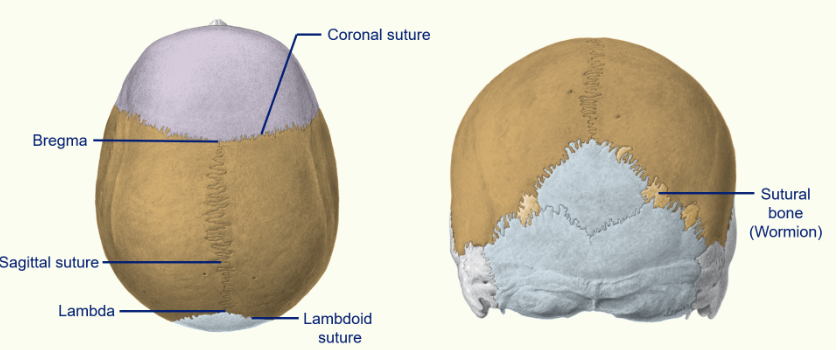
between the parietal bone and the occipital bone, we have our lambdoid suture
where the sagittal suture joins the coronal suture - we call this the bregma
where the sagittal suture joins the lambdoid suture - we call this the lambda
the bregma (anterior fontanelle) and lambda (posterior fontanelle) are soft spots in neonate heads - this allows the brain to continue growing after birth
Bones of the Skull (inside the skull)
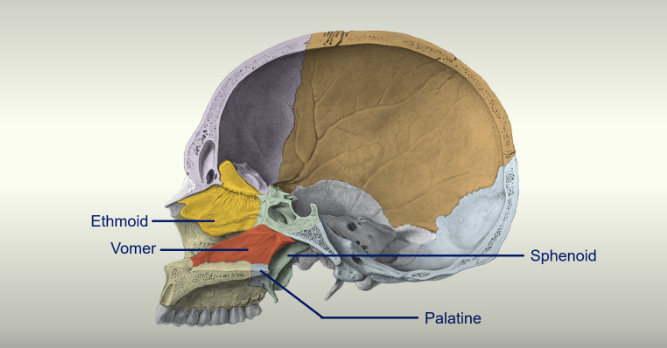
There are 2 new bones here which can be seen in this sagittal cross section of the skull
Vomer
Palatine bone - makes the posterior part of the hard palate
the ethmoid bone makes up the superior part of the nasal cavity whilst the vomer bone makes up the inferior part of the nasal cavity
Cranial Fossae and the Foramen
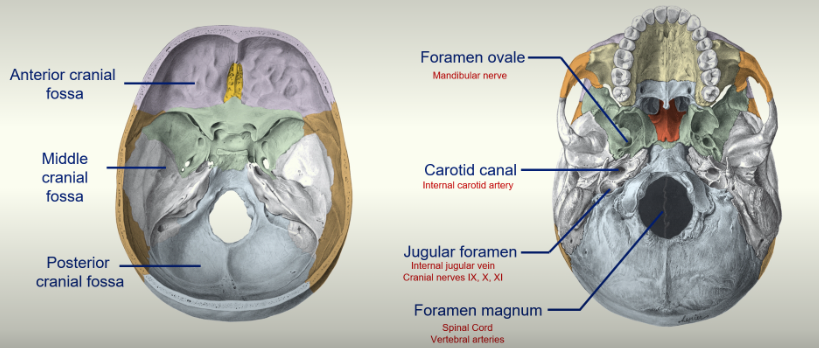
the cranial cavity divides itself naturally into three parts:
Anterior cranial fossa
Middle cranial fossa
Posterior cranial fossa
the foramen are crucial for allowing vascularisation of the brain
a lot of things need access to the brain
Major Foramen:
Foramen Ovale : Mandibular nerve passes through here.
Foramen Magnum: the spinal cord goes through here and becomes the brain stem. The vertebral arteries also go through here
Jugular Foramen: internal jugular vein and cranial nerves IX, X, XI pass through here.
Carotid Canal: internal carotid artery passes through here.
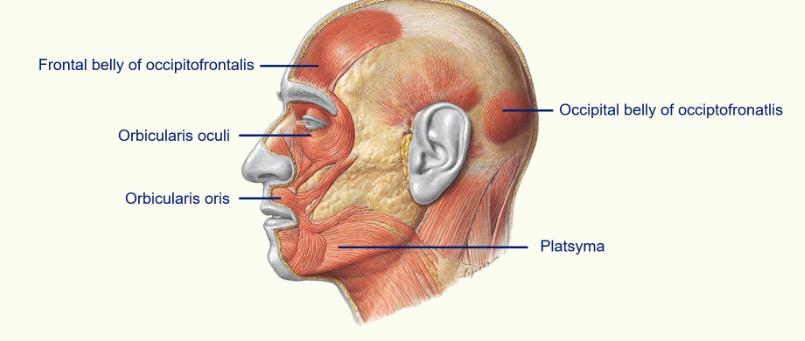
Muscles of Facial Expression
unique muscles within the body - they are subcutaneous and insert directly into the skin
they are responsible for moving the skin to provide facial expression, but also act as sphincters around the eyes and mouth
supplied by cranial VII - the facial nerve
the thickness, position etc of the muscles vary greatly between people
The Major muscles you should know are:
Orbicularis Oculi - this surrounds the eye and is one of the sphincter muscles which helps close the eye.
Orbicularis Oris - this surrounds your mouth and helps to pucker your lips.
Platsyma - goes all the way to your neck and helps to depress the angles of your mouth
Occipitofrontalis - this is the muscle on your scalp and it is divided into the frontal belly and occipital belly - connected by an aponeurosis ( a large flat tendon)
The Facial Nerve
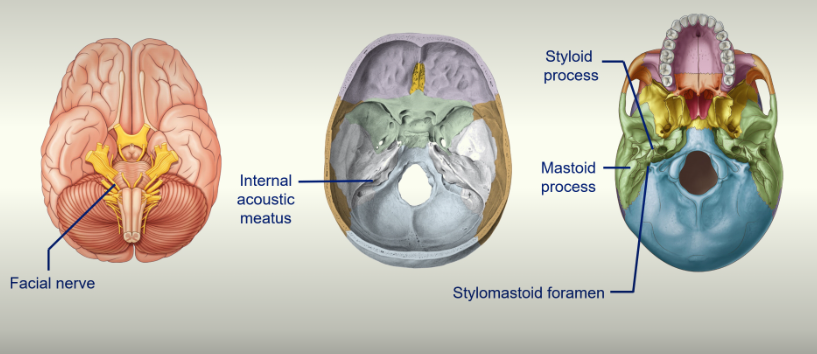
the facial nerve travels through the internal acoustic meatus and then through the mastoid process
the facial nerve comes out of the mastoid process, travels through the Parotid gland and moves superficially because our muscles are superficial
the facial nerve divides into 5 distinct different branches:
Temporal branch
Zygomatic branch
Buccal branch
Marginal mandibular branch
Cervical branch
Bell’s Palsy
paralysis of facial nerve
causes drooping of face
can’t close eyelid or eyelid droops
difficulty closing mouth
Muscles of Mastication
normal skeletal muscle
responsible for moving the mandibular at the Temporomandibular joint
supplied by cranial nerve V - the trigeminal nerve
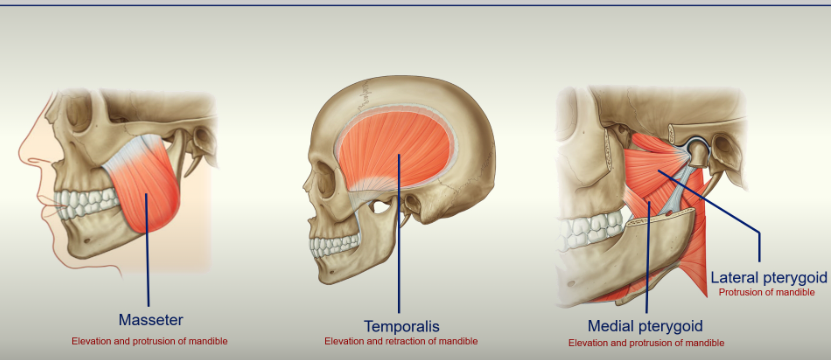
these muscles attach bone to bone (normal skeletal muscle)
1. Masseter - elevates mandible and protrudes your mandible. Powerful muscle.
Temporalis - sits on the side of your head, over your temporal bone. Inserts into the pterygoid process - elevates and retracts mandible.
Medial pterygoid - elevates and protrudes mandible.
Lateral pterygoid - protrudes mandible
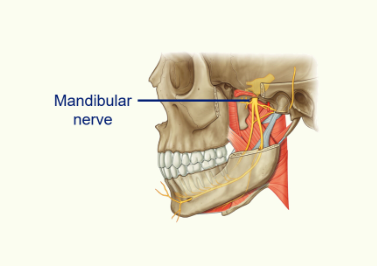
The Mandibular Nerve and Trigeminal Nerve
the Mandibular Nerve is a branch of the Trigeminal Nerve
the Trigeminal Nerve is sensory to the face and scalp as far back the vertex (supplies the skin of these areas and orifices such as nasal and oral cavities)
it also has a motor function to the muscles of mastication
The Trigeminal Nerve has 3 major branches
Ophthalmic Nerve
Maxillary Nerve
Mandibular Neve - supplies the muscles of mastication - mixed as it has sensory neurones going to the skin and motor neurones going to the muscles of mastication.
Pharyngeal Arches
why are there different nerves supplying the muscles of mastication and muscles of facial expression?
Each Pharyngeal Arch has its own:
cartilage skeleton
muscular component
sensory nerve supply
motor nerve supply
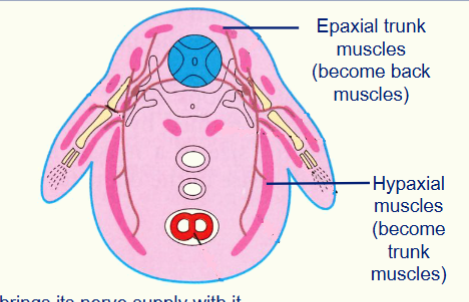
When a muscle migrates it brings its nerve supply with it.
Muscles of mastication are derived from the 1st pharyngeal arch and are therefore innervated by the trigeminal nerve (V)
Muscles of facial expression are derived from the 2nd pharyngeal arch and are therefore innervated by the facial nerve (VII)
This explains why you get a different nerve supply in the head and neck.
What is the sensory nerve supply to the face?
trigeminal nerve
What is the motor nerve supply to the muscles of facial expression?
facial nerve
The Temporomandibular Joint
it is a synovial joint
responsible for allowing movement of the mandible
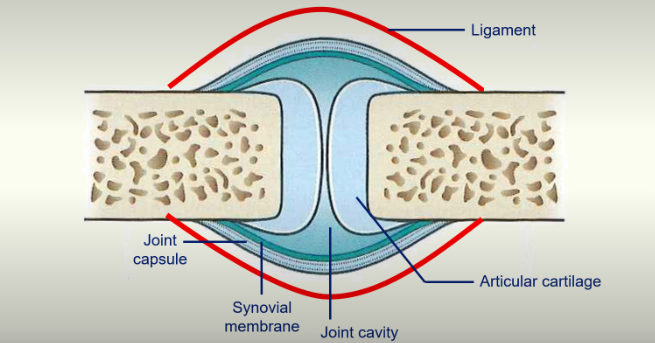
articular cartilage decreases friction
synovial membrane secretes fluid to decrease friction
Movements of the Mandible
depression of the mandible - causes mouth to open
elevation of the mandible - causes the mouth to close
protrusion of the mandible - the lower teeth come to lie in front of the upper teeth
retraction of the mandible - the mandibular head is pulled back into the mandibular fossa
rotation of the mandible - causes lateral chewing movements
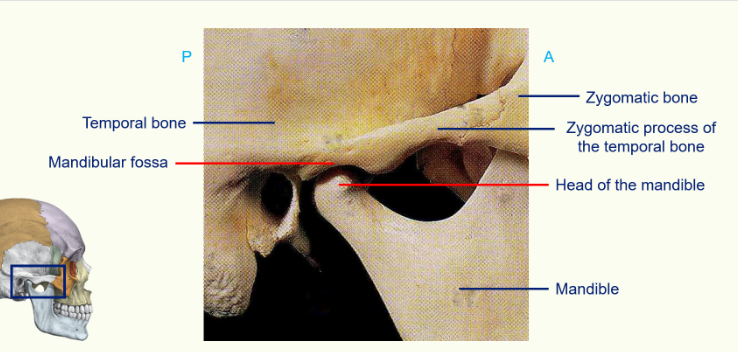
articulation between the temporal bone and zygomatic bone is called the zygomatic process of the temporal bone.
head of the mandible sits in a groove called the mandibular fossa
coronoid process - where the temporalis muscle attaches to.
The Capsule and Ligaments of the Temporomandibular Bone
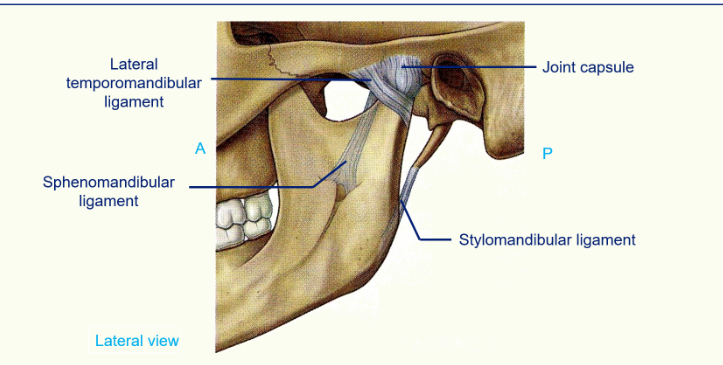
the Lateral temporomandibular ligament prevents retraction of the mandible
the sphenomandibular ligaments and the stylomandibular ligaments secure the joint and makes sure the head of the mandible stays in the mandibular fossa and can rotate without dislocating
The Temporomandibular Joint: articular disc
the reason this joint can have so many movements is due to the articular disc
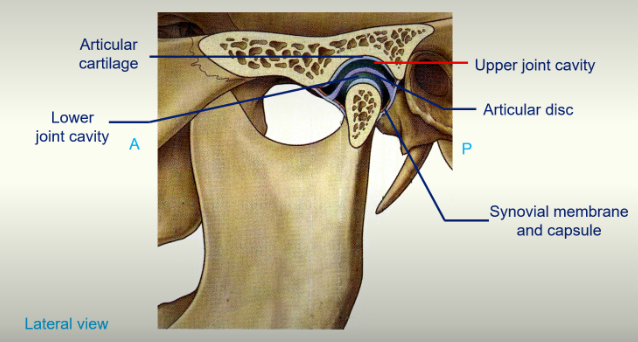
articular cartilage on the head of the mandible
articular cartilage on the mandibular fossa
synovial membrane and capsule can be seen
the articular disc separates the joint cavity into an upper joint cavity and a lower joint cavity and this allows different movements to occur
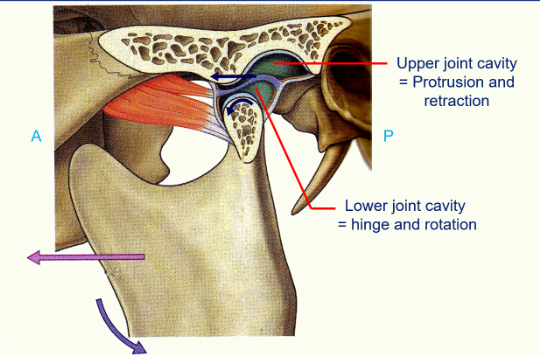
Upper Joint Cavity: the head of the mandible can move out from the mandibular fossa onto the articular tubercule and back again (protrusion and retraction)
Lower Joint Cavity: hinge rotation
The Skull and Vertebral Column Part II
L.O. Differentiate between the atlanto-occipital joint and the atlanto- axial joint and describe the movements that occur at each one.
L.O. Differentiate between different types and shapes of the vertebrae and relate their structure to function.
L.O. Describe the major components of the intervertebral (IV) and how its components reinforce as a cushioning structure between vertebrae.
L.O. Describe the embryology of normal spine development.
L.O. Illustrate and define the ligaments of the vertebral column.
L.O. Describe the surface anatomy of the vertebral column.
The Vertebral Column
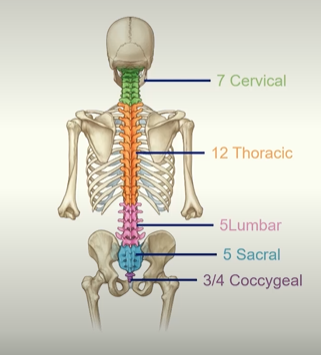
The way to remember the vertebral column:
Breakfast at 7am
Lunch at 12
Dinner at 5pm
and then the Sabral and Coccygeal
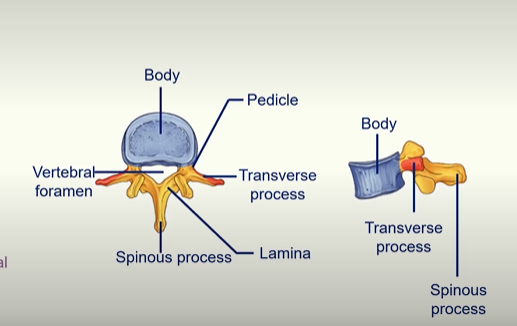
The ‘Body’ is the weight bearing part of the vertebral column. With each segment, the body gets larger because it has to bear more weight. So that’s a way to tell from what region of the body the vertebra is from by the size of the body.
The Vertebral foramen is where the spinal cord is housed.
What is a process?
Outgrowth of tissue from a larger structure, most commonly a bone. These projections serve to provide attachment points for muscles and ligaments or to form joints with other bones.
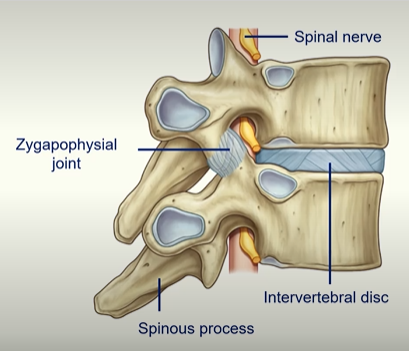
intervertebral disc - secondary cartilaginous joint which allows some movement
zygapophysial joint - synovial joint - get quite a lot of movement
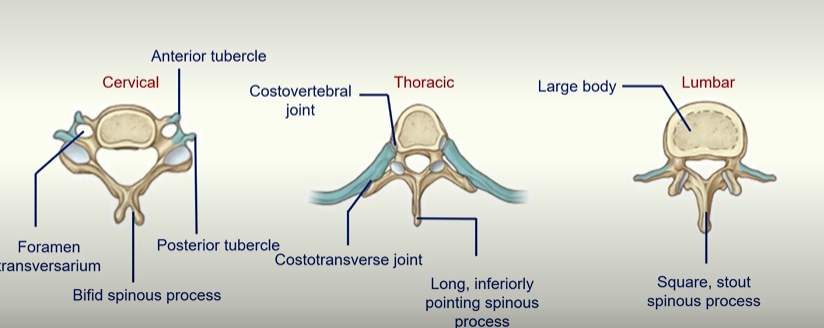
Regional Variations of Vertebrae
Musculoskeletal Block: Upper Limb I - Shoulder to Elbow
L.O. Description of the major landmarks of the bones of the shoulder.
L.O. Description of the relationship between joint structure and range of motion.
L.O. Description of the muscles of the shoulder (in particular the rotator cuff), their associated ligaments and their movements.
Pectoral Girdle and Humerus - ANTERIOR view
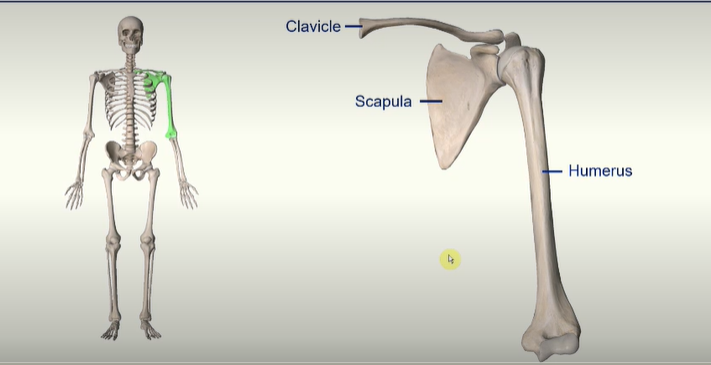
Clavicle -

the clavicle attaches to the sternum on the medial end and the acromion of the scapula at the lateral end
Scapula -
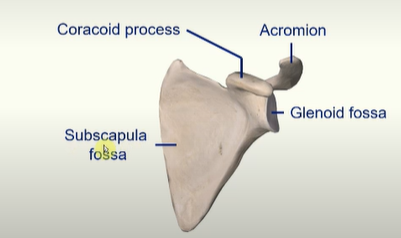
a fossa is just a ‘natural hollow’ in a bone
Glenoid fossa articulates with the head of the humerus
Acromion articulates with clavicle
coracoid process
Humerus -
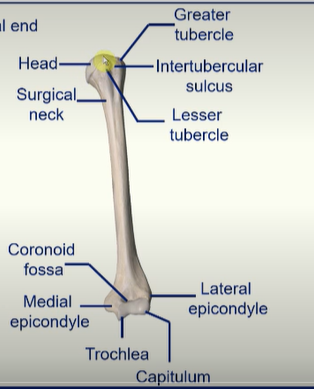
the head articulates with the glenoid fossa
two bumps = greater tubercule
and lesser tubercle
intertubercular sulcus is the groove between the tubercles
surgical neck = most likely to break arm here
trochlea articulates with the ulna
capitulum articulates with the head of the radius
coronoid fossa fits the coronoid process of the ulna
two bumps - medial epicondyle and lateral epicondyle
Pectoral Girdle and Humerus - POSTERIOR view
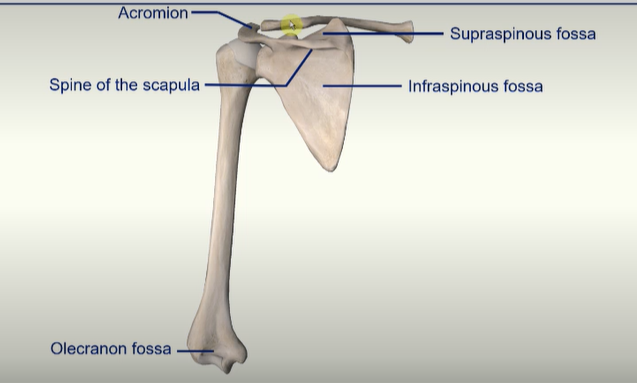
clavicle pushes the humerus away from the rib cage giving it a larger range of motion and stabilising the bone
Spine of the scapula - splits the posterior scapula into two;
Supraspinous fossa
Infraspinous fossa
Pectoral Girdle - Superior View
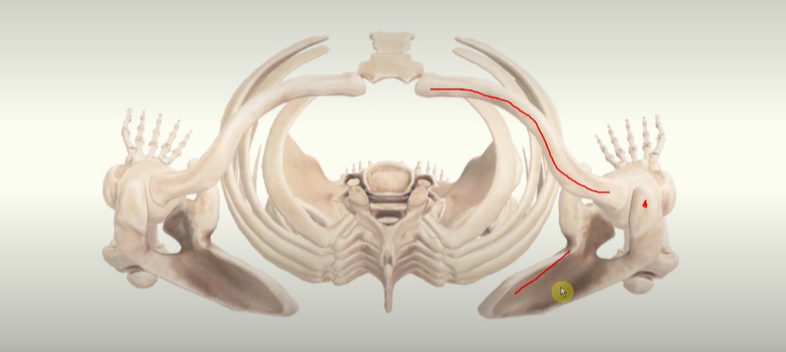
the clavicle becomes quite posterior and is not flat across the body
the scapula is also not flat in the body but positioned at an angle
Synovial Joints -
trade off between stability vs mobility
The Glenohumeral Joint
extremely mobile allowing flexion, extension, abduction, adduction, medial and lateral rotation and circumduction
the disadvantage is the extreme mobility as this joint is the most dislocated joint in the body

Abduction of the arm
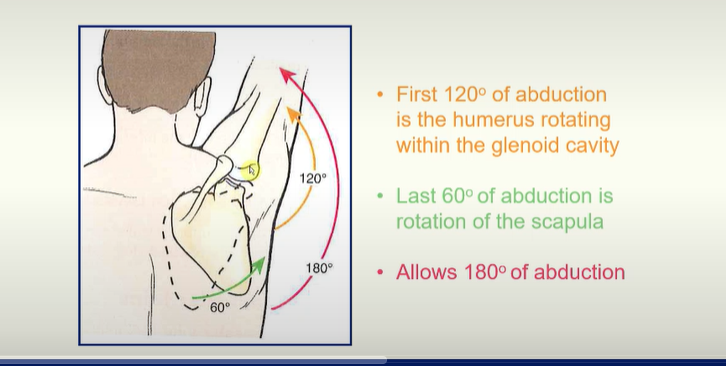
mix of humerus rotating within the glenoid fossa as well as the rotation of the scapula
The Glenohumeral Joint Capsule
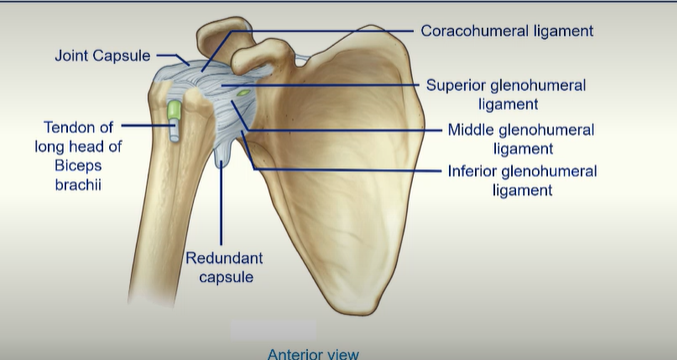
4 Intrinsic Ligaments
Coracohumeral ligament
Superior glenohumeral ligament
Middle glenohumeral ligament
Inferior glenohumeral ligament
redundant capsule hangs at the bottom when the arm is adducted as a bit of slack is needed when that person abducts the humerus as if it was taught the capsule would rip
tendon of long head of biceps of brachii pierces the joint capsule and goes to attach to the very top of the glenoid fossa, actually inside the joint itself. - can rip put
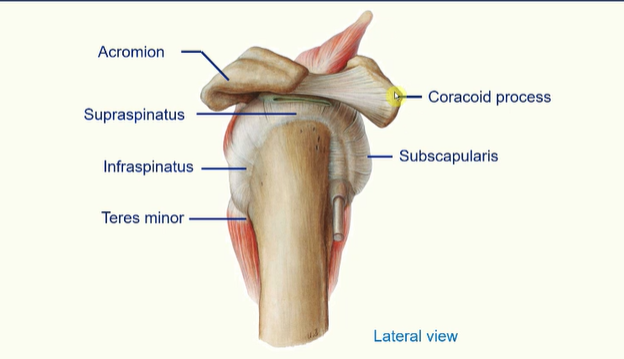
The Rotator Cuff
the rotator cuff is a group of muscles whose tendons surround the glenohumeral joint
as well as providing movement to the upper limb these muscles strengthen the joint
these muscles are;
subscapularis
supraspinatus
infraspinatus
teres minor
Rotator Cuff Muscles
supraspinatus initiates abduction of the arm
infraspinatus allows lateral rotation of the humerus
teres minor allows lateral rotation of the humerus
subscapularis allows medial rotation of the humerus
Rotator Cuff injuries -
common in people who continuously use the arms above the horizontal - throwing, racquet sports, swimming, weightlifting
can lead to inflammation and a result tear in the cuff especially the supraspinatus tendon
can test for injuries by asking a patient to adduct their arm slowly - if the arm suddenly drops to their side at 90 degrees it is likely they have injured their rotator
L.O. Description of the major muscles of each of the compartments and their associated movements.
L.O. Description of the surface anatomy of the arm and shoulder.
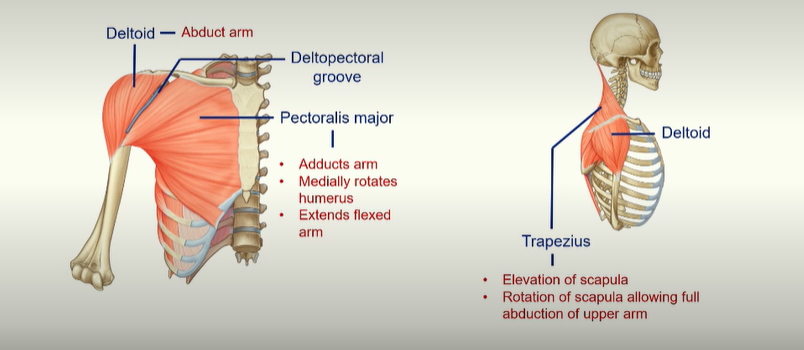
Muscles of the Upper Limb
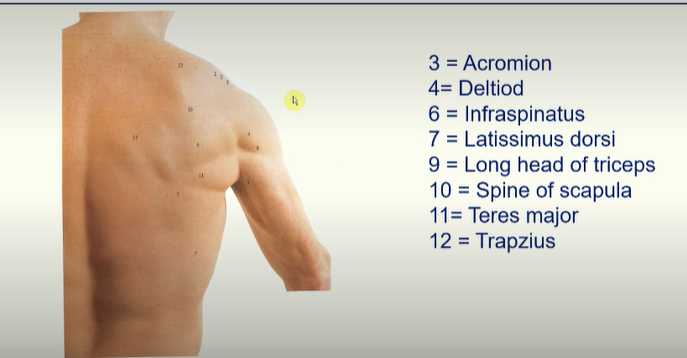
deltoid muscle - allows abduction of arm
pectoralis major - adducts arm, allows medial rotation of the humerus, extends flexed arm.
deltopectoral groove - major vein here
trapezius - allows elevation of the scapular and rotation of scapula allowing full abduction of upper arm.
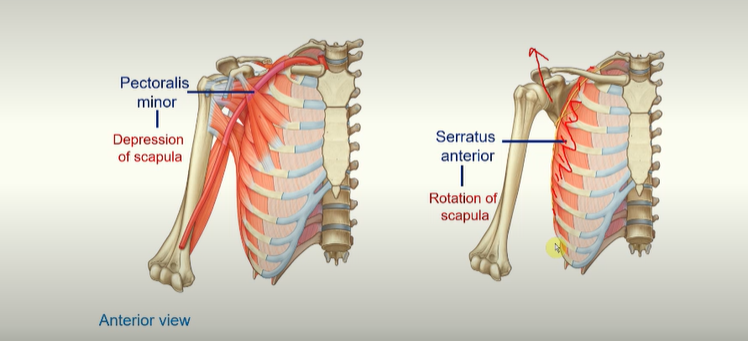
pectoralis minor muscle - allows depression of scapula
serratus anterior - allows rotation of scapula and protraction (moving in) of scapula. This muscle goes around and hugs the rips, goes around between the scapula and the ribs and inserts onto the medial border of the scapula.
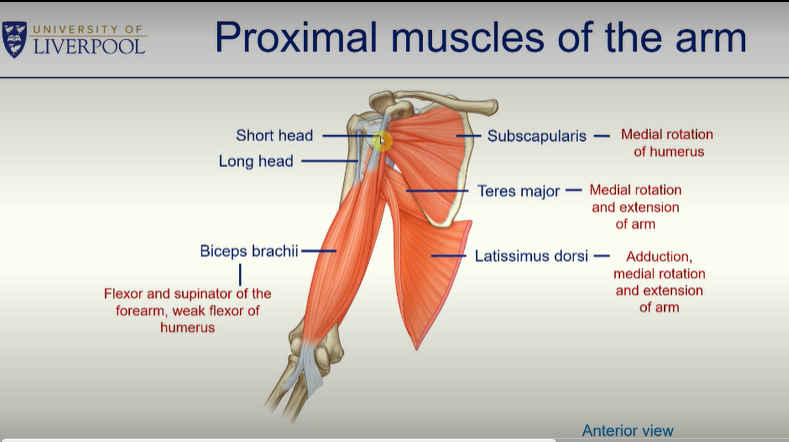
Proximal Muscles of the Arm
teres major - allows medial rotation and extension of arm
latissimus dorsi - allows medial rotation and extension of arm
subscapularis - allows medial rotation of the humerus
biceps brachii - two headed muscle in the arm - allows flexion and supination of the foramen - weak flexor of the the humerus
long head - goes into the glenohumeral joint capsule
short head - inserts into the coracoid process
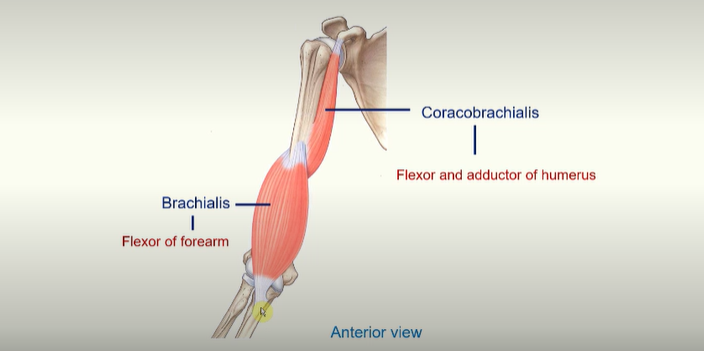
coracobrachialis - flexor and adductor of humerus
brachialis - flexor of forearm
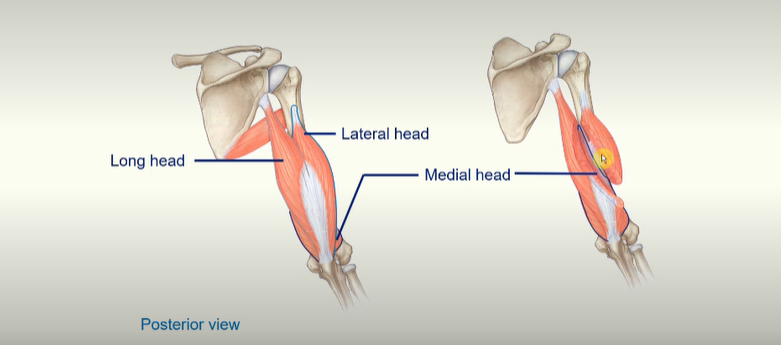
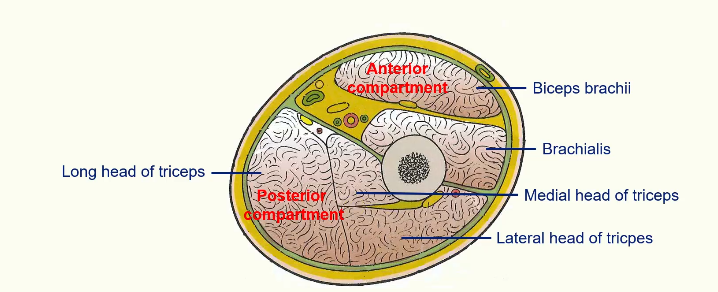
triceps brachii - long head, lateral head and medial head
all of these muscles go to attach to the Olecranon Process of the ulna
all of the muscles help extend the forearm
the long head goes to the lateral part of the scapula - so you do get a little bit of help with the extension of the humerus there.
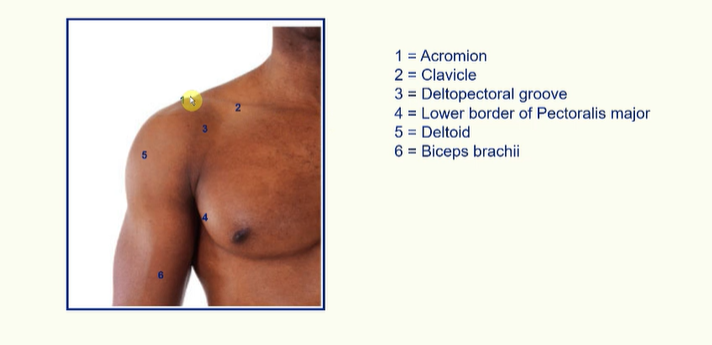
Anterior Surface Anatomy -
Posterior Surface Anatomy -
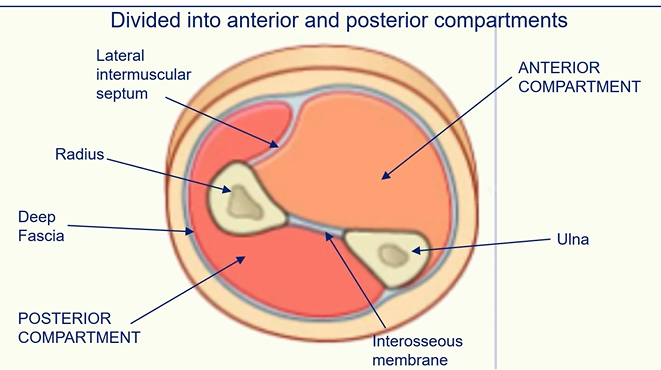
L.O. Description of the compartments of the arm.
L.O. Description of the brachial plexus, its origins and how this relates to the ulnar, median and radial nerves.
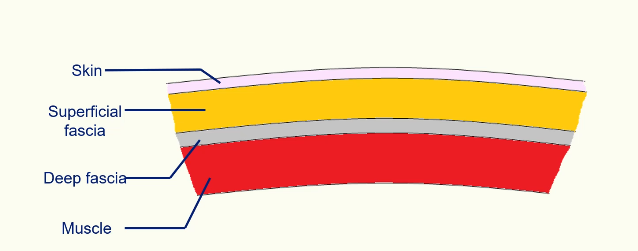
Fascia -
(connective tissue you can see with the naked eye).
Intermuscular Septa -
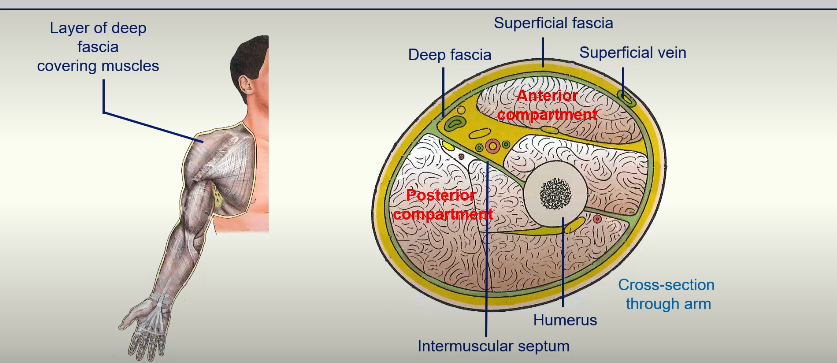
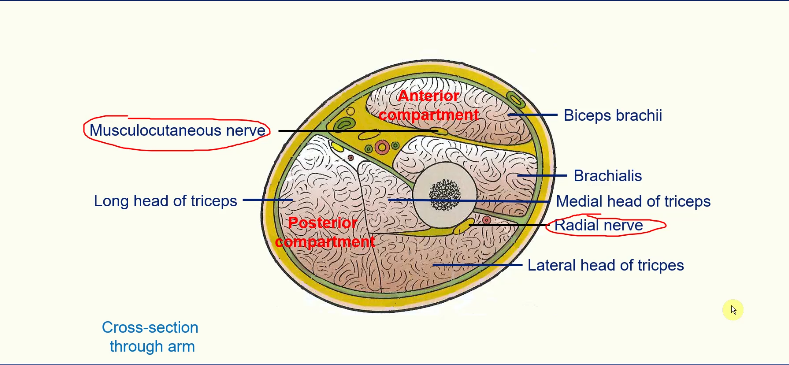
anterior compartment of the arm
posterior compartment of the arm
Compartments of the Arm
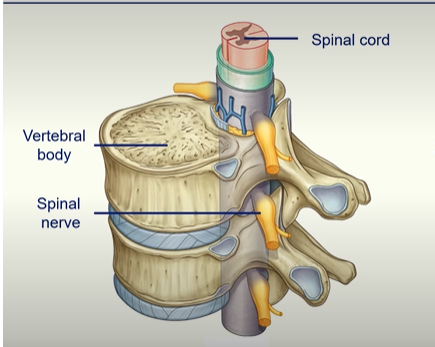
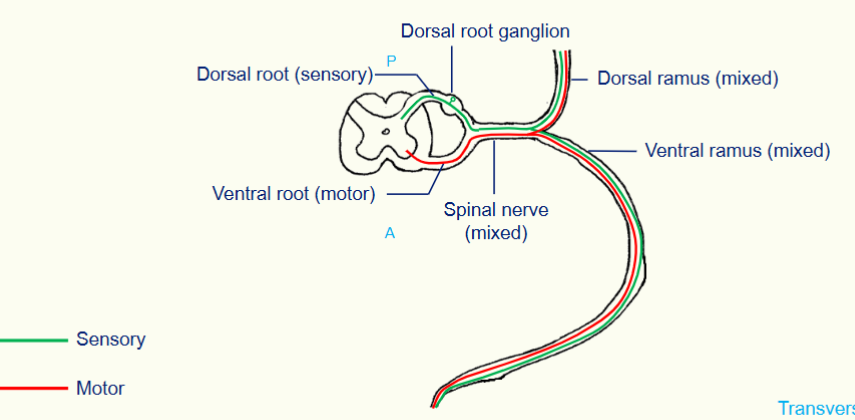
The Spinal Cord
the spinal cord sits inside the vertebral foramen
the spinal nerve is mixed (both sensory and motor)
the spinal nerve splits into two - the dorsal and ventral ramus
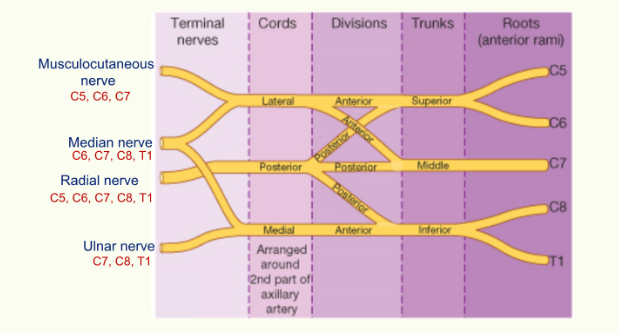
The Brachial Plexus (nerves which supply the arm)
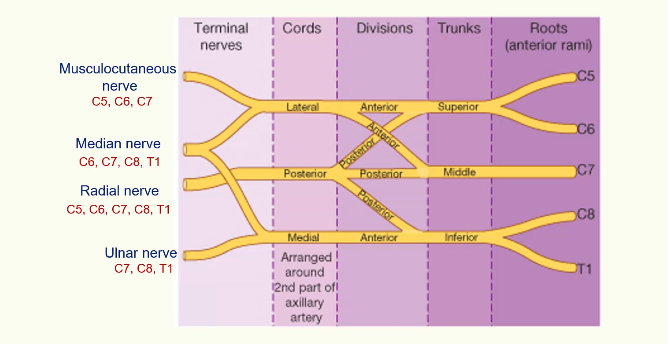
the Roots - C5, C6, C7, C8 and T1
C5 and C6 join to become the Superior Trunk
C7 becomes the Middle Trunk
C8 and T1 join to become the Inferior Trunk
Then each trunk gives off a posterior and anterior division
The posterior divisions all join together to form a posterior cord
The middle trunk gives off an anterior division which joins from the superior trunk to form a lateral cord. And the inferior trunk just keeps going to the anterior division to form the medial cord.
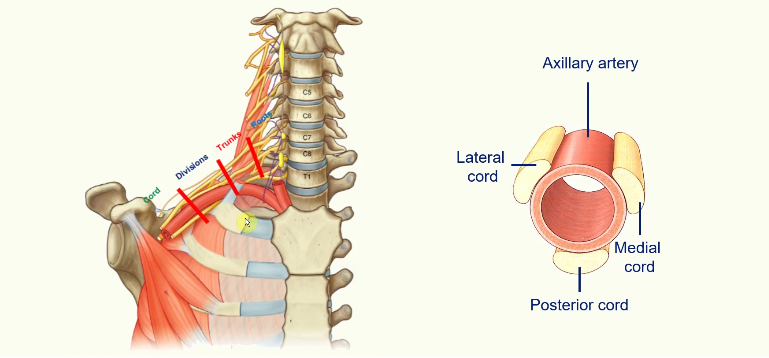
Cord position compared to Artery:
The lateral cord is lateral to the artery
the posterior cord is posterior to the artery
the medial cord is medial to the artery
The posterior cord just keeps going and becomes the Radial Nerve
The medial and lateral cord will split and join together to form the median nerve
The lateral cord continues as the muscular cutaneous nerve
The medial nerve continues as the ulnar nerve
Motor Innervation of the Upper Arm
Musculocutaneous Nerve - supplies the anterior compartment;
biceps brachii
coracobrachialis
brachialis
Radial nerve supplies the posterior compartment
1. triceps brachii
Upper Limb 2: Elbow to Hand
L.O. Recall the major landmarks of the humerus, radius and ulna including the ligaments (e.g. annular ligament).
L.O. Demonstrate the structure and movements of the elbow joint.
Bones of the Upper Limb
Arm Proper
contains the humerus
Forearm
contains the radius and ulna
Hand
contains 8 carpal bones in the hand, 5 metacarpals in the palm and 14 phalanges in the digits
Proximal Humerus
greater tubercle
lesser tubercle
head of humerus
Distal Humerus - Anterior View
lateral epicondyle
medial epicondyle
capitulum
trochlea
coronoid fossa
radial fossa
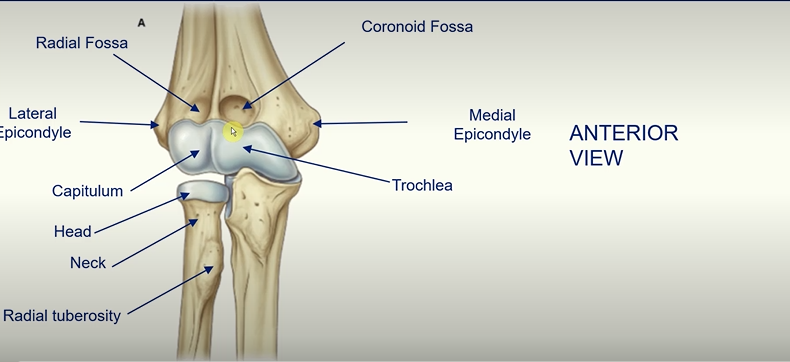
at the superior end the radius is much smaller than the ulna
at the inferior end the radius is much bigger than the ulna
the radius articulates with the capitalism
the ulna articulates with the trochlea
head and neck of the radial as well as the radial tuberosity
Proximal Ulna
trochlear notch (where ulna articulates with the trochlear of the humerus)
coronoid process - ‘beak like’ projection
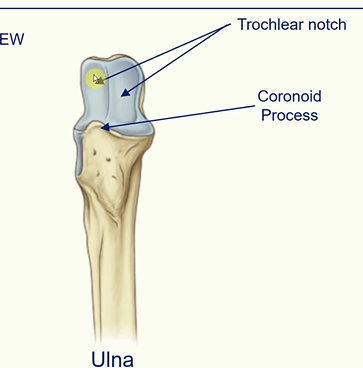
radial notch - where the head of the radius sits on the ulna
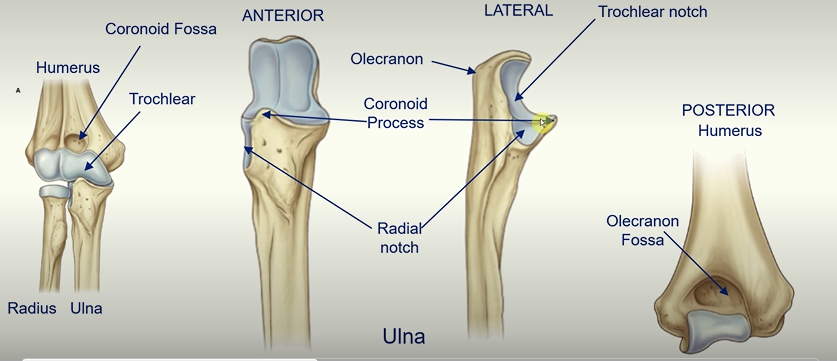
olecranon fossa - see it posteriorly on the humerus - big indentation where the olecranon sits when elbow is fully extended
the olecranon is the bony point of the elbow at the top of the ulna bone
Elbow Joint
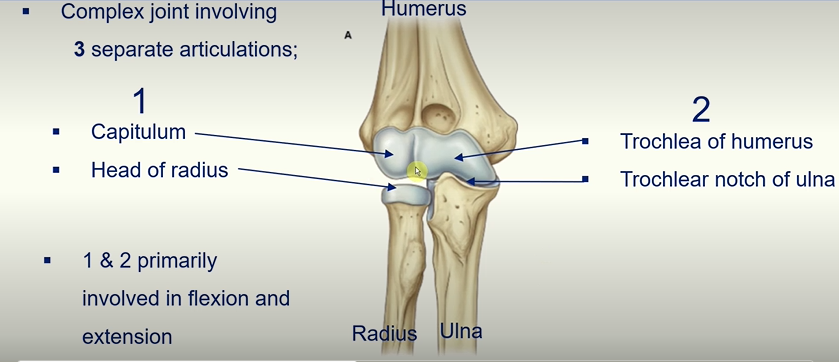
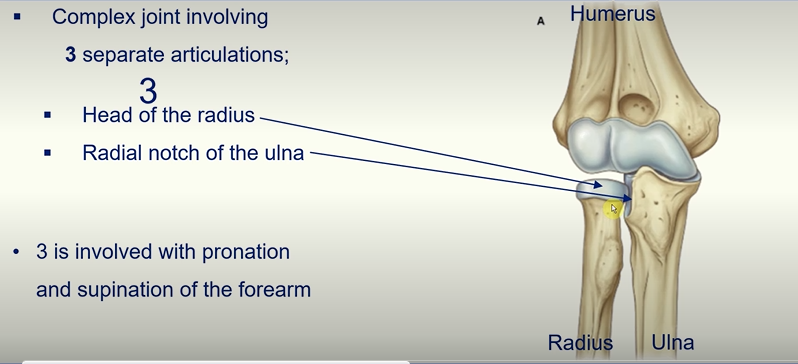
3 separate Articulations make up the elbow joint!
The capitulum and head of radius - allows flexion and extension
Trochlea of humerus and trochlea notch of ulna - allows flexion and extension
Head of radius and radial notch of the ulna - involved in pronation and supination of the forearm.
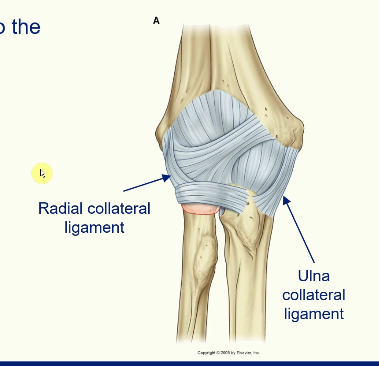
Stability of the Elbow Joint
fibrous membrane of the joint contributes to the stability
thickened medially and laterally to form the collateral ligaments
support flexion and extension movement
Taking the ligaments away you can see…
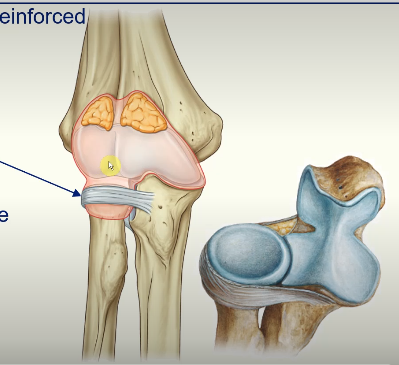
external surface of the joint capsule reinforced laterally
cuffs the head of the radius
annular ligament of radius
allows the head of the radius to slide against the radial notch of the ulna and pivot on the capitulum during pronation and supination
At the Distal End…
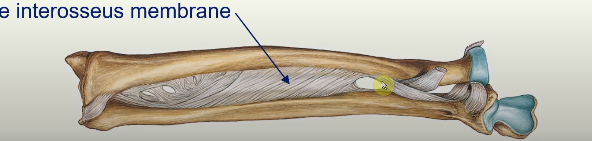
distally the ulnar notch of the radius slides anteriorly over the convex surface of the head of the ulna
bones held together during this movement by
the articular disc at the distal radio-ulnar joint
the interosseus membrane
Muscles of Pronation and Supination
Pronation = inward rotation of the forearm
Supination = outward rotation of the forearm
Two muscles supinate the hand
biceps brachii
supinator
Two muscles pronate the hand
pronator teres
pronator quadratus
Pronation
Pronator teres
Origin: medial epicondyle of the humerus
Insertion: lateral surface of the radius midway along shaft
Pronator quadratus
Origin: anterior surface of the distal end of the ulna
Insertion: anterior surface of the distal end of the radius
Action of movement
as muscles contract the distal end of the radius is pulled over the ulna
this causes tendon of biceps brachii muscle and the supinator muscle to become wrapped around the proximal end of the radius
when these muscles contract they unwrap from the bone, producing supination.
L.O. Describe the bones of the wrist/hands with particular attention to carpal bones and the carpal tunnel.
L.O. Classify the muscles of the forearm and their associated movements on the wrist and the hand.
Bones of the Upper Limb - The Hand
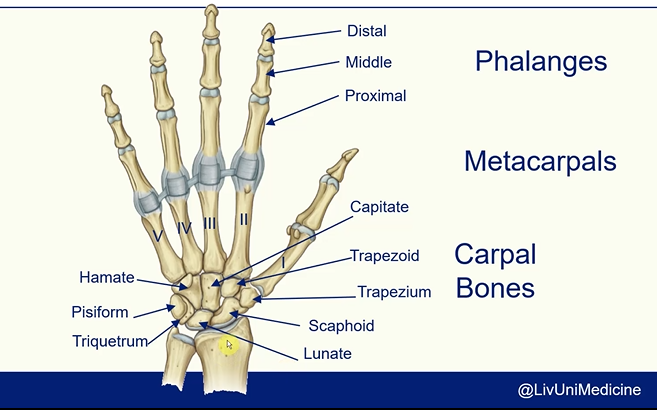
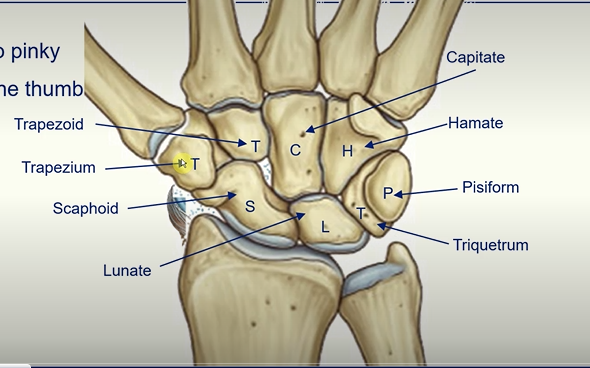
Carpal Bones -
Straight Line To Pinky
Here Comes The Thumb
Scaphoid
Lunate
Triquetrum
Pisiform
Hamate
Trapezoid
Capitate
Trapezium
The Anatomical Snuffbox
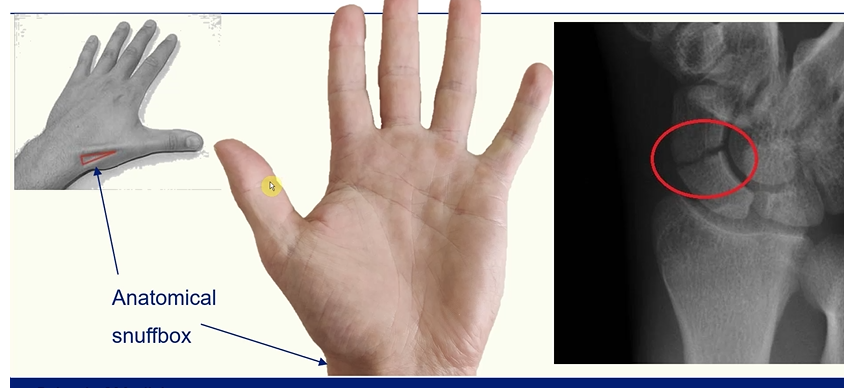
this region is highly palpated in order to see if the scaphoid bone is broken
the scaphoid bone has a good blood supply so if this is interrupted complications can occur
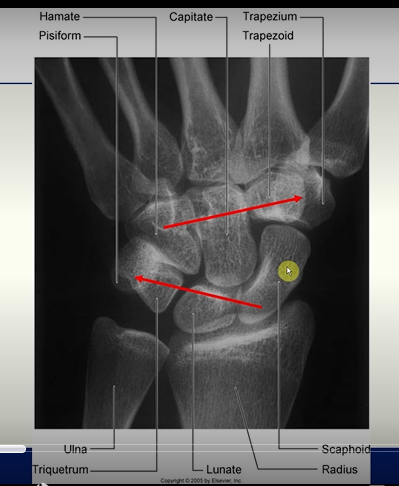
X - RAY
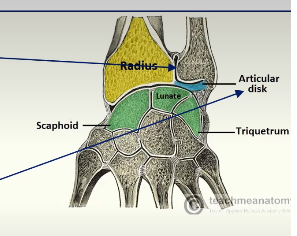
Wrist Joint
Articulation between;
the distal end of the radius and the articular disc overlying the distal end of the ulna
ellipsoid concave
scaphoid and lunate
ellipsoid convex
Radius
the scaphoid and the lunate articulate with the radius
sometimes a small part of the triquetrum may articulate with the articular disc of the distal radio-ulnar joint, but not directly with the radius itself
Ulna
the ulna does not directly articulate with any carpal bone.
instead, the triangular fibrocartilage complex (TFCC) sits between the ulna and the proximal carpal row (mainly the triquetrum and lunate)
Meta Carpals
I, II, III, IV, V (from thumb to pinky finger)
Muscles of the Forearm
muscles in the anterior compartment help flex the wrist joint and fingers
muscles in the posterior compartment help extend the fingers and wrist joint
Anterior (flexor) Compartment
Muscles in this compartment;
move the wrist joint
flex the fingers and thumb
pronate the hand
Arranged in three layers
superficial
intermediate
deep
Deep Layer
Made of three muscles
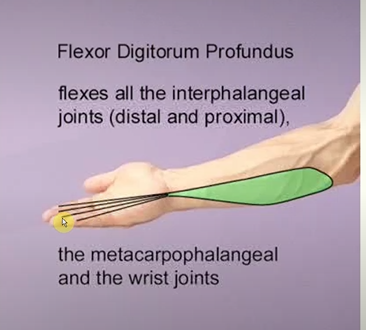
Flexor digitorum profundus
Action;
flex the metacarpophalangeal joints (knuckles)
flexes the proximal and distal interphalangeal joints of four finger
flexes the wrist
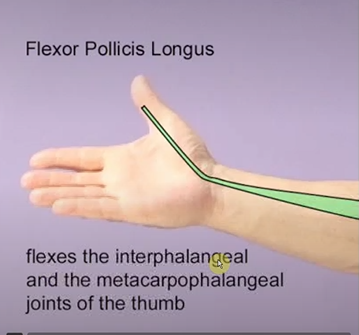
Flexor pollicis longus
Action; flexes the thumb
Pronator quadratus
Action; pronating the forearm
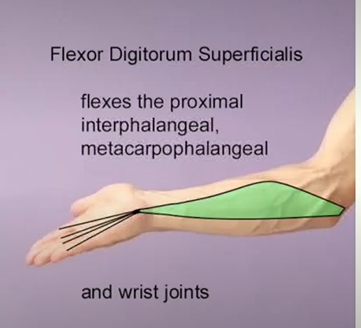
Intermediate Layer
Flexor digitorum superficialis muscle
Action;
flexes metacarpophalangeal joint
flexes the proximal interphalangeal joint of four fingers
flexes the wrist
The Carpal Tunnel
tendons of flexor digitorum profundus, flexor digitorum superficialis and flexor pollicis longus pass through carpal tunnel
formed by the carpal bones and flexor retinaculum (prevents bowing of tendons)
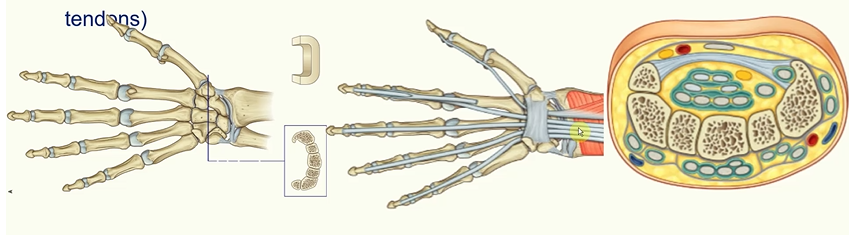
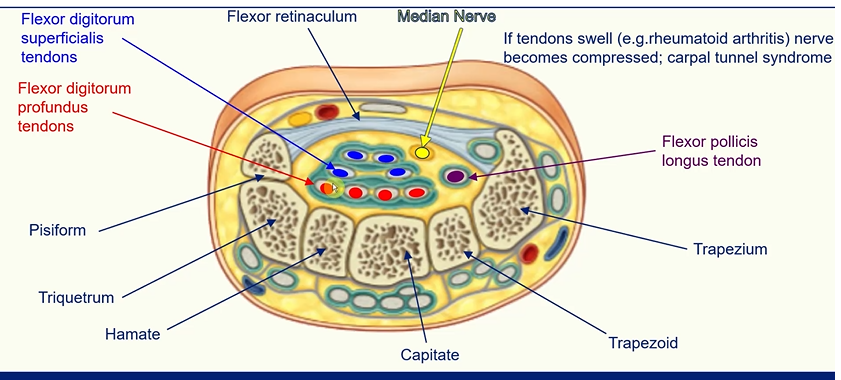
median nerve innervates this area
compression of this nerve causes rheumatoid arthritis or carpal tunnel syndrome
Carpal Tunnel Syndrome
increased pressure in the carpal tunnel
pins and needles and pain in distribution of median nerve
weakness and loss of muscle bulk of thenar muscles
Treatment;
reducing inflammation (rest/splint/steroids)
surgical decompression of the flexor retinaculum
Superficial Layer
Four muscles all with a common origin on the medial epicondyle of the humerus
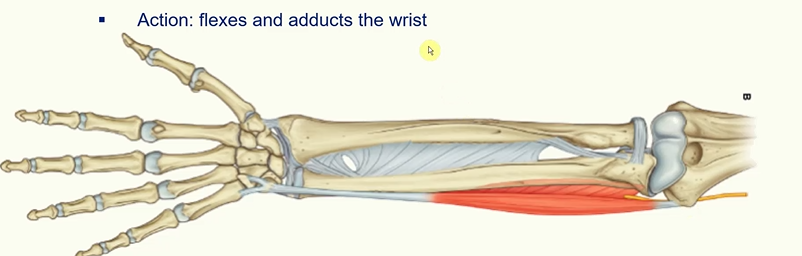
Flexor carpi ulnaris
Action - flexes and adducts the wrist
Palmaris Longus
Absent in ~15% of the population
Action; flexes the wrist
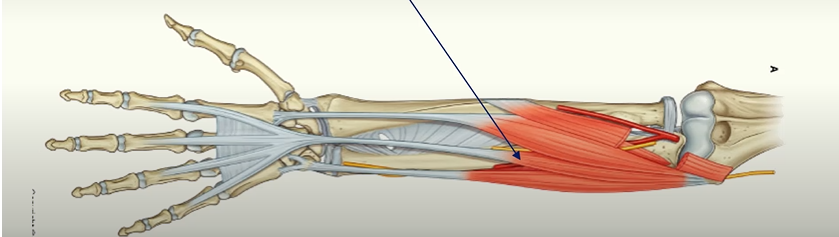
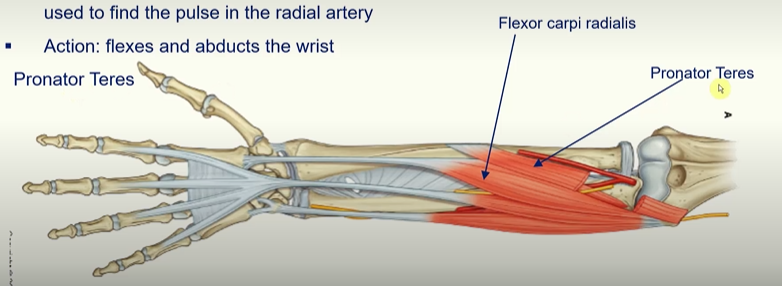
Flexor carpi radialis
tendon is easily palpated in the wrist and is usually used to find the pule in the radial artery
action; flexes and abducts the wrist
Pronator Teres
rotates radius on its axis
L.O. Classify the muscles of the forearm and their associated movements on the wrist and hand.
L.O. Illustrate the vascular supply of the upper limb.
L.O. Discuss the innervation of the hand.
L.O. Describe the contents and the boundaries of the cubital fossa (brachial artery, cubital vein and median nerve and their relationship to each other).
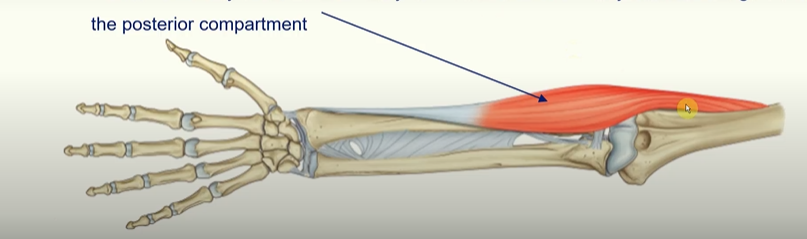
Extensor Compartment (Posterior view of the forearm)

Muscles in this compartment;
move the wrist joint
extend the fingers and thumb
supinate the hand
Arranged into two layers
superficial
deep
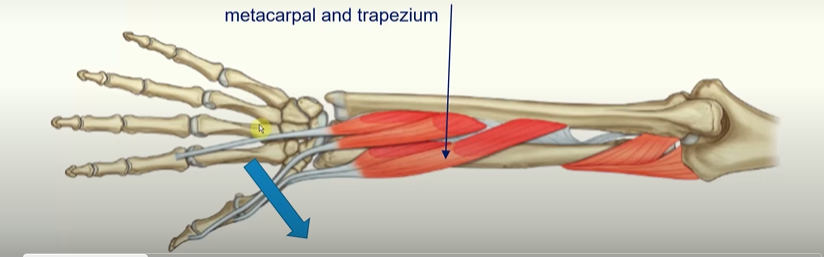
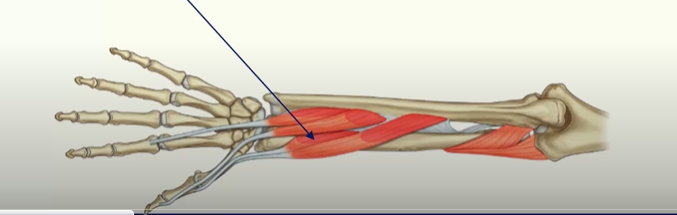
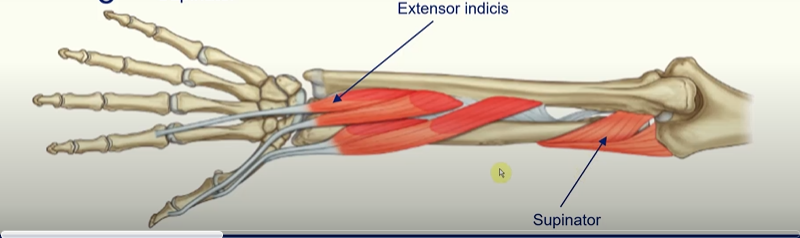
The Deep Layer
there are 5 muscles in the deep layer of the posterior forearm
Abductor pollicis longus; abduct the thumb at joint between metacarpal and trapezium.
Extensor pollicis brevis
tendon forms the lateral border of the anatomical snuff box
action; extends the metacarpopharangeal and carpometacarpal joints of the thumb
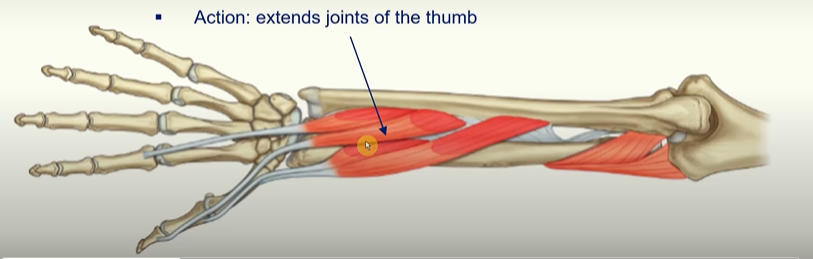
Extensor pollicis longus
tendon forms the medial border of the anatomical snuffbox
action: extends joints of the thumb
Extensor Indicis
action: accessory extensor of the index finger
Supinator
it is wrapped around the radius, once it contracts it will try to unravel itself and cause supination
The Superficial Layer of the Posterior Forearm
seven muscles
all originate from the supraepicondylar ridge and lateral epicondyle of the humerus
Brachioradialis
Action; accessory flexor of the elbow joint as it is anterior to that joint even though it is in the posterior compartment
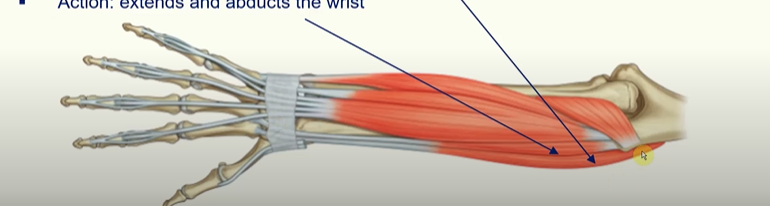
Extensor carpi radialis longus
Action: extends and abducts the wrist
Extensor carpi radialis brevis
Action: extends and abducts the wrist
Extensor digitorum
Action: major extensor of the four fingers
Extensor digiti minimi
Action: accessory extensor of the little finger
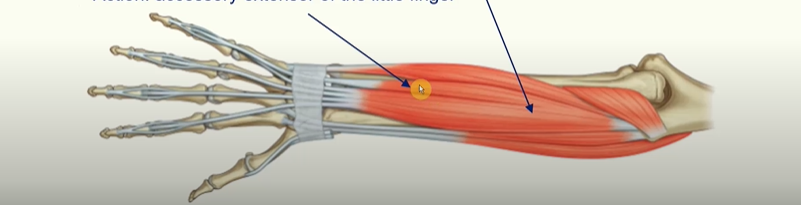
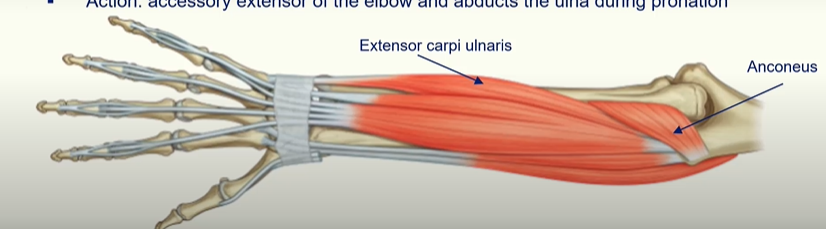
Extensor carpi ulnaris
Action: extends and adducts the wrist
Anconeus
Action: accessory extensor of the elbow and abducts the ulna during pronation.
Arteries of the Upper Limb
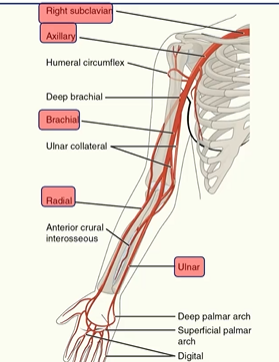
right subclaviar artery
axillary artery
brachial artery
radial artery
ulnar artery
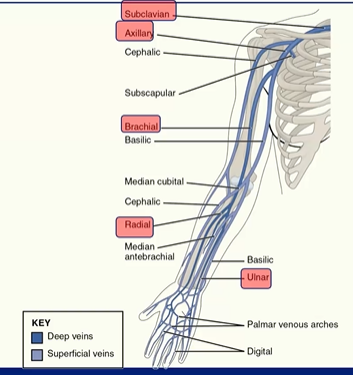
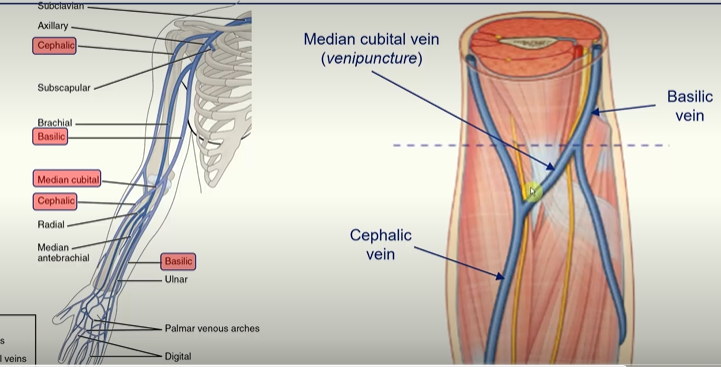
subclavian veins
axillary veins
brachial veins
radial veins
ulnar veins
Innervation of the Hand
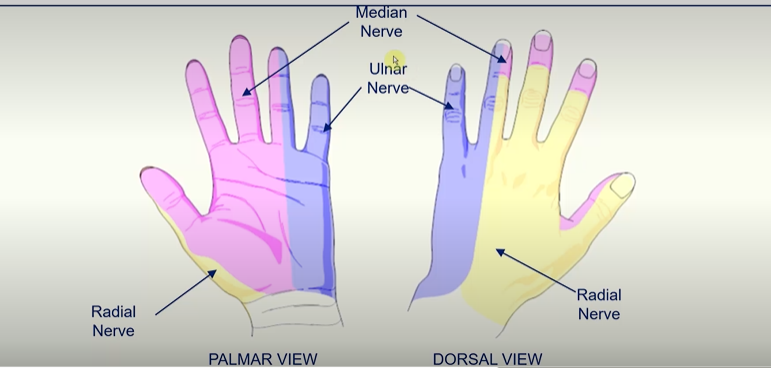
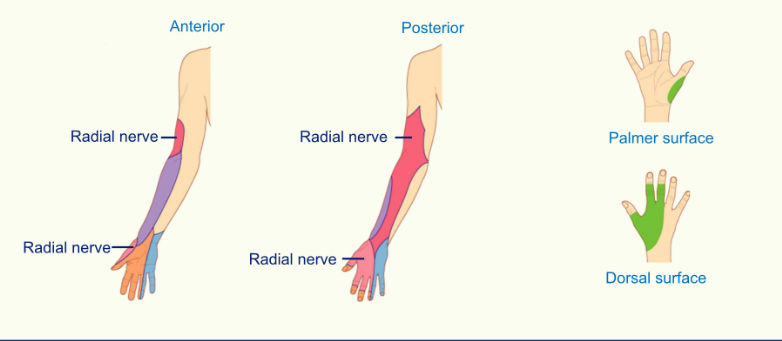
radial nerve innervates thumb and side of the thumb, first finger, middle finger and half of the ring finger on the dorsal view
median nerve innervates the thumb, index finger, middle finger and half of the ring finger in the palmar view
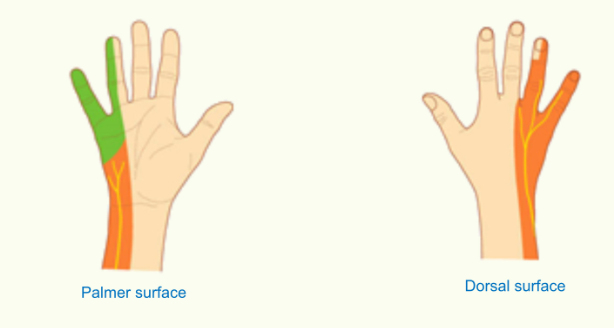
the ulnar nerve innervates the pinky finger and half the ring finger on both sides of the hand
Cubital Fossa
important transition area between the arm and forearm
formed by:
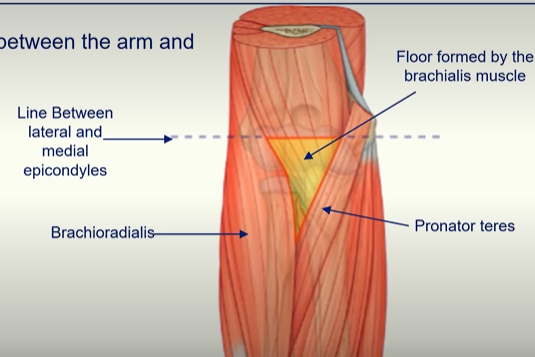
line between the epicondyles forms a ridge
when taking blood pressure readings, the clinician places the stethoscope over the brachial artery in the cubital fossa
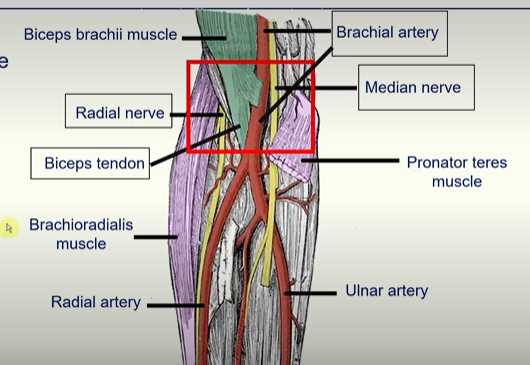
A way to remember is:
Really need (radial nerve)
Beer to (biceps tendon)
Be at (brachial artery)
My nicest (median nerve)
Cubital Fossa - Roof
MSK: Cartilage of the Joint
L.O. Describe the different types of cartilage.
L.O. Describe fibrocartilage, its function and location.
L.O. Describe hyaline cartilage, its function and location.
L.O. Describe the components of cartilage and their functions.
L.O. Describe the process of wear, lubrication and lambda ratio.
Cartilage composition and function
The Skeletal System and Cartilage
Skeletal tissues are examples of specialised connective tissues (one of the four basic tissue types).
the skeletal system is mainly comprised of bone which forms a framework for the rest of the body tissues.
adult skeleton also includes cartilage
Cartilage
is more elastic than bone
forms a semi-rigid part of the skeleton (a firm yet resilient gel)
forms a protective layer at many joints surfaces
What is cartilage?
cartilage is a specialised form of connective tissue that consists of cells embedded in extracellular matrix (ECM)
one cell type = chondrocyte (means cartilage cell_
few cells and a large amount of ECM
the ECM gives cartilage its unique characteristics
Other important points, Cartilage is….
avascular: cartilage does not contain blood supply
aneural: cartilage does not have a nerve supply
cartilage has no lymphatic supply - so in order to get nutrients and get rid of waste, it relies on diffusion.
chondrocytes maintain their phenotype to retain their function in permanent cartilage.
limited capacity for regeneration and repair in response to injury or disease
Cartilage Function
Functions:
structural support for soft tissues
connects bones together
sliding area for joints
growth in long bone length
embryonic skeleton
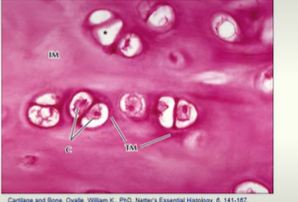
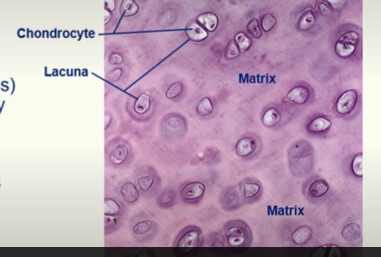
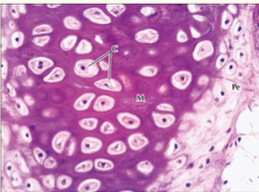
Chondrocytes
they are mature cartilage cells
they are located in spaces called lacunae
the matrix surrounds the lacunae
they are derived from chondroblasts (immature chondrocytes) that become trapped in extracellular matrix that they secreted
chondrocytes rely on diffusion for oxygen, nutrients and waste removal
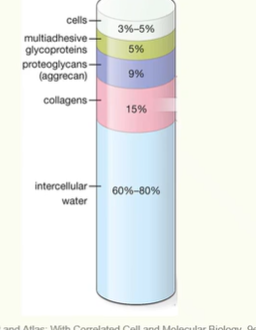
Composition of Cartilage Matrix
Cartilage is hydrated: 70-75% of its wet weight is water.
Rest of the matrix is composed of structural macromolecules.
Collagen typically makes up 15-20% of cartilage.
typically type II collagen
forms a fibrillar network
provides tensile strength
Proteoglycans make up about 2-10% of cartilage.
also has non-collagenous proteins as well
Some Cartilage has a Perichondrium - fibrous outer lining of cartilage which also has an inner cellular layer
What are Proteoglycans?
a protein
Structure
core protein
GAG chains (covalently bound)
‘GAG chains - glycosaminoglycan (long unbranched polysaccharide chains of repeating disaccharide units)’
Characteristics of Proteoglycans
negatively charged
attract Na+ ions
osmotic effect, attracts water
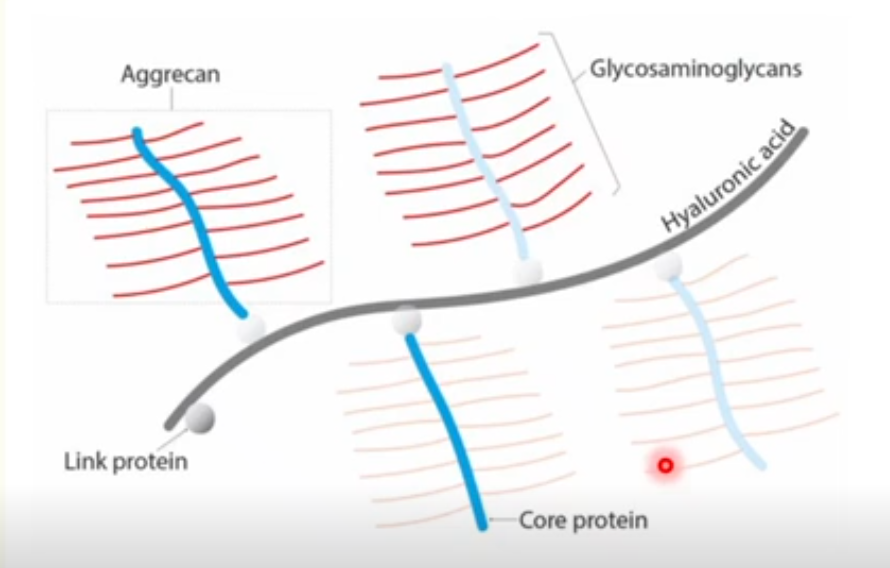
Major Proteoglycan of cartilage = aggrecan
Aggrecan in cartilage
Aggrecan is the major proteoglycan of cartilage
it contains GAGs that are sulfated, mainly chondroitin sulfate and keratan sulfate
Cartilage also contains hyaluronic acid (HA)
this is a non-sulfated GAG
HA can bind to the aggrecan core protein via a link protein
forms large aggrecan aggregates
Summary
interactions of aggrecans, water and collagen fibrils gives cartilage its resistance to compression (stiffness) and resilience.
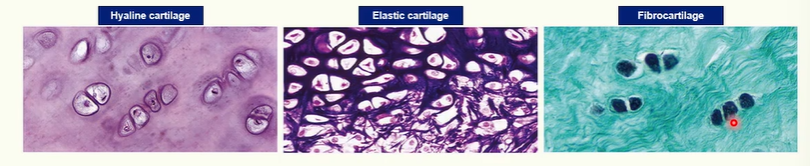
Cartilage Types
Three types of cartilage, defined by their histological appearance and ECM:
hyaline
fibrocartilage
elastic
Hyaline
most common cartilage in the body
you can find it in synovial joints, respiratory passages, costal cartilages and foetal skeleton
Fibrocartilage
find it in very specific places
pubic symphysis, intervertebral discs, menisci, articular discs (TMJ and sternoclavicular), entheses (ligament and tendon attachments to bone)
Elastic cartilage
You find it in….
pinna of ear
external auditory meatus
auditory tube
epiglottis
Histology of Cartilage
Function of hyaline cartilage
resists compression
provides cushioning, smooth, and low-friction surface for joints
provides structural support in respiratory system
forms foundation for development of fetal skeleton and further endochondral bone formation and growth
the perichondrium is present on nearly all types of hyaline cartilage except at the articular surface and in a growth plate (epiphyseal plates)
Perichondrium - fibrous outer lining of cartilage which also has an inner cellular layer
Function of elastic cartilage
provides flexible support for soft tissues
has a perichondrium
Function of Fibrocartilage
resists deformation under stress
does not have a perichondrium
All three of these tissues have chondrocytes and chondroblasts
Characteristics of Extra cellular matrix
Hyaline cartilage ECM
contains only Type II collagen fibrils
aggrecan monomers
Elastic cartilage ECM
contains only Type II collagen fibrils
elastic fibres
aggrecan monomers
Fibrocartilage ECM
Type I and II collagen fibres
proteoglycan monomers: aggrecan (secreted by chondrocytes) and versican (secreted by fibroblasts)
Growth and repair of cartilage is very limited.
cartilage can try to repair, but it commonly forms scar tissue composed of fibrocartilage which does not have the right mechanical properties
The appearance of Hyaline cartilage
hyaline means glossy
hyaline cartilage has a translucent, glassy appearance
it is the most common type of cartilage
The appearance of Elastic cartilage
lots of elastic fibres, that are rich in the protein elastin
elastic cartilage is more flexible
when bent, it will bounce back to its original form
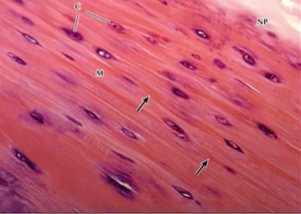
The appearance of Fibrocartilage
durable and tough due to presence of more type I collagen fibres
a mixture of hyaline cartilage (collagen type II) and dense fibrous connective tissue (collagen type I)
resists compression, absorbs shock, and prevents damage
found in sites subjected to high tensile and compressive forces.
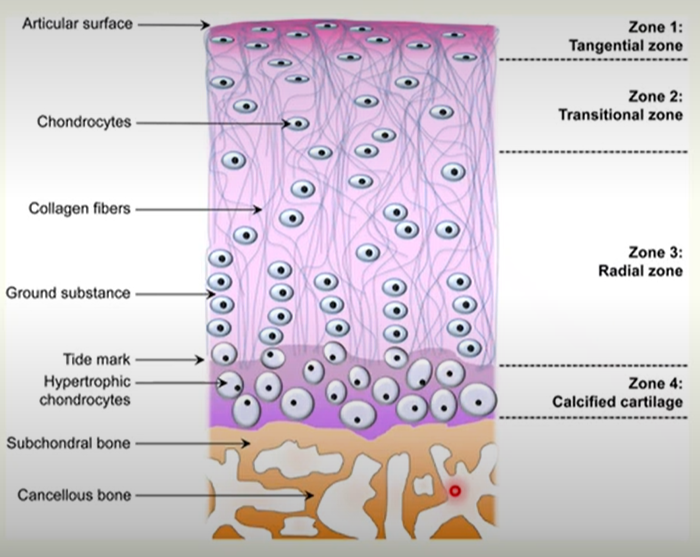
What is articular cartilage?
it is hyaline cartilage that covers the ends of bones involved in a joint (i.e. articular surface of synovial joints)
articular cartilage is remnant of the original hyaline cartilage template of developing bones, that persists through life.
articular cartilage is divided into four zones
articular cartilage is in contact with subchondral bone
The Four Zones of Cartilage
Zone 1: Superficial or tangential) zone
elongated and flattened chondrocytes
collagen is parallel to the articular surface
Zone 2: Transitional/middle zone
rounder chondrocytes distributed randomly in the matrix
collagen fibrils are less organised and oblique to the surface
Zone 3: deep (radial ) zone
small, round chondrocytes arranged in columns
collagen fibrils are perpendicular to cartilage surface
Zone 4: Calcified Zone
large, hypertrophic chondrocytes
collagen is perpendicular to the cartilage surface
Articular cartilage resists mechanical load
the negatively charged GAG sidechains of aggrecan repel each other and attract water
this increases matrix volume
expansion of the matrix is limited by the collagen network (tensile strength)
Cartilage Loading
compression pushes GAG side chains closer together and releases water, decreasing the matrix volume
decompression (unloading) allows re-expansion of the molecules and matrix volume
Synovial membrane and fluid
articular surfaces are in contact with each other at a synovial joint (or have an intervening disc)
must be lubricated to lower friction and allow wide range of movement
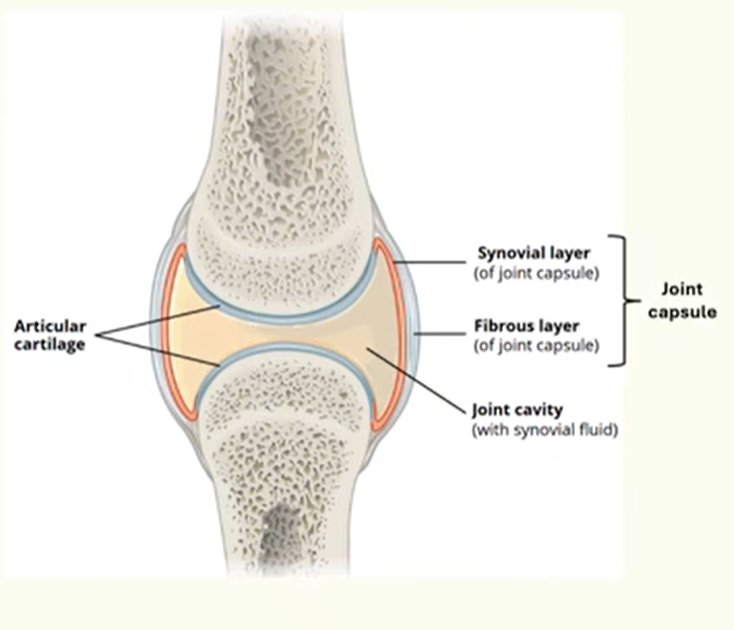
All synovial joints have a joint capsule and synovial cavity:
outer fibrous membrane
inner synovial membrane
encloses the synovial cavity which is filled with synovial fluid
Synovial membrane function
Specialised connective tissue
not epithelial! Lacks a basement membrane
2 main layers:
Intimal lining cells = synoviocytes (Type A = immune cells such as macrophages, type B = fibroblasts)
Subintimal matrix = loose connective tissue that is highly vascularised
Functions:
to produce synovial fluid
to remove cellular and connective tissue debris
nutrition
Synovial Fluid
Synovial fluid is an ultrafiltrate of blood plasma.
less protein, but similar electrolyte concentrations
Hyaluronic Acid
non-sulfated GAG secreted by synoviocytes
gives the synovial fluid its high viscosity
also helps to maintain the thickness of the lubricating fluid film
Lubricin
proteoglycan secreted by both superficial cartilage cells and synovium
lubricates the surface of the cartilage
stick to the articular cartilage, projecting a highly negatively charged domain that repel each other, preventing the surfaces from touching
Phospholipids are also bound to the articular surface, providing hydrophobicity (repel each other).
When two articular surfaces come into contact they try and repel each other.
Wear, lubrication and lambda ratio
Wear = the gradual breakdown or erosion of the smooth cartilage
Synovial joints are subjected to an enormous range of loading conditions
Yet under normal circumstances, the cartilage sustains little wear.
How?
A number of lubrication mechanisms to aid articulation.
Fluid film lubrication
a thin fluid film separates the articular surfaces
load is supported by the increased hydrostatic pressure that develops in the fluid when it is compressed
The three types of fluid film lubrication
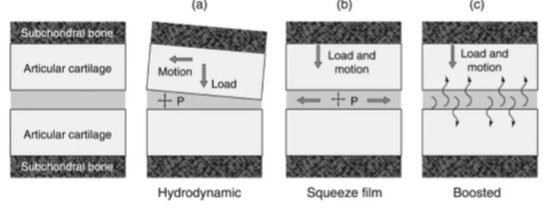
a) Hydrodynamic fluid film lubrication; where fluid gets trapped and pressurised within the space, due to perhaps the cartilage becoming deformed as it is depressed, changes shape, trapping some fluid and increasing the pressure in the fluid. This forms a lifting pressure again.
b) Squeeze film; surfaces move towards each other, squeezing fluid and generating pressure
c) boosted; when the joint is loaded, water is forced into the cartilage rather than the synovial fluid —> this increases the concentration of the hyaluronic acid in the synovial fluid, increasing the viscosity and this helps bear load.
Summary:
Joints use all three of these lubrication mechanisms depending on the load/movement.
—> Fluid film lubrication is the most ideal type of lubrication that we would like to see when we’re loading our joints, however it is not always possible when you are…
bearing heavy and prolonged loads
geometry incongruence
or have low synovial of fluid viscosity
Then boundary lubrication occurs
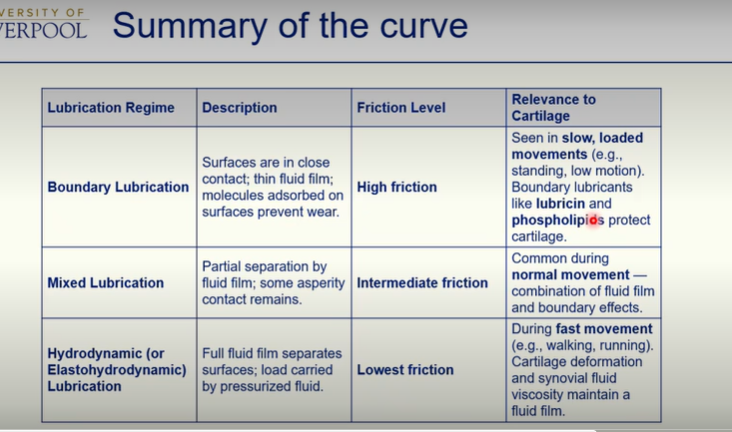
What is Boundary Lubrication?
involves lubricant molecules attached to the articular surface (i.e. lubricin, phospholipids).
prevents the cartilages surfaces coming into direct contact
reduces friction and prevents cartilage wear
Mixed Lubrication can occur - where we get boundary and fluid film lubrication occur together.
Lambda Ratio
Lambda ratio is the minimum film thickness (h) needed in relation to the roughness of the surfaces.
A higher lambda ratio indicates greater separation between surfaces and suggests a move towards full fluid film lubrication, which is the ideal scenario with minimal wear due to low friction.
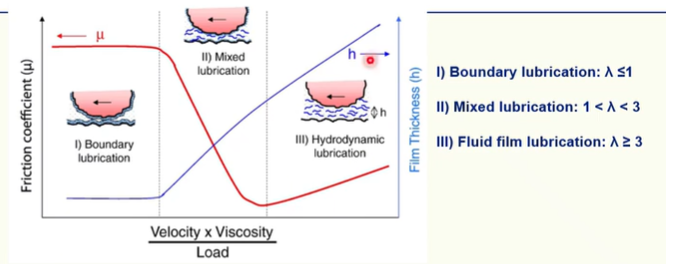
Model Stribeck curve - where the friction coefficient and the fluid film thickness are plotted as a function of velocity, fluid viscosity and load for the boundary, lubrication and hydrodynamic lubrication regimes.
Lubrication in disease
In healthy joints, the lambda ratio is about 1-3, meaning the joint operates in mixed fluid-film modes of lubrication, maintaining a low friction.
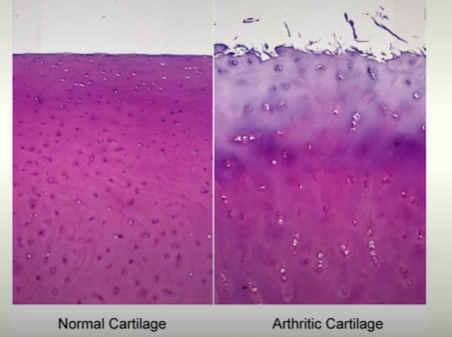
In osteoarthritis where cartilage matrix is altered and cartilage is degraded:
surface roughness can increase
fluid film thickness can decrease (due to loss of key proteins such as lubricin, aggrecan etc, which can affect osmotic balance)
can reduce the lambda towards boundary lubrication, with increased friction —> may increase mechanical wear of the cartilage, alongside non-mechanical changes!
Osteoarthritis
it is a heterogenous (a medical condition with diverse multifactorial causes), whole joint disease
affects over 500 million people worldwide
causes pain
leading cause of disability and premature work loss
no effective treatment
causes degradation of cartilage mass
marked by cell stress and ECM degradation
Multifactorial and complex disease
all joint tissues have a role
cartilage, synovium, discs, bone, osteophytes, fat pad, tendons, ligaments, synovial fluid etc
obesity and joint injury increase risk of getting OA
inflammation, metabolic alterations and trauma
OA and ECM
Imbalance between catabolic and anabolic processes
Cartilage
increase in enzymes that breakdown matrix
e.g. MMPs, aggrecanases, collagenases, low tensile strength, resilience, osmotic effect
Subchondral bone
increased bone turnover and sclerosis of the bone adjacent to the cartilage
osteophytes (bony spurs)
microfractures
What happens in OA?
There is excessive activity of matrix degrading enzymes that break down collagen and proteoglycans.
Collagen becomes disorganised.
Cartilage becomes thinner and cracked, compromising its cushioning function, and causing joint pain and stiffness.
May get cartilage fibrosis as it tries to repair.
proteoglycan loss is an early indicator of OA
MSK: Cartilage and Bone Growth
L.O. Describe the embryology of normal limb growth.
L.O. Describe the function and structure of different types of cartilage.
L.O. Describe the functional importance of epiphyseal plates and the process of growth.
L.O. Describe the structure, function and role of chondrocytes in growth.
L.O. Describe how hormones control and modify bone growth.
L.O. Describe the differences between membranous and endochondral ossification processes.
L.O. Describe the process of bone growth, modelling and remodelling.
Three Embryonic Germ Layers
3rd week of human development
—> Gastrulation occurs:
Formation of the trilaminar embryonic disc that contains the primary germ layers.
—> will form all foetal tissues
—> establishment of major body axes
Ectoderm - outer skin which forms the covering of the body as well as nervous system
Endoderm - inner skin which forms the lining of the gastrointestinal and respiratory systems and urogenital systems and associated glands
Mesoderm - middle skin which forms the skeletal, connective and muscle tissues of the body and some organs and glands (everything else basically) - limb bud comes from here
Limb Bud development - from Mesoderm
Week 4
Limb buds appear towards the end of the 4th week of development
Upper limb bud (26-27 days)
Then lower limb buds 1-2 days later
The limb bud consists of a mass of mesenchyme covered by a layer of ectoderm.
Thickening of ectoderm at the apex of each limb bud forms the apical ectodermal ridge (AER).
The AER….
promotes outgrowth of the bus
bone morphogenetic protein (BMP) is essential for this
retinoic acid promotes formation of the limb bud, by inhibiting fibroblast growth factor 8
The AER influences growth and development of the limbs along a proximodistal axis
FGFs from the AER cause expression of sonic hedgehog which controls anteroposterior patterning
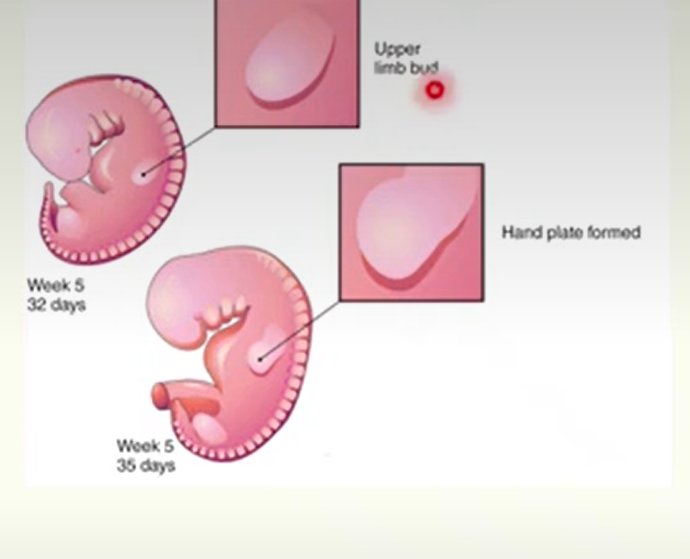
Week 6
digital rays being to develop in hand plates
5-8 days later for lower limb (in week 7)
these outline the pattern of the digits
digital rays are separated by loose mesenchyme
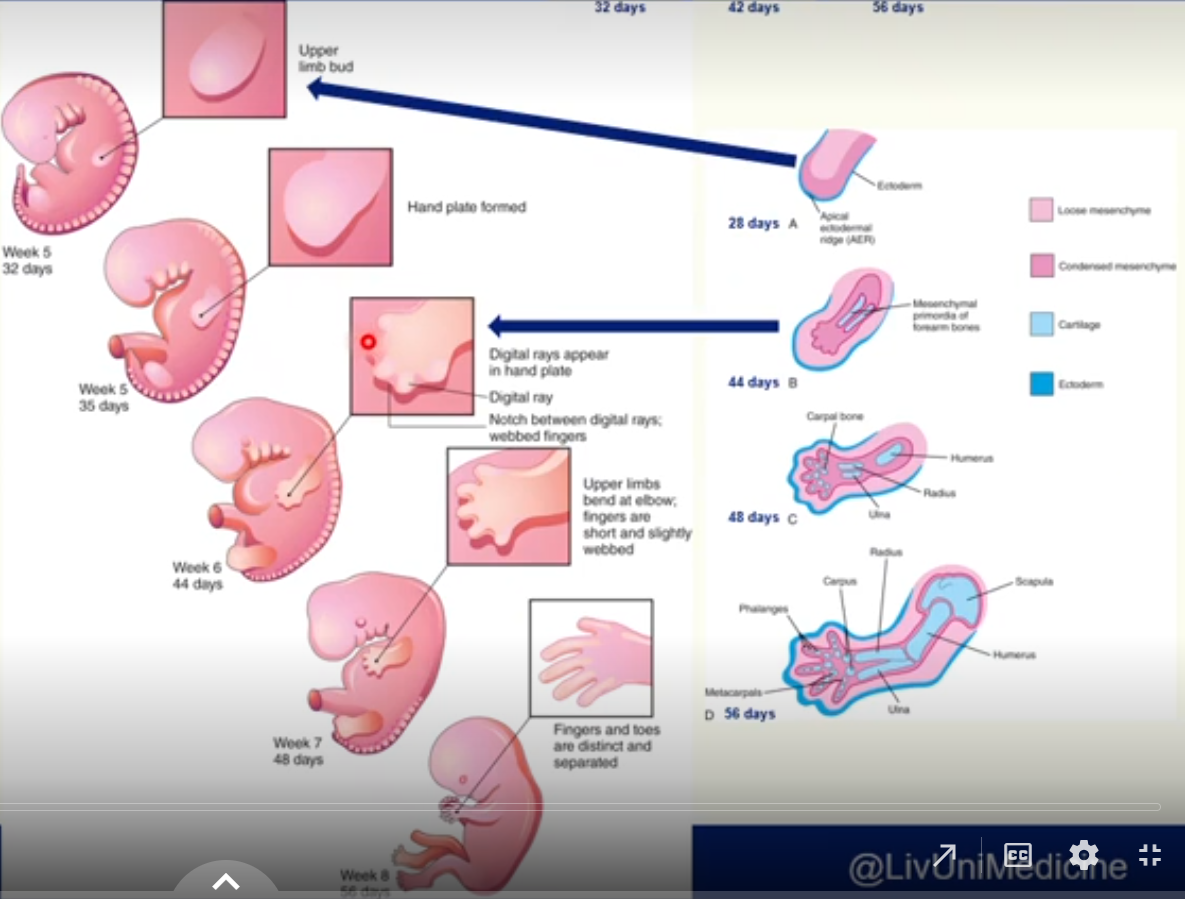
Week 7
limbs change considerably
loose mesenchyme undergoes apoptosis forming notches between the digital rays, separating future digits
Week 8
fingers and toes are now separate digits
coordinated limb movement begins
hands and feet rotate into position
Limb rotation and adult anatomy
During week 8, the limbs rotate in opposite directions
Upper limb rotates 90 degrees laterally.
extensor muscles are on lateral and posterior surfaces
thumbs lie laterally
Lower limb rotates 90 degrees medially
extensor muscles are on the anterior surface
big toe is medial
Limb bud tissues
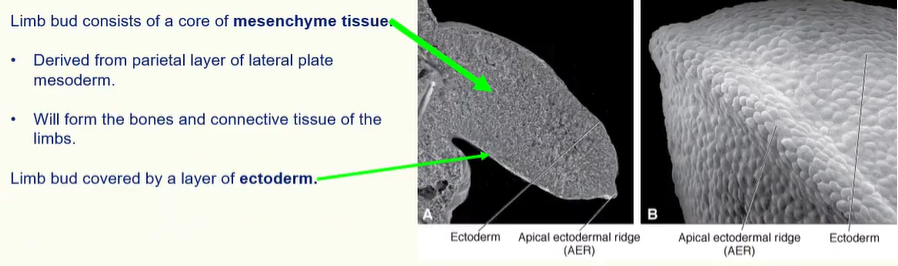
this ectoderm is thickened at the distal end of the limb bud to form the apical ectodermal ridge (AER)
The AER is important for regulating limb development
Cells nearest to it remain undifferentiated.
Cells further from it start to become cartilage and muscle.
Limb development proceeds proximodistally.
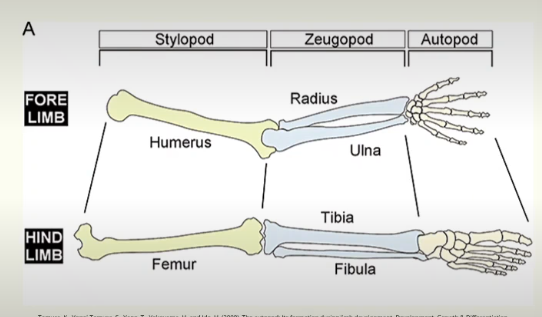
Three segments to the limb
Limb develops from proximal to distal into its three components
Stylopod = humerus/femur
Zeugopod = radius and ulnar / tibia and fibular
Autopod = carpals, metacarpals and digits / tarsals, metatarsals and digits
Limb Bone development
The Mesenchyme in a limb bud gives rise to bones, ligaments and blood vessels.
As the limb buds elongate in week 5, the mesenchymal models of the bones are formed by cellular aggregations that become chondrification centres. (cells differentiate into chondroblasts).
By the end of week 6, the entire limb skeleton is cartilaginous.
Osteogenesis of long bones begins in 7th week.
primary ossification centres in the diaphysis
all long bones have ossification centres by week 12
primary ossification of carpal bones begins after birth (during first year)
Muscles come from somites (also mesoderm).
Motor and sensory nerves come from spinal cord (ectoderm).
Development of bone and cartilage cells
Key genes expressed during chondrogenic and osteoblastic differentiation.
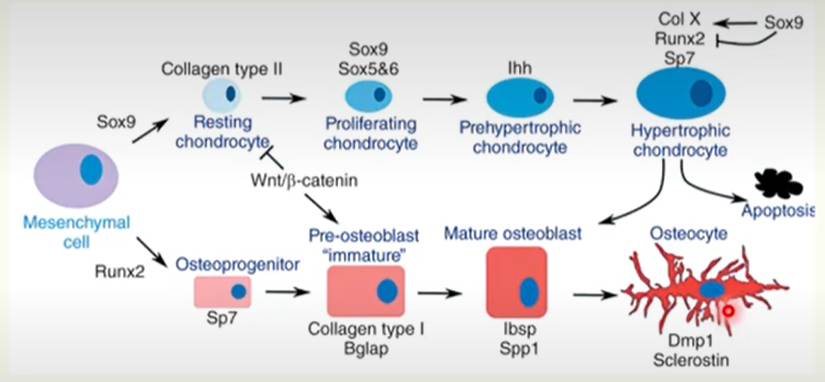
Key chondrocyte genes:
SOX9 (transcription factor)
COL2
IHH (for hypertrophy)
Key Osteoblast genes:
RUNX2 (transcription factor)
COL1
SP7 (osterix; transcription factor)
BGLAP (osteocalcin; marker of bone formation)
IMPORTANT!
Sox9 persists in chondrocytes until they become hypertrophic.
induces collagen X
inhibits RUNX2 (osteoblast marker)
Key Osteocyte genes:
DMP1 (regulates phosphate homeostasis and bone mineralisation)
Sclerostin (inhibits bone formation)
When chondrocyte-osteoblast transformation occurs, SOX9 is degraded, allowing expression of RUNX2 (chondrocyte —> osteoblast).
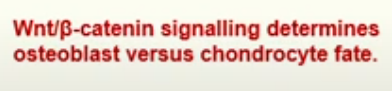
An overview of Joint Formation
gene expression is controlled spatially and temporally to cause joint formation. This is the simplified version:
cells in the cartilage model express Sox9, Col2 and Dcx. Joint site is determined.
Gdf5 expression is activated with other inter-zone-specific genes. Cells in the cartilage model are Sox9, Col2 and Matn1 positive.
Gdf5 positive cells that are Matn1 negative become articular chondrocytes
(Gdf5 is critical for articular cartilage development)
Joint cavitation occurs and development of other joint tissues occurs (ligaments meniscus etc)
Where does bone come from?
Mesenchyme
from mesenchymal membranes
intramembranous bone formation
most facial bones are formed from mesenchyme
skull vault and clavicles are formed from mesenchyme
Cartilage
cartilage models that are replaced by bone
endochondral bone formation
the base of the skull, vertebral column, ribs, sternum, limb girdles and limb bones are formed this way
Both osteogenesis and chondrogenesis are programmed early in development.
Independent processes, under the influence of molecular and vascular events.
Hox genes, BMPs (5 and 7), GDF5, VEGF and other signalling molecules are important in the regulation of cartilage and skeletal development.
B-catenin levels commits skeletal precursors to become chondrocytes and osteoblasts.
Ossification
the process of laying down bone
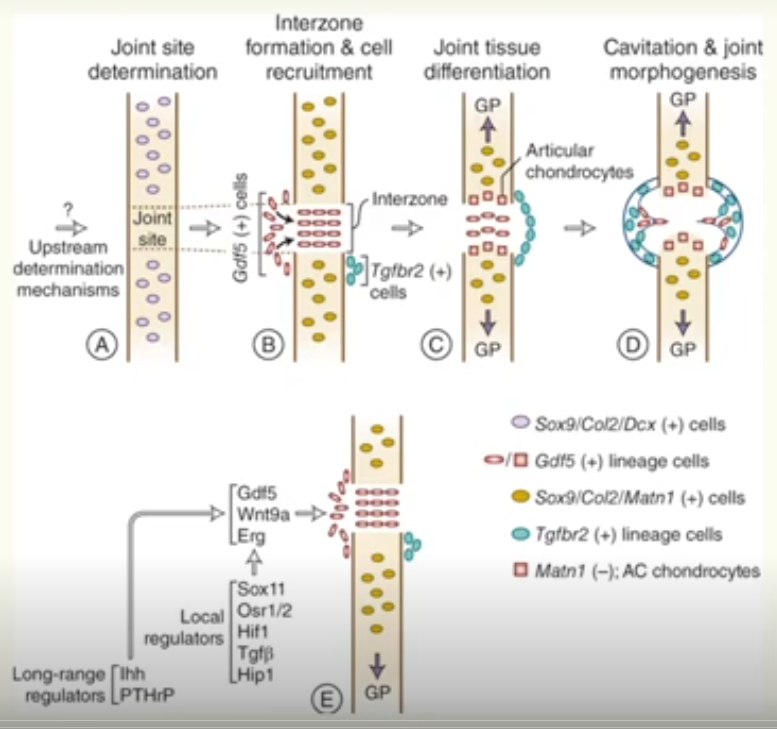
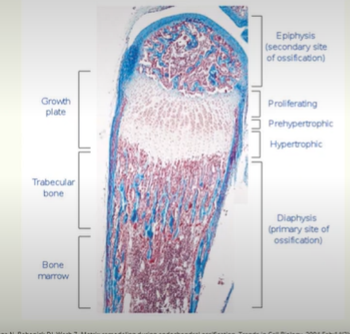
Typical anatomy of a gross long bone
Diaphysis - cylindrical shaft, composed of compact bone.
Epiphysis - expanded ends of the bone.
Metaphysis - between epiphysis and diaphysis.
Medullary cavity
surrounded by a shell of compact bone
contains bone marrow
site of blood production (red marrow) but becomes progressively replaced by adipose tissue (yellow marrow).
Periosteum - outer lining
Endosteum - inner lining
Articular surfaces (hyaline cartilage)
Endochondral Ossification
endochondral ossification of a typical long bone
Mesenchymal cells condense and express Sox9.
prehypertrophic chondrocytes differentiate and secrete collagen type II and other matrix proteins (i.e. proteoglycans) and perichondrium develops in diaphysis region.
some chondrocyte become pre-hypertrophic (IHH) and then hypertrophic (enlarged, collagen X), surrounded by a calcified matrix
this increases the size of the cartilage model, usually elongating it.
A bone collar forms; hypertrophic chondrocytes gives rise to osteoblasts in the region of the perichondrium, forming cortical bone.
Ossification begins when the developing bone is invaded by blood vessels that branch from limb vasculature.
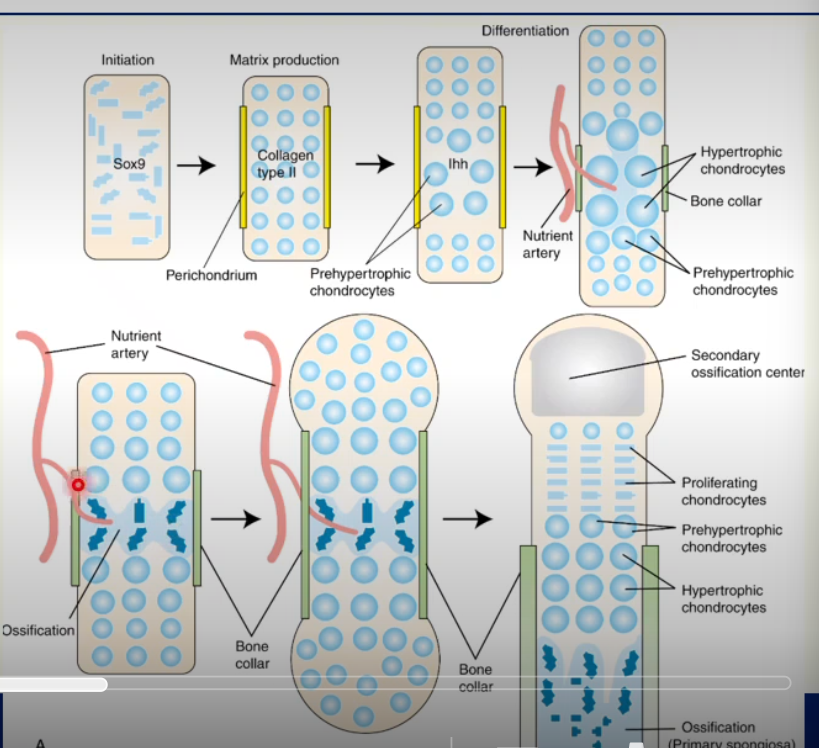
blood vessels bring pre-osteoblastic cells that differentiate into osteoblasts.
osteoblasts can also arise from the hypertrophic chondrocytes (degradation of Sox9)
these osteoblasts form the primary spongiosa, by laying down collagen type I and the mineralised bone matrix. The cartilage matrix is broken down and replaced by bone.
ossification then spreads from the primary ossification centre towards the epiphyses, forming a loose trabecular network of bone.
blood vessels also bring osteoclasts, which are important for remodelling the growing bone (and throughout adult life)
At birth, the diaphysis has a bone collar and trabecular bone core. The epiphyses are still cartilaginous.
at birth, secondary ossification centres develop (with blood vessels) in the epiphyses, which gradually ossify.
cartilage remaining at the end of the bone —> articular cartilage.
a layer of cartilage persists between the epiphysis and diaphysis (where it is still growing), in the region of the metaphysis.
epiphyseal cartilage plate
chondrocytes are present in distinct zones: proliferating, pre-hypertrophic and hypertrophic.
chondrocytes are in columns, directing growth along the axis of the bone.
chondrocytes proliferate, differentiate and are then replaced with bone = growth in bone length (interstitial growth).
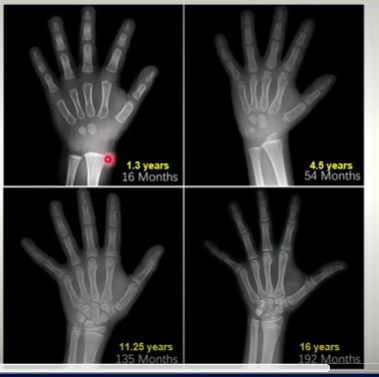
Growing bone example (mouse)
Hand X-rays
Bone Growth
Length (interstitial growth)
bones grow in length via endochondral ossification at the growth plate
actively proliferating plate of cartilage
converted to trabecular bone
progressively increases length of the bone
becomes epiphyseal line (after it ossifies)
Width (appositional growth)
to grow in width and thicken the cortical bone
bone is deposited on the outer surface and resorbed in the inner surface
Intramembranous Ossification
the direct formation of bone within membranes (condensed mesenchyme).
mesenchyme contains mesenchymal stem cells —> osteoprogenitor cells —> osteoblasts
osteoblasts form ossification centres, deposit osteoid and mineralise it. Entrapped osteoblasts will become osteocytes.
initially this occurs in isolated islands, but eventually they merge to form trabecular bone. This is woven bone at this stage.
tissue becomes vascularised. Mesenchyme on the outer surface of the woven bone condenses to form periosteum.
trabecular bone adjacent to the periosteum will be replaced with compact bone.
lamellar bone will replace woven bone
Lamellar versus woven bone
there are two main patterns of bone identified according to the pattern of collagen forming the osteoid (unmineralised bone matrix).
Woven Bone
haphazard organisation of collagen fibres.
mechanically weak
when osteoblasts produce osteoid rapidly
collagen fibres are deposited in an irregular loosely intertwined pattern
initially woven bone is all foetal bone (then remodelling takes place and this bone is replaced by more resilient lamellar bone).
Lamellar Bone
regular parallel alignment of collagen into sheets called lamellae
mechanically strong
virtually all bone in the healthy adult is lamellar
Bone Physiology
Bone is constantly being remodelled throughout life by bone-remodelling units composed of osteoblasts and osteoclasts.
Bones can change their shape and density in response to mechanical load.
Physiological aspects of bone:
the physiology of calcium and phosphate metabolism, formation of bone and teeth, and regulation of vitamin D, parathyroid hormone (PTH), and calcitonin are all closely intertwined.
phosphate homeostasis and calcium homeostasis are closely associated.
What affects bone growth?
Diet
need adequate intake of vitamins and minerals
calcium and phosphorus
vitamin C for collagen synthesis, and differentiation of osteoblasts into osteocytes
vitamin A for stimulation of osteoblasts
Slight changes in calcium can cause extreme immediate physiological effects.
Hormones
IGFs (insulin-like growth factors) stimulate bone growth and maintain bone mass.
IGFs produced by bone and liver.
IGF production is stimulated by hGH (human growth hormone) produced by the anterior pituitary
thyroid hormones and insulin are also important
Far lower or higher phosphate changes does not cause immediate effects on the body.
i.e. low calcium causes nervous system excitement and tetany
i.e. high calcium depresses the nervous system and muscle activity
Bone Matrix
80% of bone is cortical
20% of bone is trabecular
much more porous
greater surface area
greater turnover
Bone is composed of:
Tough organic (protein) matrix (i.e. collagen for tensile strength)
inorganic matrix (i.e. bone mineral)
Inorganic matrix (i.e. bone mineral)
calcium phosphate salts in the form of hydroxyapatite
compressive strength
The concentrations of calcium and phosphate ions in extracellular fluid are considerably greater than those required to cause precipitation of hydroxyapatite.
Why do all tissues not mineralise?
Inhibitors are present in almost all tissues, and the plasma, to prevent precipitation of hydroxyapatite.
An example of an inhibitor would be: Pyrophosphate
In bone, mineralisation of bone matrix occurs when calcium salts are deposited.
This is regulated mainly by pyrophosphate.
Pyrophosphate is then regulated by 3 other molecules secreted by osteoblasts:
TNAP (tissue specific alkaline phosphate)
this breaks down pyrophosphate to allow mineralisation.
NPP1 (nucleotide pyrophosphate phosphodiesterase 1)
produces pyrophosphate outside the cell
ANK (ankylosis protein)
increases extracellular pyrophosphatase
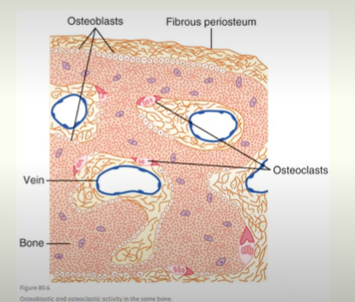
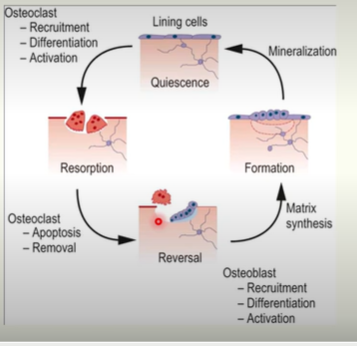
Bone Remodelling
Bone is continuously remodelled
Osteoblasts deposit bone.
osteoblasts found on surfaces of bone
active on about 4% of all bone surfaces
Osteoclasts resorb bone.
found on surfaces of bone
normally active on <1% bone surfaces
PTH controls their activity
Why is it continuously remodelled?
adjust to load: strengthen and change shape
old bone can become brittle and weak: must be replaced.
blood calcium levels
Bone remodelling cycle
The Innervation of the Upper and lower limb
L.O. Outline the functional units of the nervous system and how it is divided.
L.O. Describe the origin and structure of spinal nerves.
L.O. Define the difference between dermatomes versus myotomes including their embryological origin.
The Central Nervous System
the brain and the brain stem AND the spinal cord
responsible for integrating, processing and coordinating sensory data and motor command.
also responsible for higher functions such as intelligence, memory, learning and emotion.
The Peripheral Nervous System
consists of all the neural tissue EXCEPT the brain and spinal cord.
delivers sensory information to the CNS
carries motor demands to the peripheral tissues and systems.
functionally divided into afferent (carry signals toward the CNS) and efferent (carry signals away from CNS to periphery)
A Single Spinal Nerve
Dermatomes and Myotomes
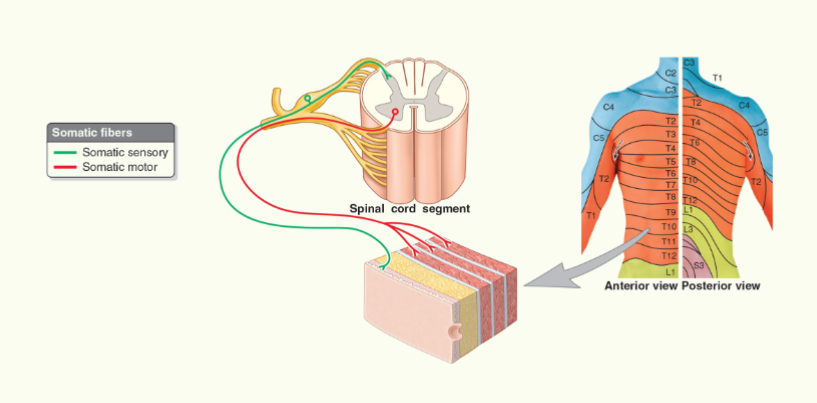
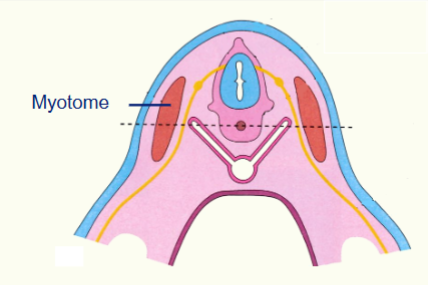
Myotome Embryology
a golden rule of anatomy - when a muscle migrates it brings its nerve supply with it
a single spinal nerve can supply a single muscle = mytome
a single spinal nerve can supply a group of muscles = myotome
myotomes can fuse together. This is why multiple spinal levels may supply a single muscle. The portion of the muscle supplied by a single spinal nerve.
L.O. Describe the structure and major nerves of the brachial and lumbar plexuses.
L.O. Revise ulnar, median and radial nerves and describe how to test each of these.
Brachial Plexus
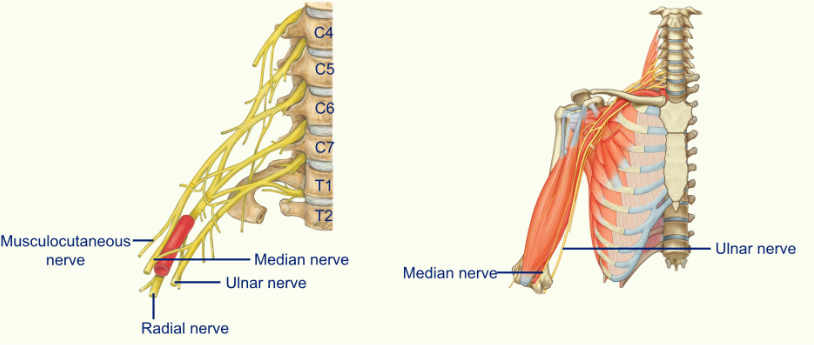
the ulnar nerve is sitting on the median side of the brachial artery
the median nerve starts on the lateral side of the brachial artery and then crosses over to lie on the medial side of the brachial artery
the radial nerve is posterior to the brachial artery
The Radial Nerve
the radial nerve emerges into the posterior compartment through the gap called the triangular interval
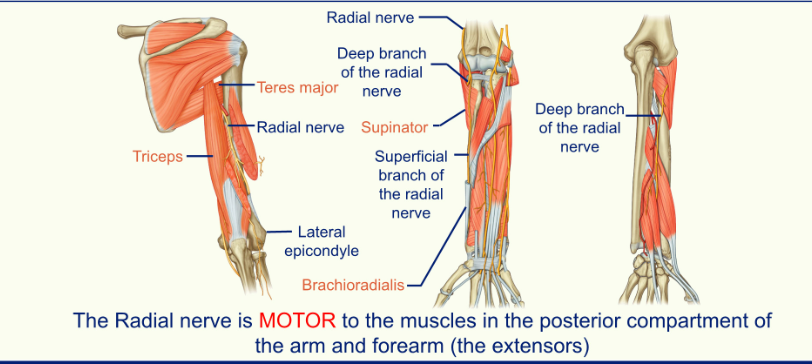
triceps are medial to the radial nerve
teres major is superior to the radial nerve
Cutaneous Innervation
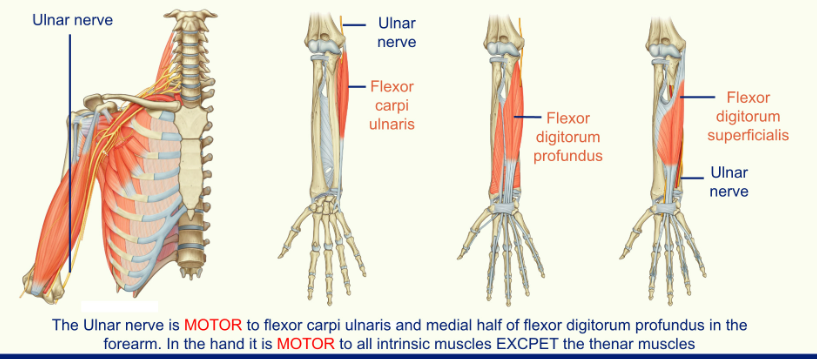
The Ulnar Nerve
the ulnar nerve sits on the medial side of the auxiliary artery of the brachial artery
it travels into the forearm, just posterior to the medial epicondyle
when you hit your funny bone you are actually hitting your ulnar nerve
in the forearm the ulnar nerve runs between the flexor carpi ulnaris and the flexor digitorum profundus
Cutaneous Innervation
The Median Nerve
the median nerve starts in the lateral part of the brachial artery before crossing over to the medial part of the artery and entering the forearm through the space known as the cubital fossa
the nerve travels through the forearm between the two heads of the pronator teres before lying in the same plane as the ulnar nerve (the surface of the flexor digitorum)
the median nerve enters the hand through the carpal tunnel
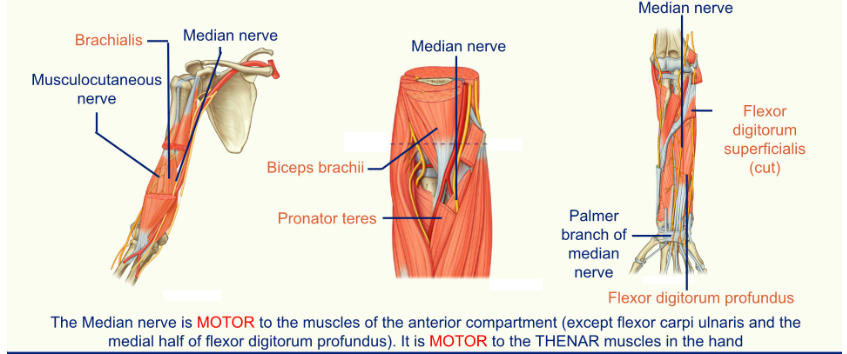
Cutaneous Innervation
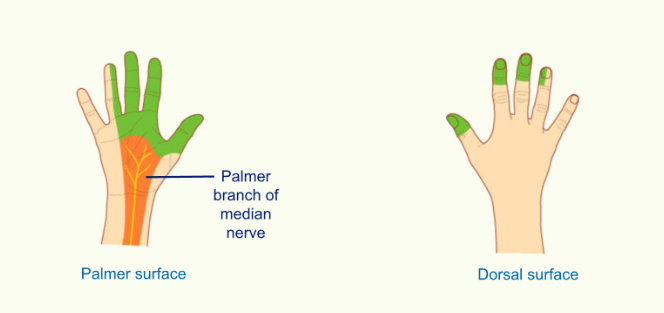
the median nerve has a branch called the palmer branch which innervates the cutaneous surface of the hand
Testing the integrity of the nerves of the upper limb
Radial Nerve
If injury occurs in the arm when the nerve is in the radial groove (usually humeral break)
You get:
weakness of triceps brachii as medial head of triceps is affected
characteristic wrist drop - extensor carpi muscles are paralysed and therefore cannot counteract flexor carpi muscles
inability to extend metacarpophalangeal joints and thumb
if injury occurs in forearm and affects the deep branch of the radial nerve you get the inability to extend the metacarpophalangeal joint
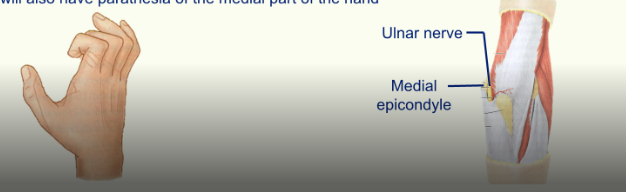
Ulnar Nerve
Ulnar nerve injury commonly occurs when the medial epicondyle fractures
results in the loss of power during wrist adduction. During flexion on the wrist the hand will be drawn to the lateral side due to flexor carpi radialis
affects the intrinsic muscles of the hand - the person is unable to make a fist as they cannot oppose the thumb. The person will have extended MCP joints and flexion of the digits 2 and 3. Person will be unable to adduct and abduct the digits
the person will also have the parathesia of the medial part of the hand.
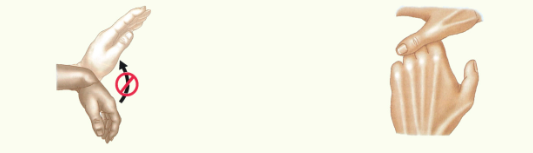
Median Nerve
When severed in the elbow region
difficulty in flexion of the interphalangeal joints (except the 4th and 5th digits which are supplied by the medial part of the flexor digitorum profundus (ulnar nerve)
cannot flex the 2nd and 3rd digits
Carpal Tunnel Syndrome
loss of sensation on the lateral 3 and a half digits. Palm unaffected
difficult to oppose thumb due to thenar muscles being affected

L.O. Describe the innervation of the sciatic and femoral nerves including how you test them.
L.O. Illustrate the importance of the correct location of intramuscular injections (gluteus maximus).
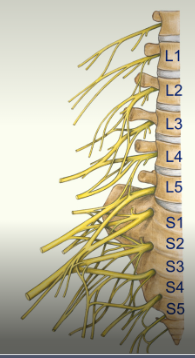
Lumbosacral Plexus
The lumbosacral plexus is formed from the ventral rami of L1-S4.
It gives rise to…
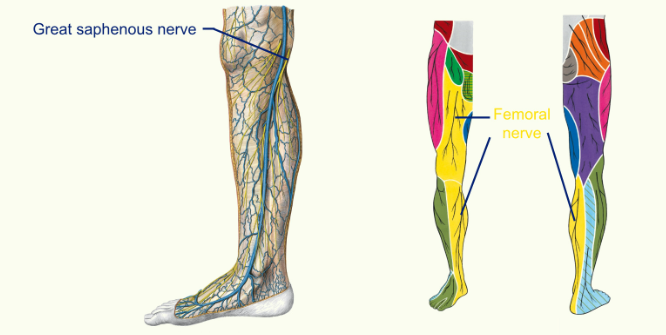
The femoral nerve
motor to the muscles of the anterior compartment
sensory innervation to the anterior thigh, anteromedial knee, medial leg and foot
The obturator nerve
motor to the muscles of the medial compartment
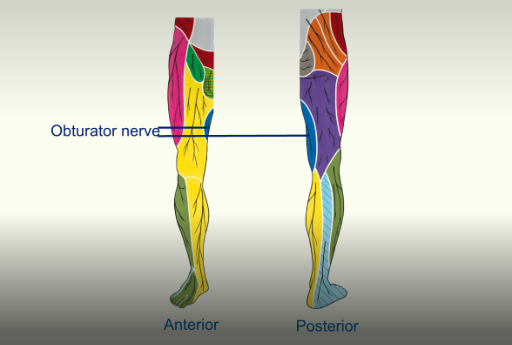
sensor innervation to the proximal medial thigh
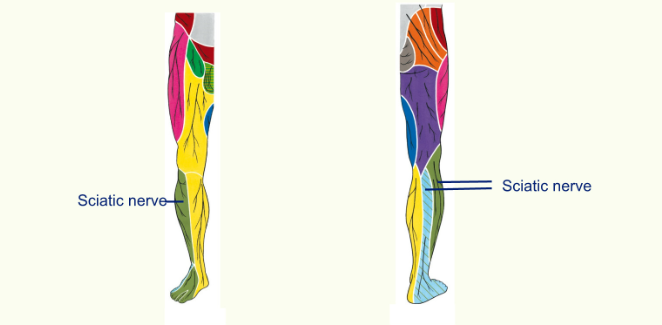
The sciatic nerve
motor to the muscles of the posterior compartment and all the muscles in the leg and foot
sensory innervation to the lateral leg and lateral, dorsal and planter surface of the foot
The Obturator Nerve
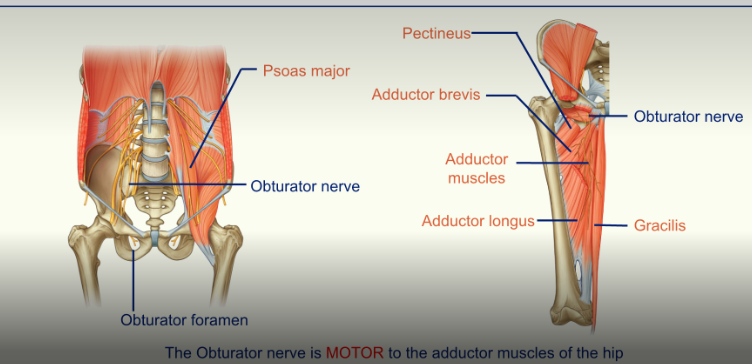
the obturator nerve is MOTOR to the adductor muscles of the hip
the obturator nerve is medial to the Psoas Major
the obturator nerve travels down the pelvic brim and then exits via this obturator foramen
Sensory Supply
The Femoral Nerve
the femoral nerve is motor to the Quadriceps muscle and sartorius
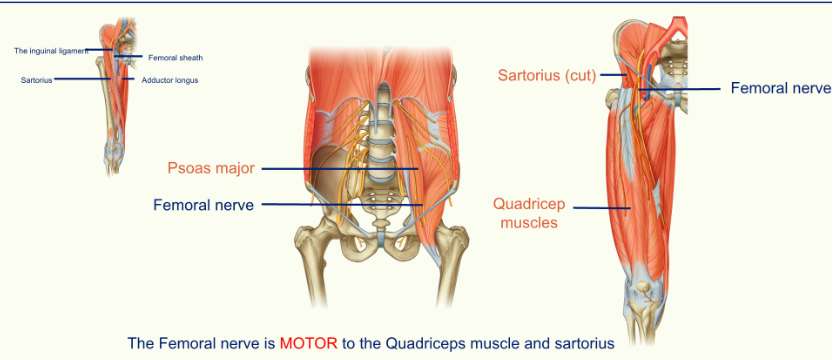
the femoral nerve travels close to the sartorius muscle
femoral nerve helps extension of the knee
femoral nerve gives sensory supply to below the knee
The Sciatic Nerve
the sciatic nerve is motor to the hamstrings and all muscles of the leg and foot
thick nerve
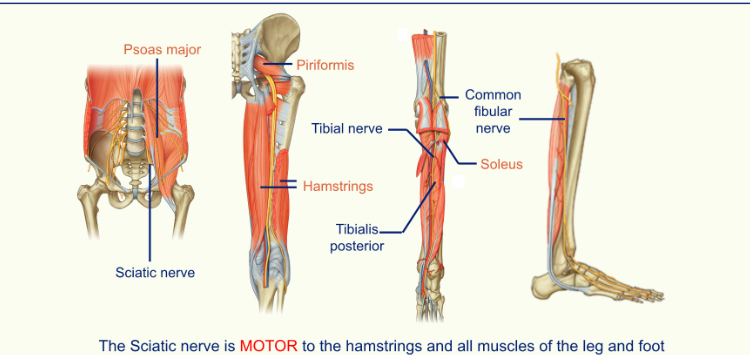
you can use the piriformis muscle to find the sciatic nerve
sciatic nerve innervates the hamstrings
sciatic nerve divides at the knee; tibial nerve and the fibular nerve
the tibial nerve travels down the calf behind the tibia, supplying muscles in the posterior compartment and skin on the back/sole of the foot before splitting into the medial and lateral plantar nerves in the foot.
the fibular nerve divides into a deep fibular nerve (peroneal nerve) which goes to the anterior compartment, and the superficial fibular nerve which goes to the lateral compartment.
Cutaneous Innervation
Intermuscular Injections
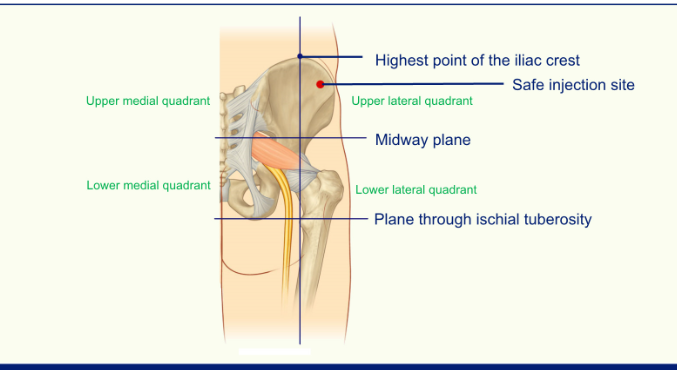
when giving injections you have to avoid the sciatic nerve
stick to the upper lateral quadrant