Midterm
Structure of the periodontium (attachment apparatus) and location
trigeminal nerve
tissue surrounding teeth and attaches to the jawbone
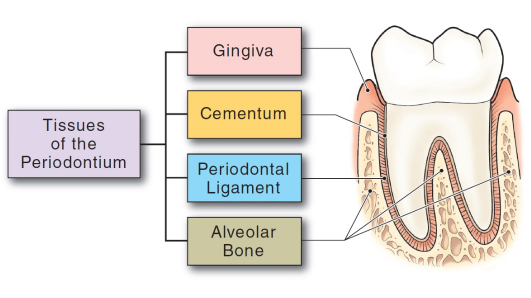
gingiva, cementum, PDL, and alveolar bone
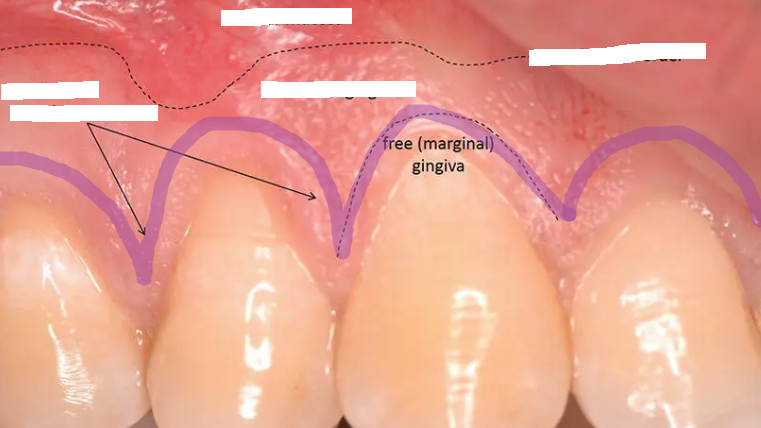
gingiva: tissue that covers the cervical portion of the teeth and alveolar processes
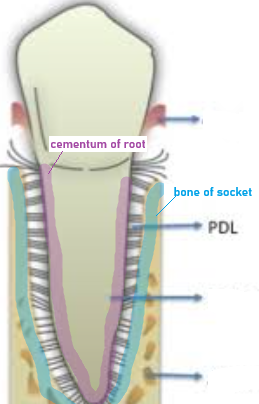
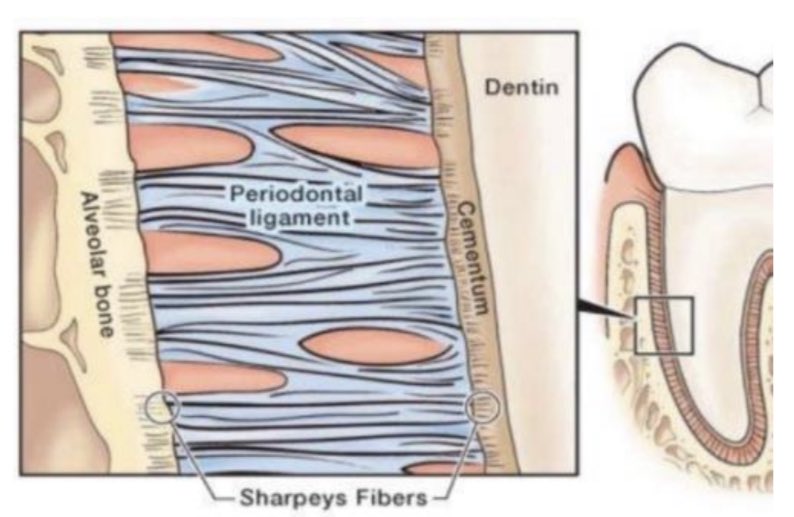
cementum: a thin layer of mineralized tissue that covers the root of the tooth
PDL: fibers that surround the tooth; attach to the socket on one side and the cementum of the root on the other side
Alveolar bone: bone that surrounds the root of the tooth, forms pockets that support the roots
Function of PDL
suspends and maintains the tooth in the socket
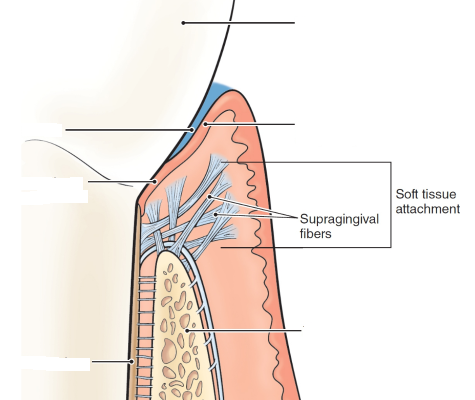
Function of gingival fibers (supragingival fibers)
network of rope-like collagen fiber bundles in the gingival connective tissue.
Located coronal to the crest of the alveolar bone and form soft tissue
Anatomical areas of the gingiva are missing when you see open spaces apical to the contact areas
interdental gingiva
periodontal health
Two types:
clinical gingival health on intact periodontium
clinical gingival health on a reduced periodontium
absence of bleeding on probing, erythema, edema, attachment loss, and alveolar bone loss

gingivitis
Definition: Inflammatory response resulting from the biofilm accumulation located below the gingival margin
two types: dental biofilm-induced or non-dental biofilm-induced
dental biofilm-induced gingivitis:
dental biofilm alone
mediated by systemic or local risk factors
drug-influenced gingival enlargement
Non-dental biofilm-induced gingival disease
genetic/developmental disorders
specific infections
inflammatory and immune conditions
reactive processes
neoplasm
endocrine, nutritional, and metabolic disease
traumatic lesions
gingival pigmentation
gingival health: <10%, localized gingivitis: 10%-30%, and generalized gingivitis: >30%
JE at CEJ; 3mm or greater; reversible

Periodontitis
results in progressive irreversible destruction of the periodontal ligament and supporting alveolar bone
JE on cementum; >4mm of pocket depth
characterization: apical migration of JE, loss of connective tissue attachment, and loss of alveolar bone

Staple Periodontitis
periodontal health on the periodontium with pre-existing loss of connective tissue and alveolar bone that is attributed to periodontitis but that has been successfully treated and is currently stable.

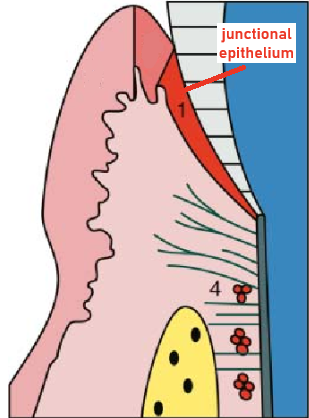
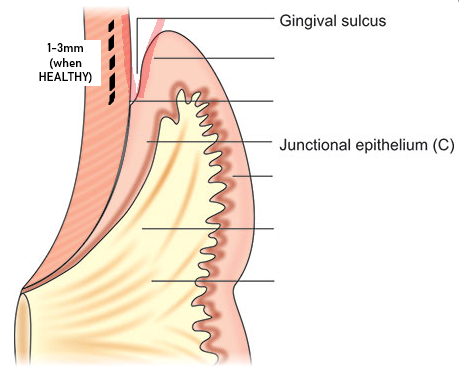
Junctional epithelium
specialized epithelium that forms the base of the sulcus and joins the gingiva to the tooth surface
functions: attachment, barrier, and host defense
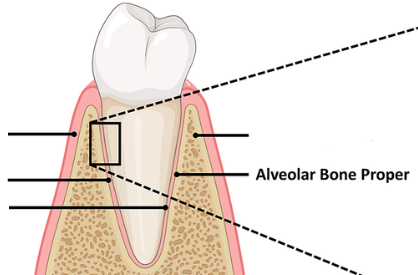
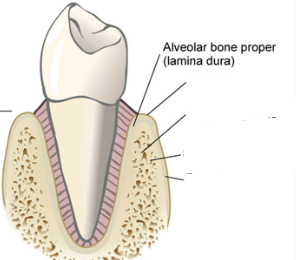
Alveolar bone proper/cribriform plate/lamina dura
A radiopaque layer of bone that lines the alveolar socket
Structures to know:
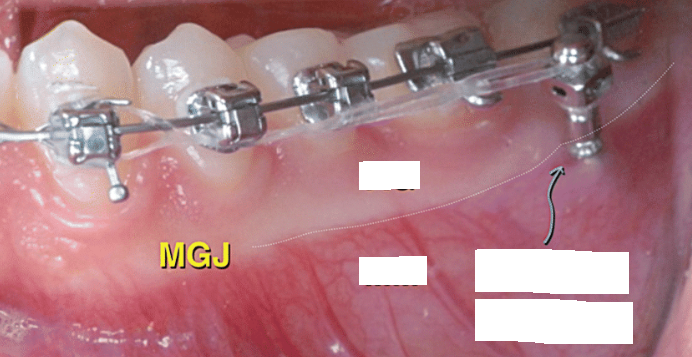
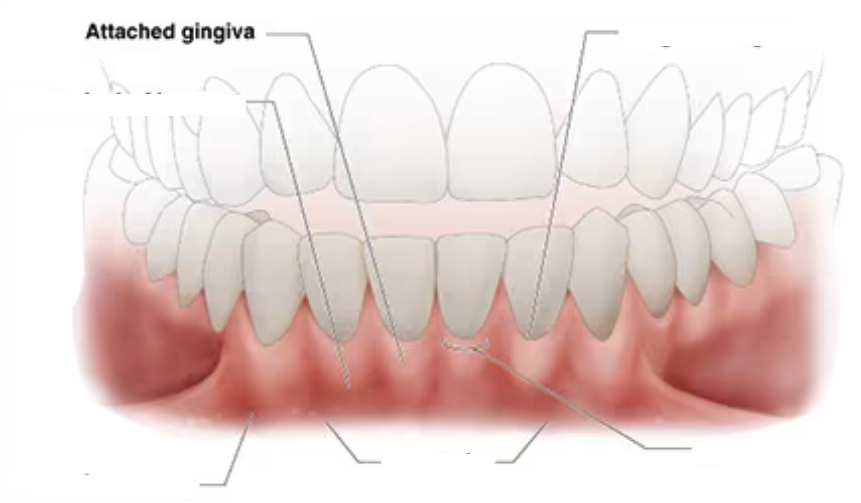
mucogingival junction
clinically visible boundary where the pink attached gingiva meets the red, shiny alveolar mucosa
clinically visible (demarcations)
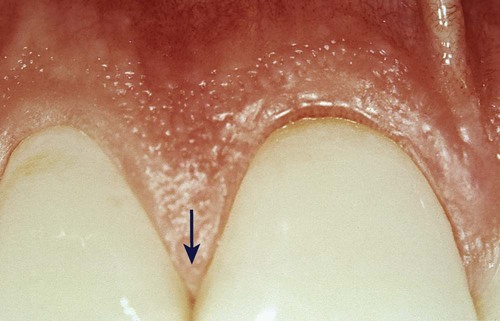
free gingival groove
A shallow linear depression that separates free and attached gingiva
rarely visible to the naked eye (demarcations)
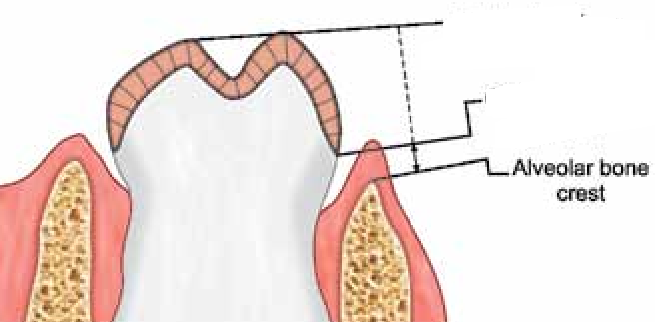
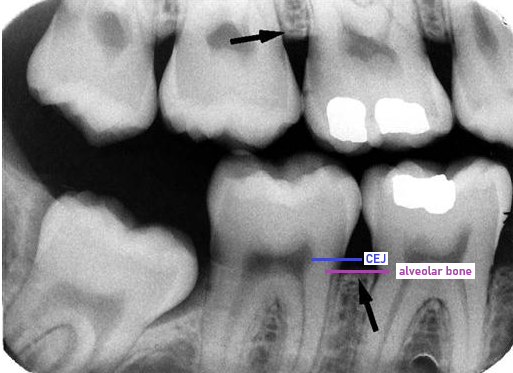
alveolar crest
coronal-most portion of the alveolar process
in health, located 1 to 2 mm apical to CEJ
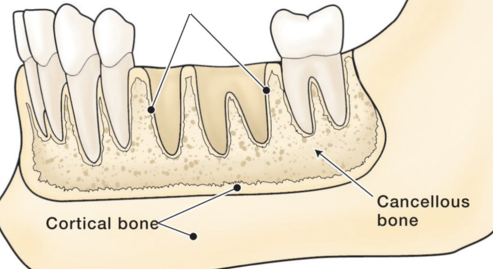
spongy and compact bone
Compact (cortical) bone forms the hard outer wall of the mandible and maxilla; it surrounds the alveolar bone proper
Cancellous (spongy) bone fills the inner portion of the alveolar process (between cortical bone and alveolar bone proper)
alveolar bone proper (cribriform plate)
thin layer of bone that lines the socket and surrounds the root
has foramina that allow blood vessels from cancellous bone to connect with the vessels of the PDL space
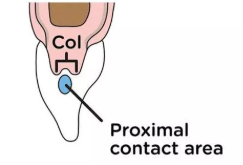
interdental col
valley-like depression in the portion of the interdental gingiva that lies directly apical to the contact area of 2 adjacent teeth and contacts the facial and lingual papillae
absent if adjacent teeth are not in contact
attached gingiva (where is it thinnest?)
continuous with the free gingiva is tightly bound to cementum on the cervical-third of the root and periosteum of the alveolar bone
lies between the free gingiva and the alveolar mucosa
thinnest in the premolar region
desmosomes
create cell-to-cell connections
found in the gingival epithelium
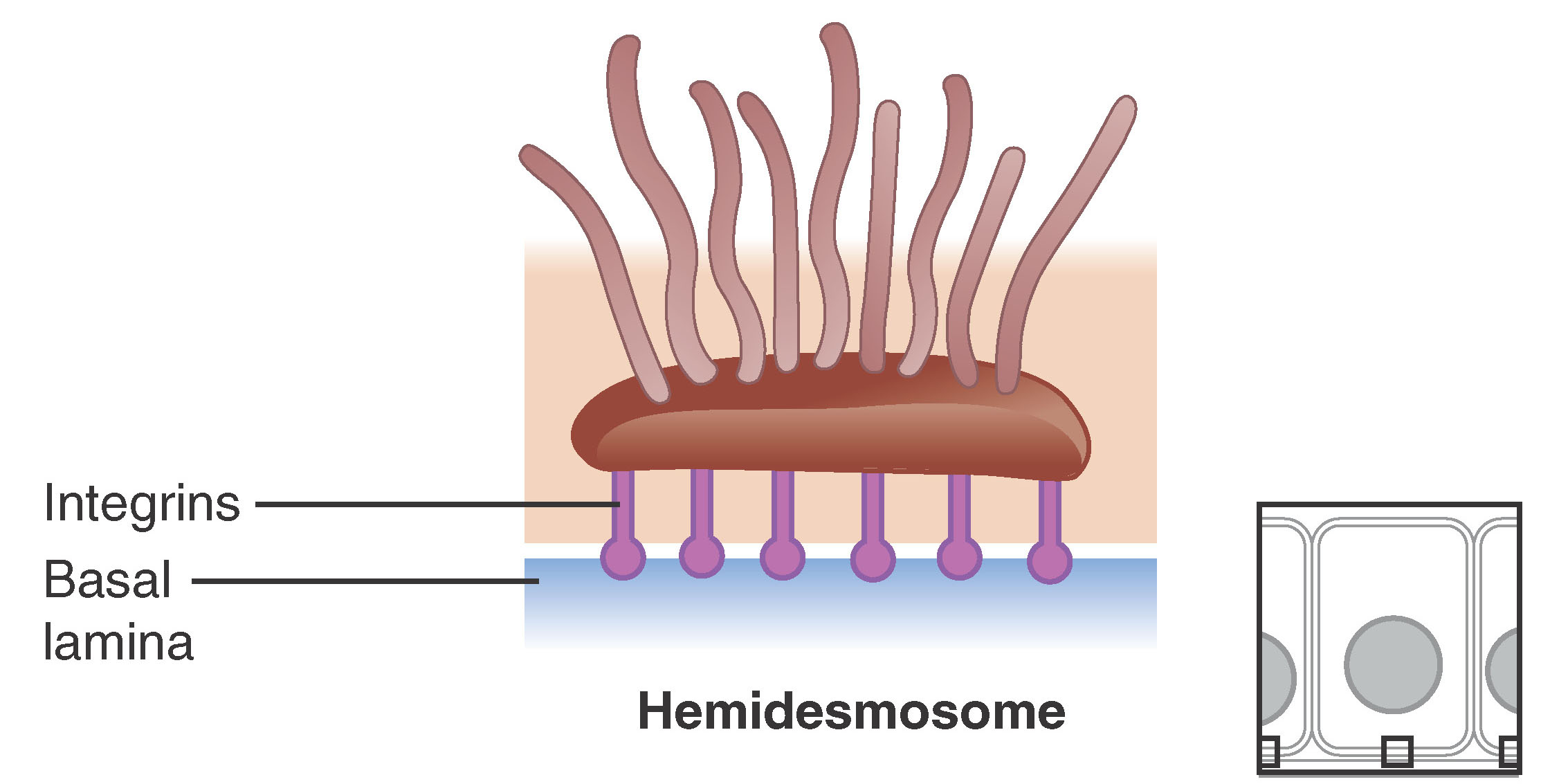
hemi-desmosome
create cell-to-basal lamina connection
found in the gingival epithelium
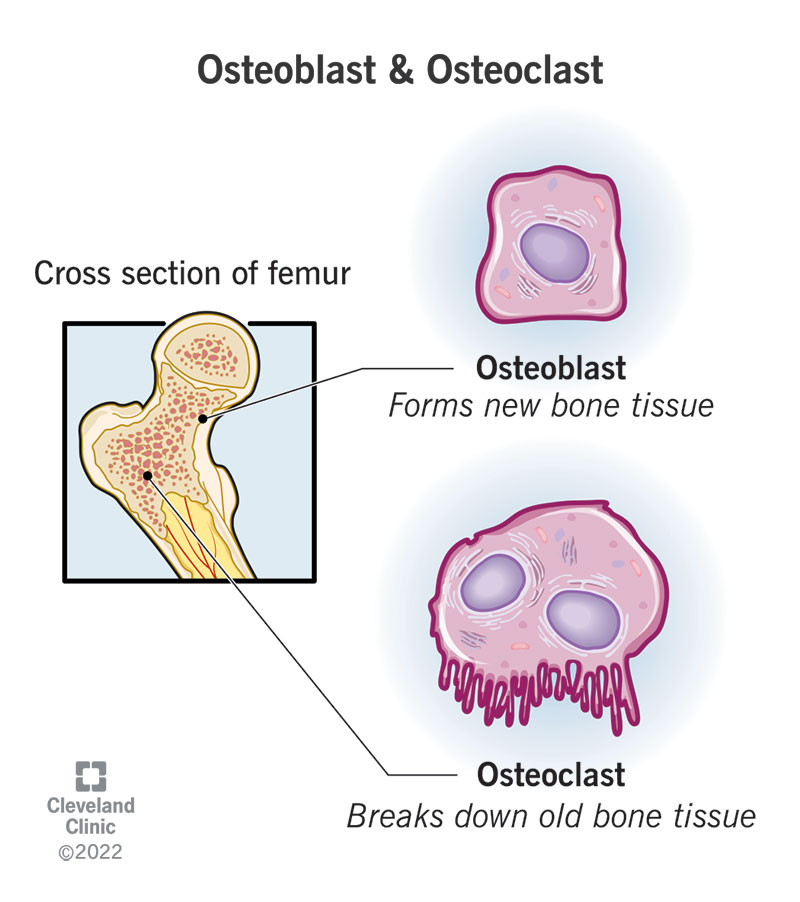
osteoblast
bone-formers that produce the bone matrix consisting of collagen fibers and protein fibers
osteoclasts
bone consumers; cells that remove the minerals and organic matrix of the alveolar bone
Sharpey’s fibers
Calcified terminal ends of PDL embedded in cementum and alveolar bone
attach when cementum and bone are forming
pathogenesis
sequence of the events that occur during the development of a disease or abnormal condition

anastomosis
vessels of the periodontium join together to supply blood
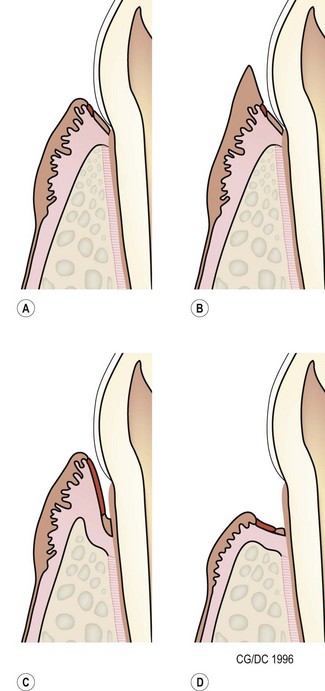
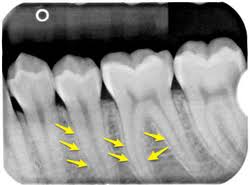
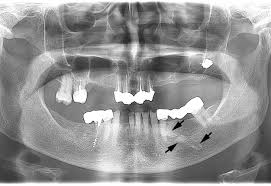
horizontal bone loss
most common in periodontitis
fairly even reduction in the height of the alveolar bone

vertical bone loss (angular bone loss)
less common
uneven reduction in the height of the alveolar bone

infrabony pockets
occurs when vertical bone loss is present
classified into infra-bony defects or osseous defects
JE is located apical to the crest of the alveolar bone
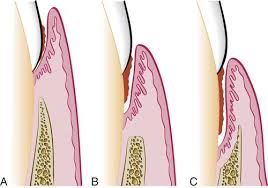
suprabony pockets
occurs when horizontal bone loss is present
base of the periodontal pocket is coronal to the alveolar crest
JE is located coronal to the crest of the alveolar bone
gingival pocket (pseudo-pockets)
deepening of the gingival sulcus as a result of swelling or enlargement of the gingival tissue
caused by: detachment of the coronal portion of JE and/or increased tissue size due to swelling
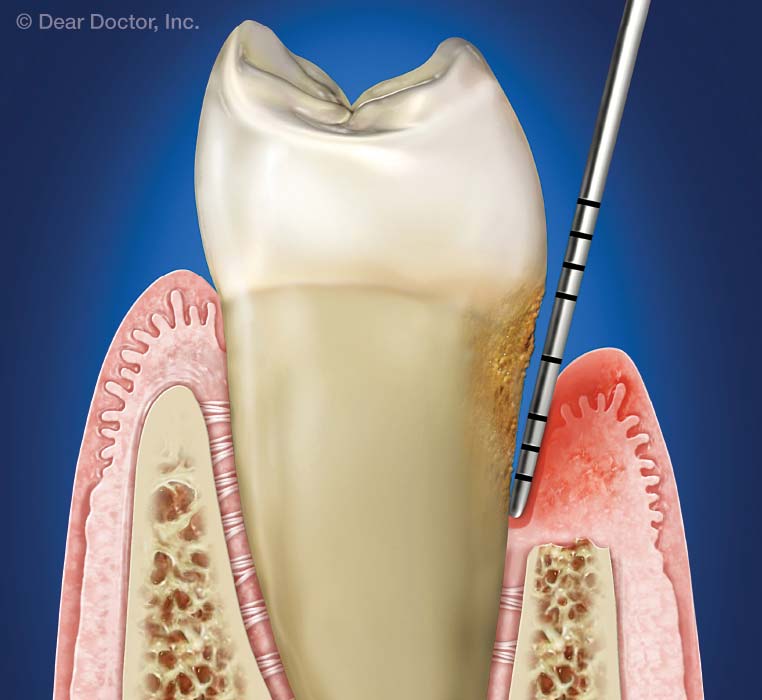
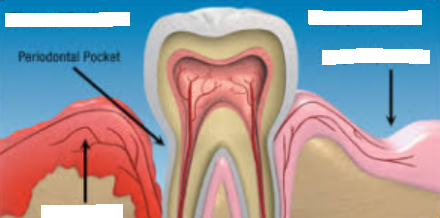
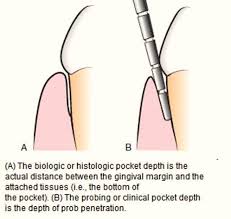
periodontal pocket
pathologic deepening of the gingival sulcus
results from either apical migration of the JE, destruction of the periodontal ligament fibers, or destruction of the alveolar bone
pseudo-pocket
no apical migration of the JE, coronal portion of the JE detaches from the tooth that results in increase probing depth
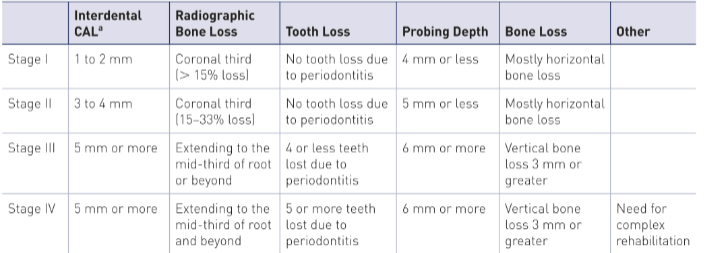
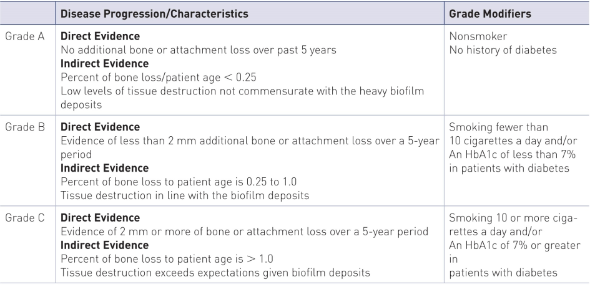
staging (severity) and grading (speed)
grade A: 1/3
grade B: 2/3 (most common)
grade C: 1/3
marginal gingivitis vs diffuse gingivitis
marginal gingivitis → affect gingival margin and papilla

diffuse gingivitis → extend to include the gingival margin, papilla, and attached gingiva

refractory vs recurrent periodontitis
refractory periodontitis
exhibits continuing attachment loss despite receiving periodontal therapy, self-care, and maintenance visits

recurrent periodontitis
return of destructive periodontitis that had been previously arrested by therapy; common

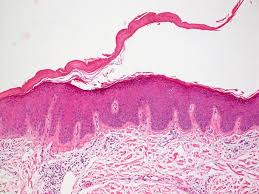
keratinization
process by which surface epithelial cells become stronger and waterproof
keratinized epithelial cells
no nuclei
form a tough, resistant layer on skin
nonkeratinized epithelial cells
nuclei
acts as a cushion
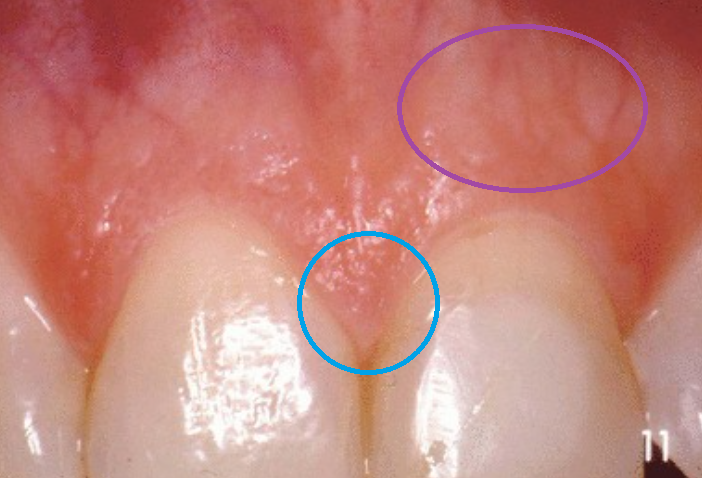
stippling
on the attached and interdental gingiva
present in 40% of pts with healthy gingiva
pyogenic granuloma
noncancerous, raised tumor in your skin or mucous membrane
associated with pregnancy-associated gingivitis

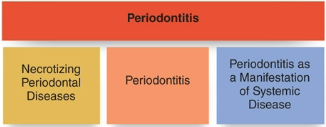
3 major forms of periodontitis in the current AAP Classifications
necrotizing periodontal disease
periodontitis
periodontitis as a manifestation of systemic disease
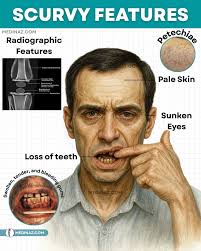
Vitamin C
also Ascorbic Acid; deficiencies cause ascorbic-acid-deficiency-gingivitis and scurvy
warning signs of periodontitis
accumulation of plaque biofilm and calculus
redness (erythema) and swelling (edema)
gingival bleeding
suppuration (pus)
periodontal pockets
clinical attachment loss and tooth mobility

common mucogingival deformity
gingival recession

What % of patients over 65 have at least one area of gingival recession
88%

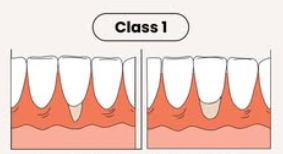
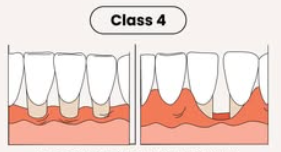
Miller gingival recession classification
Class I
marginal tissue that does not extend to MGJ
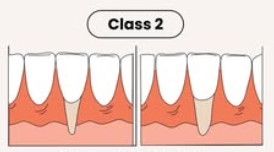
Class II
marginal tissue recession that extends to or beyond MGJ with no periodontal loss in the interdental area
Class III
marginal tissue recession that extends to or beyond MGJ with interdental bone or soft-tissue loss and/or mal-the positioning of teeth

Class IV
marginal tissue recession that extends beyond MGJ with severe loss of interdental bone to level corresponding to most apical extent of marginal tissue recession
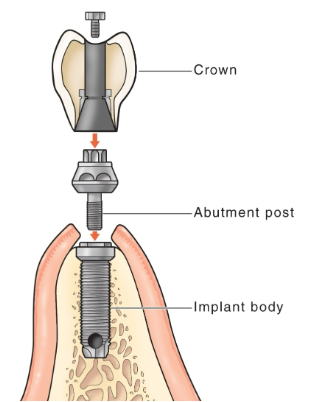
Parts of an implant
implant body (implant fixture)
made of titanium (zirconia as an alternative) or a titanium alloy
acts as “root.”
abutment
connects the prosthesis to the implant body
titanium or zirconia
prosthetic crown or prosthesis
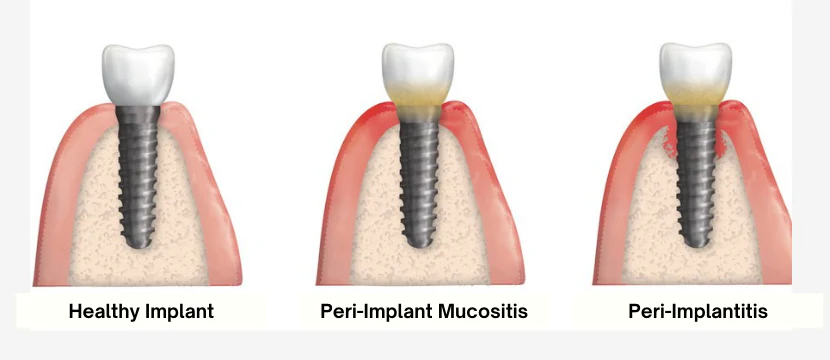
Diagnosis choices: peri-implant health, peri-implant mucositis, peri-implant gingivitis, and peri-implantitis
peri-implant health
absence of erythema, bleeding on probing, swelling, and suppuration
probing depths may be deeper at the site
peri-implant mucositis
visual signs of soft-tissue inflammation, presence of bleeding and/or suppuration upon probing, increased probing depth, absence of bone loss
peri-implant gingivitis
plaque biofilm-induced inflammation of soft tissue with no loss of supporting bone localized in mucosal tissues surrounding dental implant
peri-implantitis
plaque biofilm-induced inflammation and progressive loss of alveolar bone
inflammation, bleeding and/or suppuration upon probing, increased probing depth, progressive bone loss, radiographic evidence of bone level >3mm, and/or probing depth >6mm
uses of dental implants
replaces individual teeth or multiple teeth by supporting fixed bridges or removable dentures
indicator of implant failure → mobility

How often should radiographs be taken of dental implants
At least once a year

Radiopaque or Radiolucent
PDL
radiolucent

lamina dura
radiopaque
alveolar bone proper
radiopaque

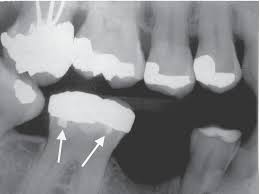
amalgam restorations
radiopaque
marrow spaces in spongy (cancellous bones)
radiolucent

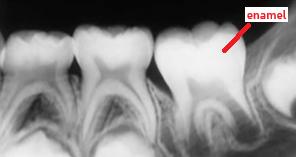
enamel
radiopaque
cementum
radiopaque
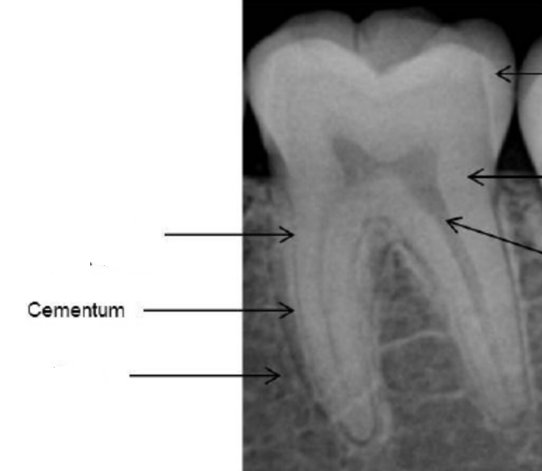
dentin
radiopaque

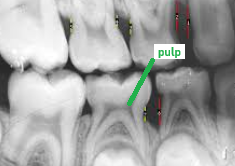
pulp
radiolucent
periapical lesions
radiolucent

sialoliths
radiopaque
normal probing depths
1–3 mm deep when healthy
The height of the Alveolar Crest is in health
1-2mm apical to CEJ
Does epithelium have its own blood supply?
NO
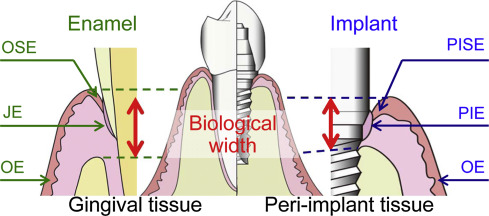
WHY there’s 1-2mm between CEJ and alveolar bone; 1-2mm represents supra-crestal tissue attachment (STA) or biologic width, and supra-crestal attached tissue (SAT)