2. Non-Automated Visual Field Techniques
non-automated instruments
Non-automated screening methods for visual field defects form part of routine eye examinations.
Screening protocols reduce testing time substantially, typically to a few minutes, making visual field testing a viable option for screening for disease.
Common non-automated screening visual field techniques include:
Confrontation
Amsler Grid
Bjerrum/Tangent Screen.
Confrontation
Sensitive only to gross, dense visual field losses
provides a preliminary indication of visual field loss.
Confrontation should be performed monocularly on all patients.
Spectacle correction: test is usually uncorrected so central and peripheral testing occur together; if the patient has high refractive error, correct for central testing and remove correction for peripheral testing.
Procedures
Record visual fields as seen from the patient’s perspective, not how it appears to you.
Label the eye tested (RE or LE) and clearly mark nasal and temporal directions to ensure the record is unambiguous.
Targets should be presented against an appropriate background so that they are readily detectable by normal observers.
Ideally, the examiner should have their back against an evenly illuminated wall free from distracting objects or potential glare sources (lamps, windows).
Communication and patient interaction
Clearly explain procedures to patients.
Typical wording cues: the examiner will describe peripheral vision tests in simple terms and ask for a specific response.
“I’m just going to examine your peripheral / side vision with a couple of simple tests”
Example approach: tell the patient you will examine the peripheral/side vision with simple tests, then give direct prompts to elicit the desired responses (eg, look at the examiner's nose and watch for finger movements).
Avoid vague questions; use precise prompts to elicit the expected answers.
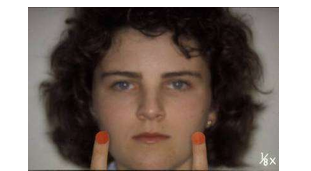
Facial Amsler (Confrontation sub-method)
Facial Amsler uses facial features as landmarks to determine central versus quadrant defects.
Facial Amsler: Procedures
One eye occluded; patient fixates on the examiner's nose.
Ask the patient whether the examiner's other facial features appear distorted or missing (eg, eyes, ears, mouth).
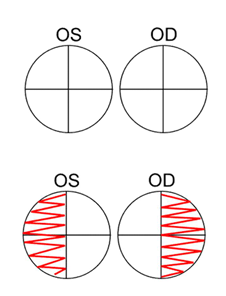
Interpretation:
Nose distortion = central scotoma.
Distortion of other facial features indicates absolute or relative scotoma.
Record the field from the patient’s perspective:
RE Facial Amsler: NAD
RE Facial Amsler: Central distortion.
Confrontation - Finger Counting Fields (FCF)
Occlude one eye; patient fixes on the open eye.
Hold up 1 or 2 fingers in the top two quadrants, straddling the vertical and horizontal midlines.
Ask for the total number of fingers seen; repeat for the bottom two quadrants.
Number of questions: four (two per eye, top and bottom quadrants) to screen both eyes (Anderson et al 2009).
Rationale: testing each quadrant individually can miss extinction, a phenomenon where a target is not seen in the affected hemisphere when two targets are presented simultaneously.
Extinction is a form of hemi-spatial neglect that often arises after stroke or brain injury.

Quick reference: sufficient responses
A rapid finger-counting confrontation screening uses four responses from the patient; examples include combinations in which the correct responses are two, three or four, and never one.
Confrontation: Colour Comparison
Red desaturation can be an early indicator of neurological visual field defects.
Procedure: place two red targets in two quadrants that straddle the vertical and horizontal midlines; ask if there are any noticeable colour differences in redness.
Subtle colour defects involving perception may be revealed by changes in saturation and hue.
Static and Kinetic Finger Movement (Confrontation procedures)
Static Finger Movement: examiner uses finger movement in each quadrant; patient indicates which side movement occurs (one side or both).
Kinetic Finger Movement: examiner uses finger movement or a large Traquair target to assess peripheral extent of the field along eight cardinal directions
patient reports when the finger/target is detected
an isopter is created for a single target.
Kinetic Finger Movement: Procedure details
Setup: examiner and patient sit facing each other at the same eye level, about 1 m apart; both cover one opposing eye with their palm.
Movement: wiggle fingers from the periphery in a plane equidistant between the two faces; move the target at a constant rate.
The patient indicates when the target is first seen; the location is compared to the examiner’s visual field.
Things to remember:
The temporal field is often greater than 90 degrees, so it may not be possible to reach the far limit of the patient’s field.
Facial contours (prominence of the nose, recession of the eyes, brow prominence) may affect the visual field.
Consider whether the visual field loss is anatomical or pathological.
Confrontation - Recording and documentation
Always record what you do and the results:
Facial Amsler: Normal
Finger Count: 4 quadrants normal
Colour Comparison: Colour loss noticed in RE right upper field
Peripheral Fingers: RE and LE normal in 8 directions
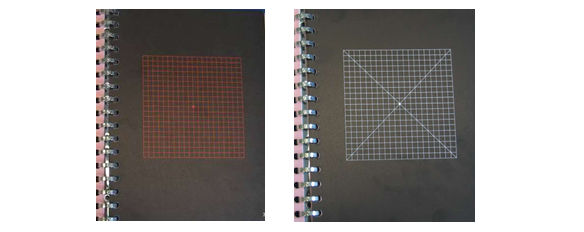
Amsler Chart
A qualitative test of the central visual field (~10°).
Detecting central and paracentral scotomas, as well as areas of distorted vision
Assessment of patients with ocular diseases where scotomas or distortion exist close to fixation, eg. macular degeneration
Advantages: rapid, easy, portable; suitable for home visits and self-monitoring.

Amsler Chart: Procedures
Standard chart: grid of white lines on a black background; held at a working distance of 30 cm from the patient; at this distance the chart extends to about 10° from fixation.
Each 5 mm square subtends a visual angle of 1° at 30 cm.
Correction: an appropriate lens is required for the working distance, particularly for presbyopes
patient’s own reading spectacles may be suitable only if single-vision
if px wears multifocals or bifocals use a trial frame.
Procedure: view the chart with one eye while fixating the central spot
indicate any areas where lines are missing or distorted (metamorphopsia).
Recording: defects should be recorded on the chart
it is often useful for patients to note deficits themselves.
Patient instructions
"We are now testing the central vision of your right eye. Look at the centre dot, but be aware of the background at all times.“
“Can you see the central dot?”
“Can you see all 4 corners of the card? How about all 4 sides?”
“Are all the lines straight and even?”
“Are any of the squares missing?”
“Are any of the lines wavy or distorted?"
Amsler variations
Red printed charts have been proposed to aid detection of toxic retinal conditions.
Some charts include diagonal lines through the center to assist fixation for patients with central scotomas.
Amsler recent research interest
There is increased clinical and research interest in central field assessment for detecting ocular disease.
Screening for wet AMD prior to anti-VEGF treatment: systematic review (mostly case control studies)
Values from 12 studies: sensitivity and specificity of 78% and 97%
Highlighted the importance of correct instruction and monitoring
In glaucoma, a study of 106 eyes (53 patients) showed that Amsler grid detected moderate to severe central glaucomatous loss
Compared Amsler results with 10-2 VF (HFA)
Sensitivity and specificity of 68% and 92%
Useful where more sophisticated VF tests are unavailable
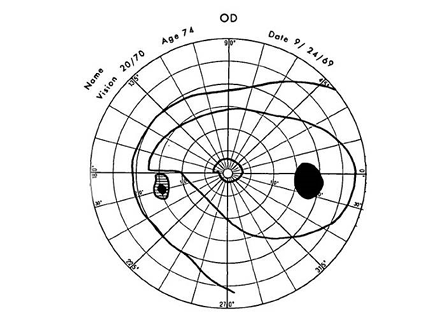
Bjerrum/Tangent Screen
The Bjerrum screen (also known as the Tangent Screen) measures the central 30deg at 1 metre.
Uses Kinetic strategy
Technique requires skilled and experienced examiners.
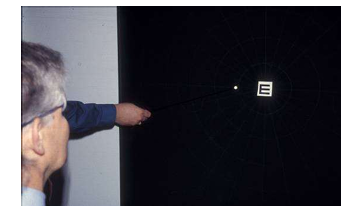
Bjerrum/Tangent Screen: Procedures
Screen is a black felt surface with eccentricities, meridians, and blind spots stitched onto it
screen illuminance of 10 lux
Targets consist of painted discs or beads moved at 5 deg/s (usually from non-seeing to seeing)

Plotting and recording
Plot blind spots first using a 5/1000W target in the eight cardinal directions.
Plot isopters using a 2/1000W moving target from the periphery inward until seen; continue inward to fixation.
If the target disappears, this indicates a scotoma.
Smaller or coloured targets may be used to plot additional scotomas.
Black map pins are used to record the visual field on the screen and then transposed to printed charts.
For reduced distraction, the examiner should wear a black sleeve or dark clothing.
Isopter notation
Isopters are described as A/BC, for example 1/2000W.
A = target size (mm); B = test distance (mm); C = colour of the target.
Non-Automated Visual Field Techniques: General Considerations
These qualitative non-automated tests are influenced by the following factors:
Type, size, colour, and brightness of the target used.
Distance at which the test is carried out.
Speed of target movement.
Background against which the test is performed.
These tests are crude screening tools; if there is any indication of an abnormal field, an automated field test should be performed for more objective assessment.