Calcium signalling
Ca2+ has allosteric (causes conformational changes) effects on enzymes and proteins. Resting cytoplasmic [Ca2+ ] is approx 100 nM, 20,000- to 100,000x lower than extracellular concentration. Resting conc maintained by active transport to the extracellular space, ER and sometimes mitochondria. Storing of calcium occurs mainly in the ER but also in the mitochondria.
Recap of ER (endoplasmic reticulum): biggest organelle by volume. Forms interconnected network of flattened membranous sacs OR cisternae (tubelike). Membranes continuous with outer nuclear membrane. Calcium is pumped into the ER from the cytosol via ATPase SERCA. Once in the ER, calcium binds storage protein calsequestrin to achieve high conc, creating steep calcium gradients.
Signalling occurs as a result of cell stimulation to release calcium from intracellular stores, and/or when calcium enters the cell. Pumping calcium occurs either using ATP via plasma membrane Ca-ATPase or cotransport eg with Na+. This occurs via Na/Ca antiporter which uses the sodium conc gradient to move Ca against its. Depending on the event taking place, calcium conc may increase in a rapid, momentary way or slow and sustained.
Symporters and antiporters? Looks like symporter = both ions/molecules move in same direction and antiporter = molecules move in opposite directions.
The movement of calcium ions DOWN the gradient via open channels is much more rapid than active transport/pumping of calcium. Calcium channels tend to be tetramers with pores through the middle. Increasing intracellular [Ca2+] is a common signalling mechanism, triggered by certain GPCRs which cause transient opening of calcium channels in the ER.
A key part of calcium signalling is phospholipase C activation by GTP-binding protein (G-protein). Phospholipase C hydrolyses phosphatidylinositol 4,5 bisphosphate forming inositol 1,4,5 triphosphate (IP3) and diacylglycerol (DAG) (this was in BM210).
Examples of Ca-regulated events are activation of signalling by PKC and vesicle exocytosis in beta cells.
Activation of signalling by PKC
IP3 opens an ER calcium channel causing release of calcium. It does this by binding a binding site on the channel causing a conformational change - allosteric modification of protein function. Calcium ions and DAG activate a kinase from the protein kinase C family. Protein kinase Cs are homologous proteins made up of several different domains. Ca2+ binds the C2 domain, changing PKC’s shape and encouraging binding to the membrane by linking PKC to negatively charged phosphatidylserine. DAG binds the C1B domain which causes further conformational changes, activating the kinase. The kinase is localised to the correct compartment. This results in signal transmission.
Vesicle exocytosis in the beta cell
Beta cells are responsible for the release of insulin which is a hormone that causes blood glucose concentration to decrease.
Glucose is taken up by beta cells via GLUT2 uniporters
Glycolysis and respiration increase ATP:ADP
[ATP] increase → ATP sensitive K+ channels close
membrane depolarises
voltage gated Ca2+ channels open
rapid Ca2+ influx → fusion of insulin secretory vesicles with plasma membrane
Voltage gated Ca2+ channels are also found in the neuron localised to the synaptic cleft. They are very sensitive and powerful so their response is rapid. Calcium channels are evolutionary conserved structures and may be voltage gated, second messenger operated eg IP3 sensitive, or receptor operated.
Calcium channels in medicine:
Calcium channel blockers and ACE inhibitors make up 60 to 70% of high BP prescriptions in the UK and US. Calcium channel blockers are also used to treat irregular heartbeats among other syndromes. These drugs cost the NHS over 200 million a year but have saved approximately 250 million pounds by preventing heart attacks.
Calcium channel blockers slow down heartrate by acting on the sinoatrial node, allowing the left ventricle to fill completely and lowering cardiac workload. They reduce contractile force by acting on the cardiac muscle and also act on vascular smooth muscle reducing arterial constriction to lower blood pressure.
There are 3 classes of calcium channel blockers: dihydropyridines (eg nifedipine and amlodipine), phenylalkylamines (eg verapamil) and benzothiazepine (eg diltiazem). These work in different ways eg verapamil plugs the molecular pore to prevent Ca entry and amlodipine remodels the channel from the outside so calcium lodges inside.
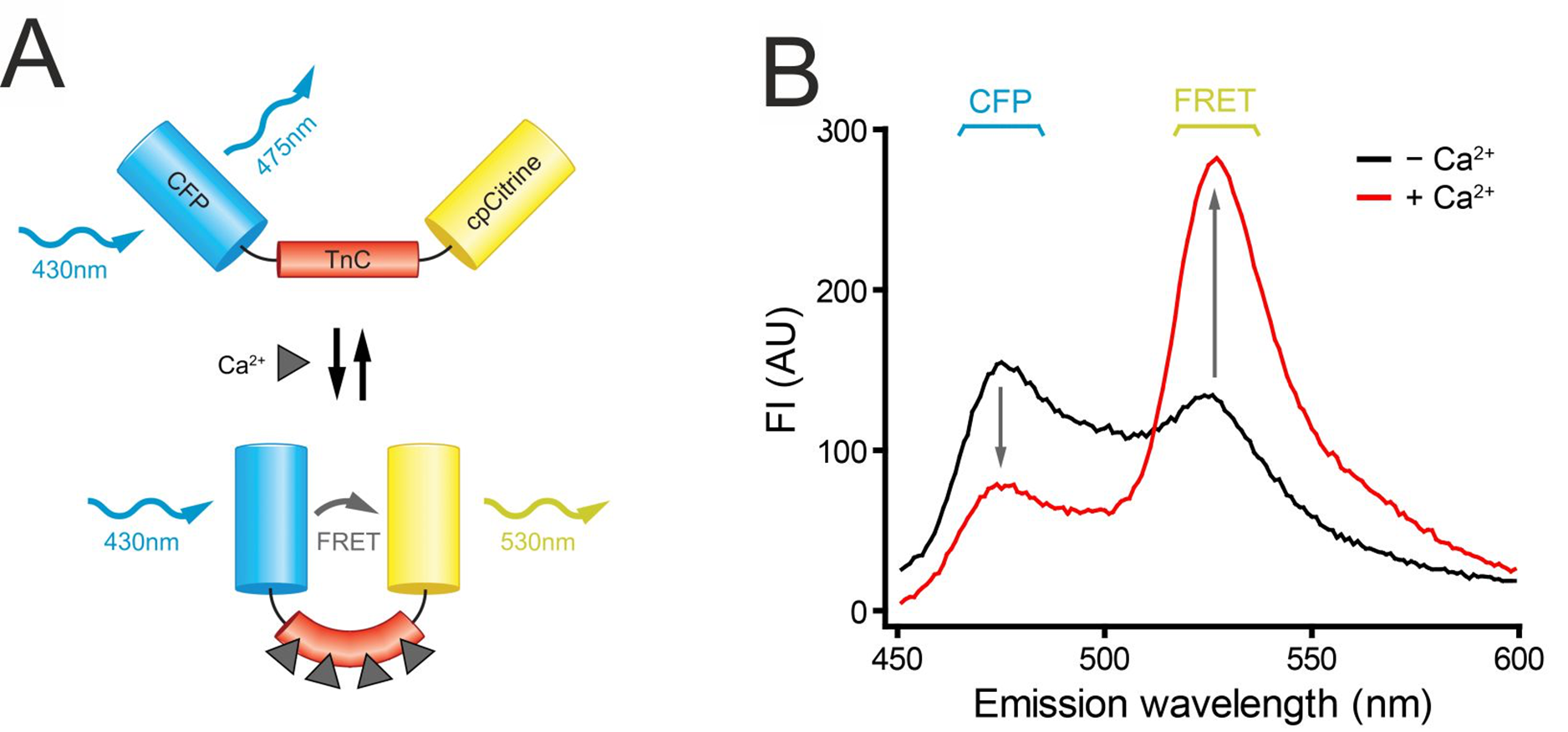
Calcium concentration changes are studied using fluorescence reporters and their spectral overlap eg CFP (cyan fluorescent protein). Genetically encoded Ca indicators are made which express proteins in cells and are used to monitor Ca by calibrating to measure exact concentration. FRET (fluorescence energy transfer) only occurs when the two fluorophores are close together, shown as an overlap between donor emission and acceptor excitation.
FRET and tropomyosin: when calcium levels increase, tropomyosin bends causing FRET. This is shown by decreased emission from CFP and increased cpCitrine emission.