Examination of the Neck
History of a Neck Lump
• Duration
• First symptom
• Other symptoms
• Progression
• Persistence
• Multiplicity
• Cause
History of a Neck Lump: Duration
• “When did you first notice the lump?”
• Be precise with dates
• Be aware that the lump may have been present months before the patient first noticed it
History of a Neck Lump: First Symptom
• “What made you first notice the lump?”
• Incidental
- The patient felt it while washing
- Someone else noticed it
• Symptomatic
- The patient noticed it when they felt a painful area
History of a Neck Lump: Other Symptoms
• “Does the lump cause any problems?”
• May be:
- Painful
- Disfiguring
- Interfere with function e.g. swallowing
History of a Neck Lump: Progression
• “Has the lump changed since it was first noticed?”
• It may have:
Changed in size
The time frame for change
Rapidly enlarging
Fluctuating in size (congenital cyst)
Become more painful
History of a Neck Lump: Persistence
• “Does the lump ever disappear?”
• Only a few conditions disappear and reappear
e.g. Salivary gland obstruction
• Less likely to be malignant
History of a Neck Lump: Multiplicity
• “Have you ever had a lump like this before?”
• “Do you have any other lumps elsewhere?”
• There may be a link between the neck lump and other lumps
Recurrence of a lump
Systemic causes of lymphadenopathy e.g. Lymphoma, Sarcoidosis
History of a Neck Lump: Cause
• “What do you think caused this lump?”
• The lump may have occurred after an event, injury or illness
History of a Neck Lump: Other important information to elicit
• Age
<16 – The majority are either inflammatory or congenital
16 to 40 – Inflammatory or congenital causes are still most common but malignant causes start to increase
>40 – Should be considered neoplastic, and potentially malignant, until proven otherwise (especially if the patient smokes and/or drinks)
• History of Head & Neck Cancer
• History of skin cancer of the face and scalp
• History of immunosuppression
• Weight loss/night sweats/fever
• Contact with relatives with infectious disease/pets & animals/occupational exposures/recent foreign travel
Red Flags for Malignancy
• Lump present for > 2-3 weeks duration
• Patient > 40 years old
• Tobacco and alcohol use
• Previous history of malignancy (head and neck, skin, lymphoma)
• Immunocompromised (renal transplant)
• Unexplained weight loss
• Other head and neck symptoms
Change in voice/hoarseness
Blood in saliva
Dysphagia/odynophagia
Otalgia
Nasal congestion
Examination of a Neck Lump
• Site
• Size
• Shape
• Consistency
• Tenderness
• Mobility
• Temperature
• Overlying skin
• Fluctuance
Examination of a Neck Lump (ICE)
• Clean hands before examination
• Introduce yourself
• Consent
• Explain what you are going to do
• Obtain verbal consent
• Expose
• Should be able to see everything above clavicles
• Unbutton shirts and remove scarves etc.
Examination of a Neck Lump
• Inspection from the front
• Ask the patient to swallow a sip of water
Watch for any movement of the midline lump
• Palpate from behind in a systematic fashion
• Systematically palpate all levels of the neck
• Remember to examine preauricular and postauricular areas
• Examine oral cavity and oropharynx
• Bimanual palpation of submandibular gland
the
• Examine the skin of the face and scalp
Description of a Neck Lump: SITE
• Description of anatomical location
• Neck level
• Think of underlying anatomical structures
Midline – thyroid
Pre-auricular – parotid
Lateral neck – lymph node
Description of a Neck Lump: SIZE
• Measure with a ruler
Length
Width
• Use common objects/food
Golf ball
Pea
Description of a Neck Lump: SHAPE
• Round
• Oval
• Pear shaped
• Kidney shaped
Description of a Neck Lump: SURFACE
• Smooth
• Irregular
Description of a Neck Lump: EDGE
• Discrete
• Diffuse
Description of a Neck Lump: CONSISTENCY
• Rock hard: Bone
• Firm: Hard but not as hard as bone
• Rubbery: Slightly squashable – rubber ball
• Spongy: Squashable – some resilience
• Soft: Squashable – no resilience
Description of a Neck Lump: MOBILITY
• Relationship between the lump and surrounding structures
• Move independently
• Fixed
Description of a Neck Lump: TEMPERATURE
• Hot or normal temperature
• Assess by feeling a lump with the dorsum of the hand (back of the hand)
• Hot - inflammatory process
Description of a Neck Lump: TENDERNESS
• Ask the patient if the lump is tender before palpating
• If so be gentle!
• Look at the patient’s face while palpating to assess the severity of tenderness
Description of a Neck Lump: OVERLYING SKIN
• Look at colour
• Look for breaks in skin/ulceration
• Puckering
• Orange peel skin (peau d’orange)
Description of a Neck Lump: FLUCTUANCE
• Fluid filled/cystic
• Compression to one point causes expansion elsewhere
RED FLAGS
• Size > 1cm
• Round or irregular
• Firm
• Fixed
• Normal temperature
• Non-tender
• Overlying skin ulcerated (fungating)
Differential Diagnosis
Surgical Sieve
• Congenital
• Acquired
• Vascular
• Inflammatory or Infective
• Traumatic
• Autoimmune
• Metabolic
• Idiopathic
• Neoplastic
Primary
Metastatic
• Degenerative
• Environmental
VITAMIN C, D, E
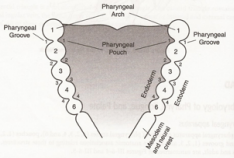
Congenital
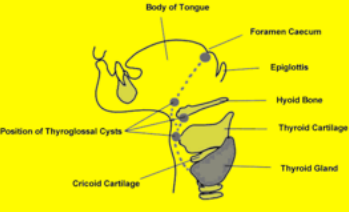
Thyroglossal Duct Cyst
• Most common congenital neck mass - 70%
• >50% before age 20yrs
• 75% midline
• 65% infra-hyoid
• Fluctuant
• Painless unless it becomes infected
• Moves when patient protrudes tongue (fixed to hyoid bone)
Branchial Cyst
• Remnant of branchial cleft (usually 2nd)
• Stratified squamous epithelium with lymphoid tissue
• Smooth, fluctuant mass level 2. Anterior to SCM
• Present post-URTI in an older child/young adult
• Painless fluctuant swelling
• Remember > 40 yrs = Malignant until proven otherwise
Haemangioma
• Most common paediatric tumour
• 0.5 % H&N tumours
• Proliferate/involute
• Haemangiomas usually resolve
• Complicated lesions may require treatment
• Propanolol
• (90% by 9 years)
• CT/MRI
Lymphatic Malformations
• “Cystic Hygroma”/“Lymphangioma”
• Present neonate (90% by 2yrs)
• Painless, fluctuant
• Cystic Hygroma usually found at the base of the posterior triangle
• No regression
• Require Rx.
Sclerosing agents
Resection
Acquired
Surgical Sieve
• Congenital
• Acquired
Vascular
Carotid Body Tumour
Carotid Aneurysm
Inflammatory or Infective
Bacterial
Viral
Protozoal
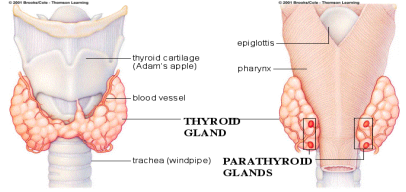
Thyroid
Traumatic
Autoimmune
Thyroid
Metabolic
Thyroid
Neoplastic
Primary
Thyroid
Lymphoma
Salivary
Metastatic
Skin
Oral/Oropharyngeal
Salivary
Thyroid
Distant
Degenerative
Idiopathic
Thyroid
• Autoimmune
Hashimoto’s
Graves’
• Neoplastic
Benign
Adenoma
Malignant
Follicular
Papillary
Anaplastic
Medullary
• Endocrine
Physiological
• Degenerative
Simple
Multinodular goitre
• Infective
De Quervains
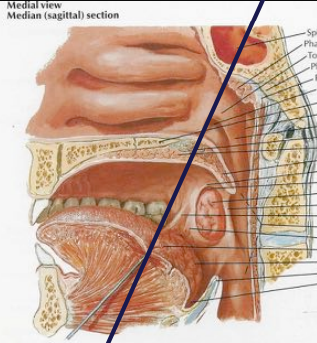
Anatomy – Site Classification
• Oral Cavity
Oral Tongue (Ant 2/3)
Floor of Mouth
Buccal Mucosa
Retromolar Trigone
Mandible/Hard Palate/Alveolus
• Oropharynx
Base of Tongue (Post 1/3)
Tonsil & Tonsillar Fossa/Pillars
Soft Palate/Uvula
Posterior pharynx
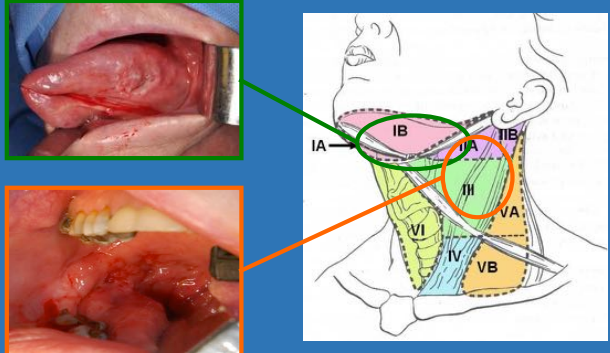
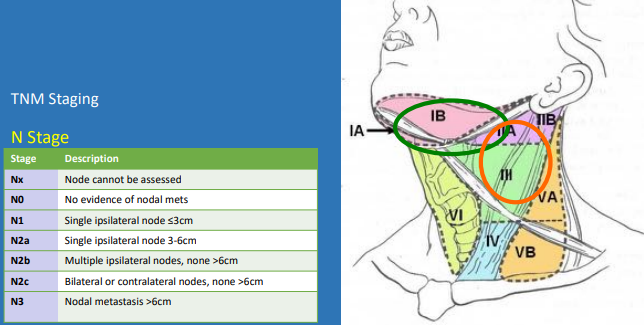
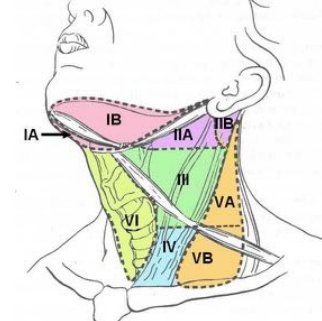
Anatomy – Cervical Lymphatics