POTS, Inappropriate Sinus Tachycardia, Vasovagal Syncope
Introduction
Discussion on high-risk patient populations with VBS (Vasovagal Syncope), POTS (Postural Orthostatic Tachycardia Syndrome), and inappropriate sinus tachycardia.
Prognosis for long-term survival is generally excellent, yet many face significant quality of life issues.
Patient Case Studies
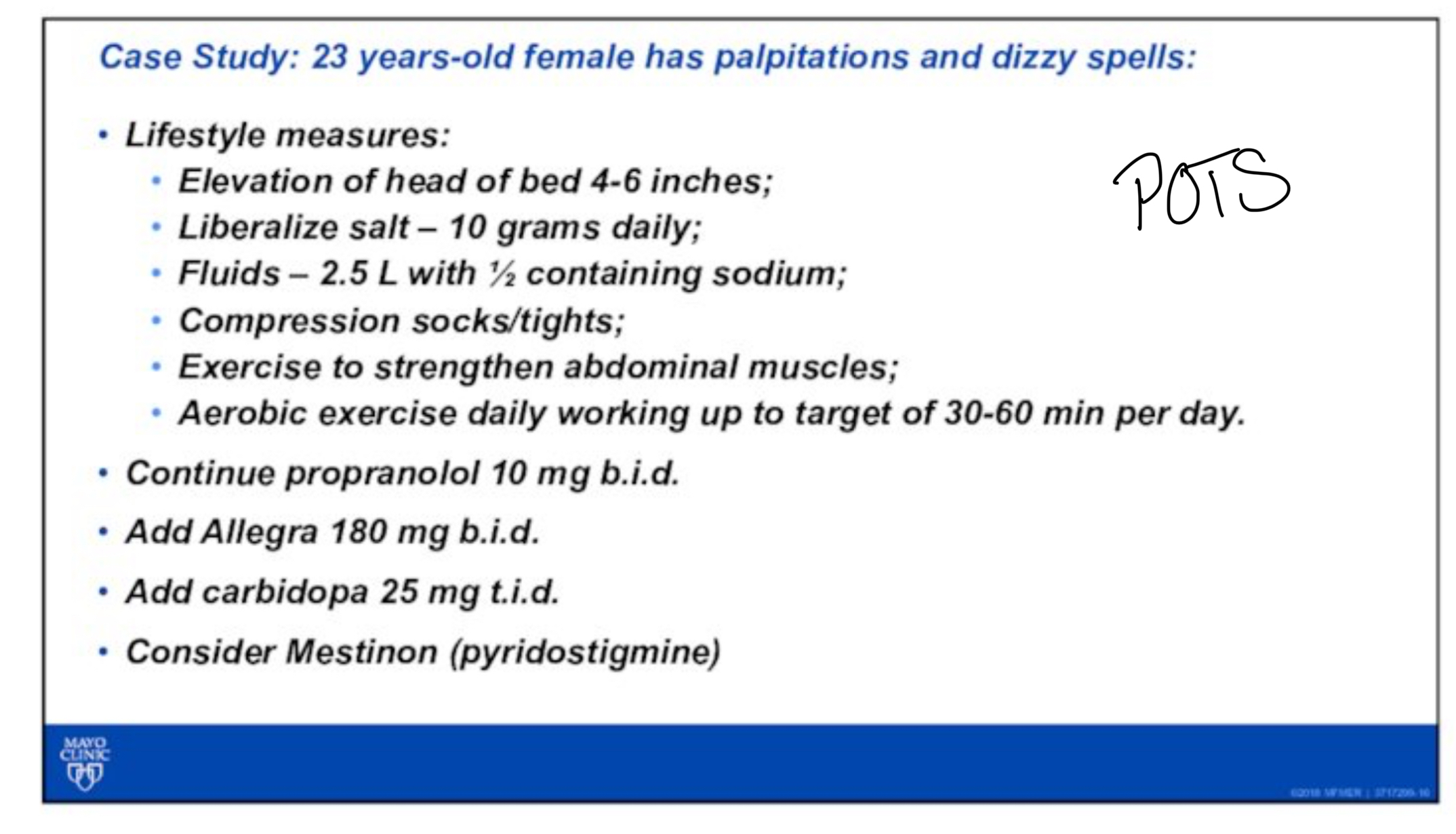
Case 1: 23-Year-Old Female
Symptoms developed post-viral infection; experienced palpitations, dizziness, light-headedness, and visual changes.
Heart Rate Monitoring:
Minimum heart rate: 67 bpm
Peak heart rate: 178 bpm
Average heart rate: 87 bpm (significant fluctuations noted throughout the day).
Tilt Table Test Results:
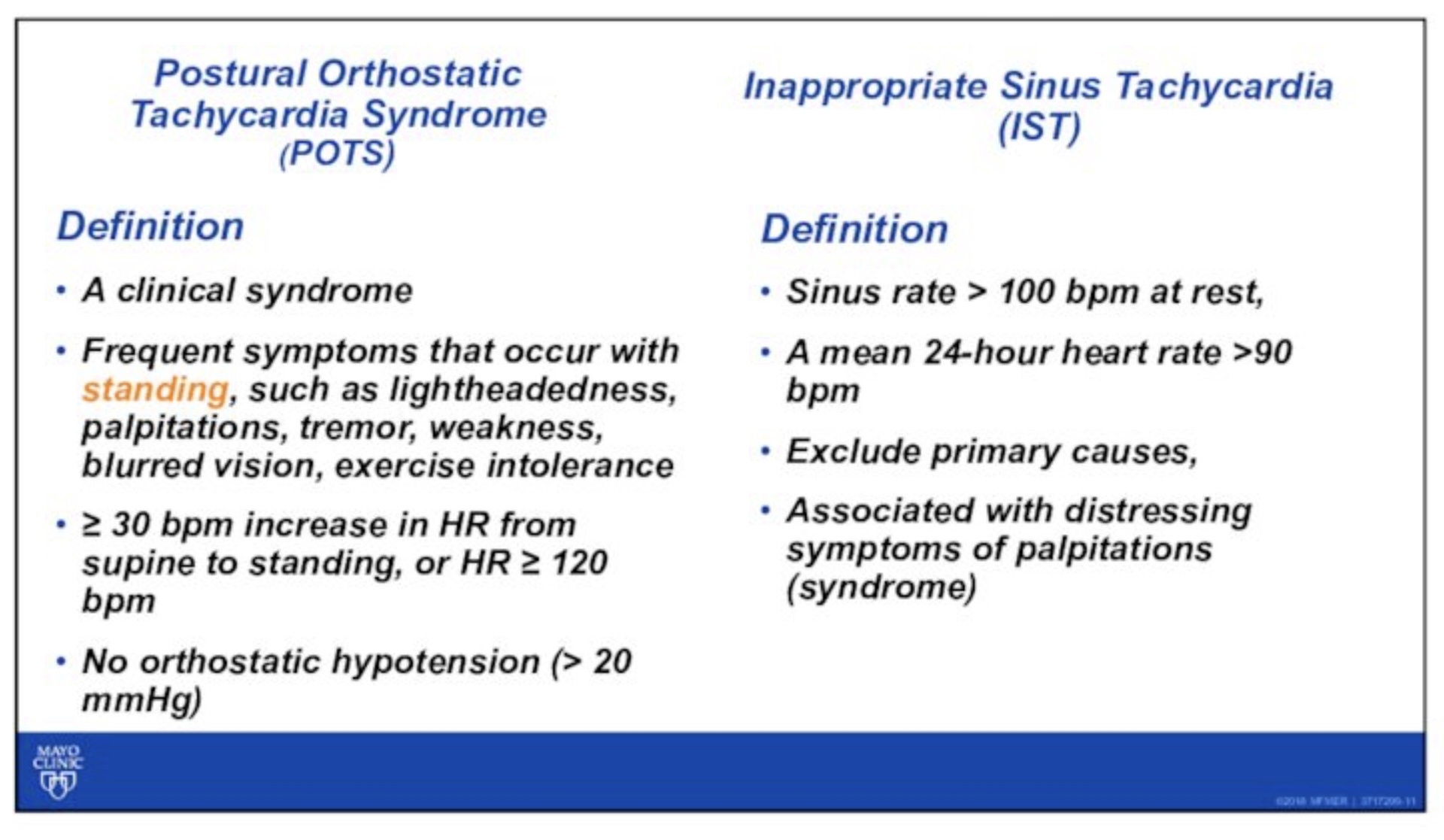
Heart rate increased by ~50 bpm upon tilt, no significant orthostatic hypotension observed, although pulse pressure narrowed with tilt.
Consistent with POTS
Case 2: 52-Year-Old Female
Heart Rate Monitoring:
Minimum heart rate: 77 bpm
Maximum heart rate: 157 bpm
Average heart rate: 82 bpm (persistent sinus tachycardia during awake hours).
Tilt Table Test Results:
Heart rate increase of ~20 bpm; systolic pressure stability under dynamic conditions.
Patient Definitions and Differentiations
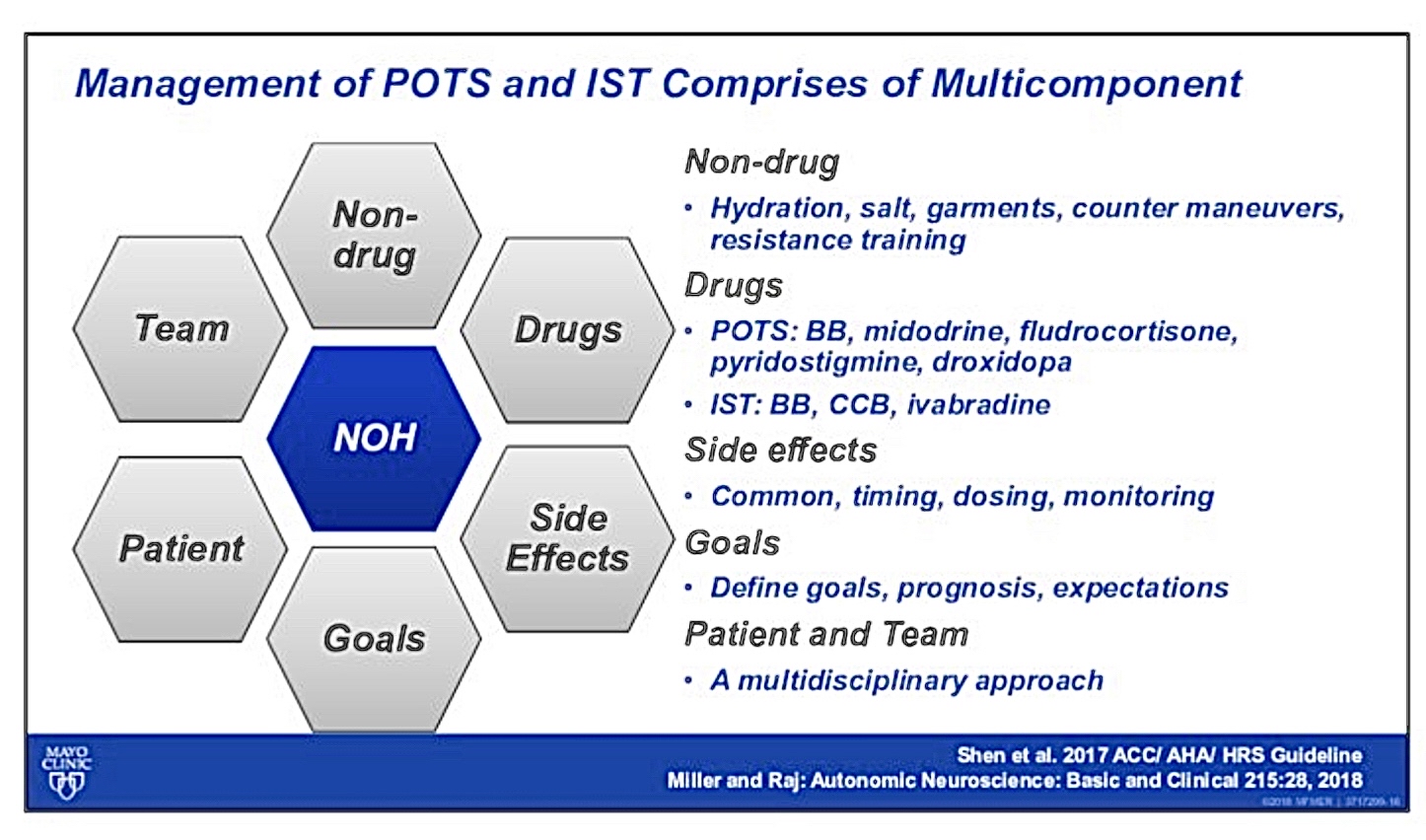
Clinical Management Strategies
General Management Recommendations
Increase in salt intake (10 grams over 24 hours) and fluid intake (2.5 liters).
Recommend daily exercises focusing on strengthening abdominal muscles and wear compression garments.
Tragus nerve stimulation for POTS is emerging as an effective therapy
Invasive Procedures and Surgical Options
Discussed the potential for sinus node sparing hybrid surgical and ablation procedure for inappropriate sinus tachycardia syndrome. In one study where cohorts was 80% IST and 20% POTS patients, HR improved from avg 110bpm to 60bpm at 6mo follow up. Most common complication was pericarditis in 9% of 225 patients in the study.
Selection criteria for invasive procedures remain undefined, indicating a need for further research.
Refractory Vasovagal Syncope
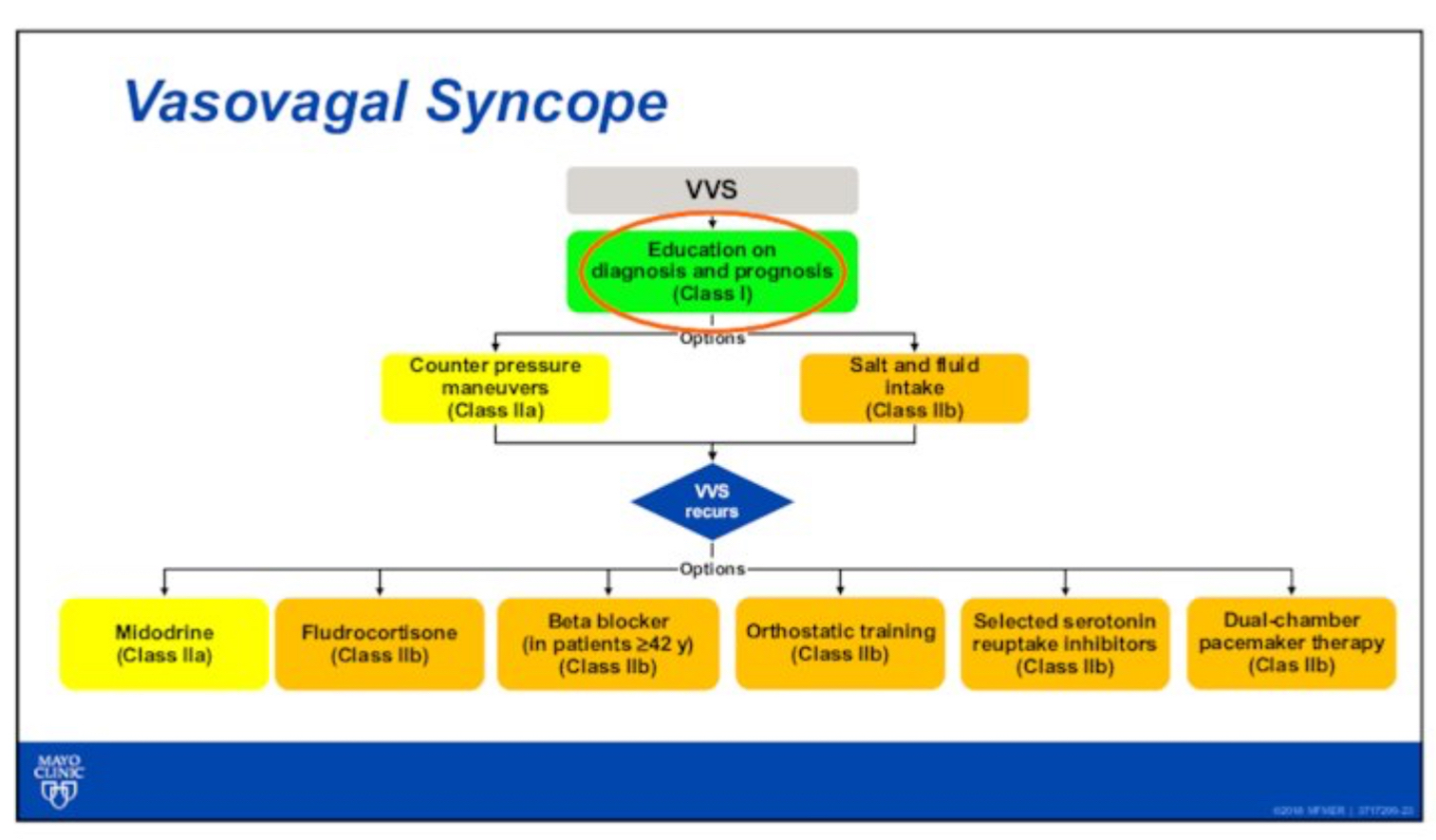
Consideration of cardioneuroablation to reduce vagal surges among patients with recurrent symptoms.
Lack of standardization in treatment protocols for vasovagal syncope.
Conclusion
Importance of clinical guidance and individualized patient management strategies based on varying presentations and responses to treatment.