ABDOMINAL WALL EXAM 2
Anterior Abdominal Wall
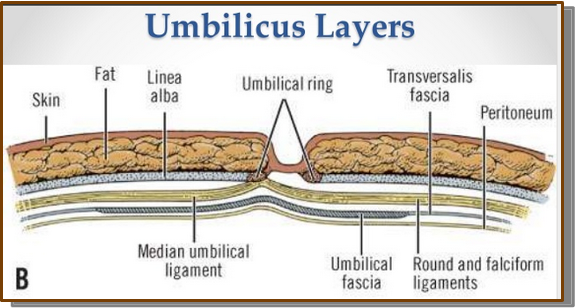
Describe the umbilical ring/folds and its structure
Umbilical Ring:
A natural opening in the linea alba where the umbilical cord once entered.
The umbilical ring is a natural opening in the linea alba that allows the umbilical cord to pass during fetal life; after birth it closes to form the umbilicus, but in portal hypertension the umbilical vein may reopen, causing caput medusae.
"Ring → Cord → Scar."
Ring = Opening
Cord = Passes through before birth
Scar = Belly button after birth
Describe the structure of the superficial layers of the abdominal wall:
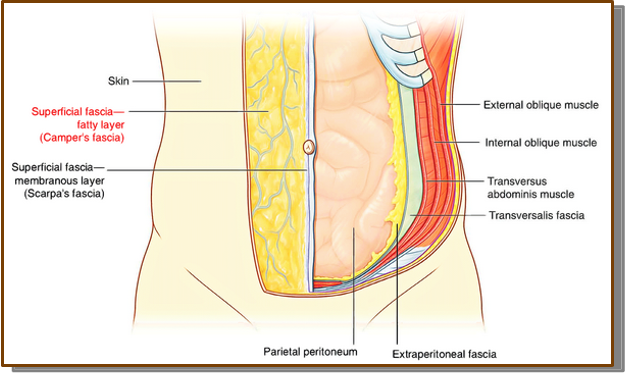
—Camper’s fascia-
fatty superficial layer (most superficial layer)
Camper's fascia is the most superficial, fatty layer of the anterior abdominal wall that provides cushioning, stores fat, and forms the pannus.
—Scarpa’s fascia
Scarpa's fascia is the deep, dense fibrous layer of the superficial fascia that provides structural support to the abdominal wall and is important for surgical closure, wound healing, and limiting the spread of fluid.
—Colles’ fascia
Colles' fascia is the strong membranous continuation of Scarpa's fascia into the perineum, where it supports superficial tissues
"CSC = Cushion → Support → Continue"
Camper's = Cushion (fat)
Scarpa's = Support (dense fibrous layer)
Colles' = Continue (Scarpa's continues into the perineum)
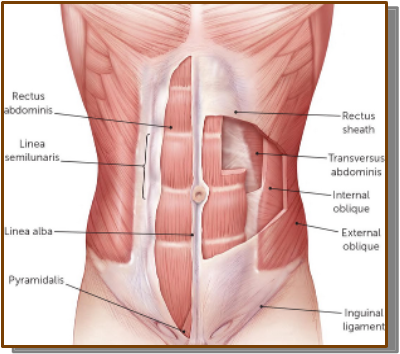
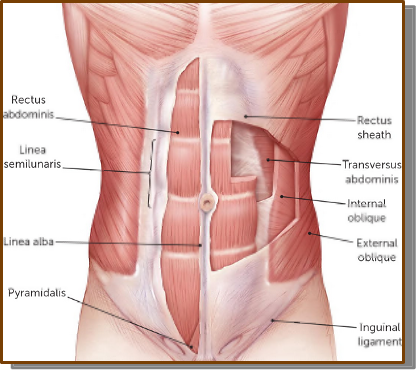
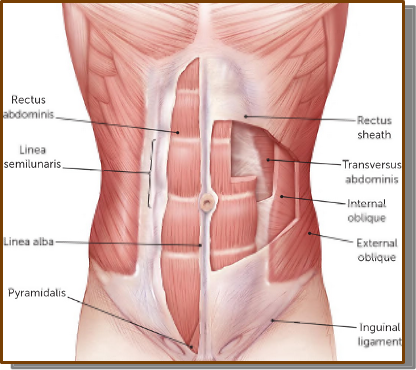
Identify the following abdominal wall muscles, innervation and the corresponding actions:
External oblique: The most superficial
Action:
○Flexion of the trunk - when both sides contract
○Rotation of the trunk to the OTHER side - when one sides contract
■For example, the right external oblique helps rotate the trunk to the left.
○Compression and Structural Support
Both sides contract (bilateral): ➜ Flexes the trunk (bends you forward, like a sit-up)
One side contracts (unilateral): ➜ Rotates the trunk to the opposite side (contralateral rotation)
Right external oblique → rotates trunk left
Left external oblique → rotates trunk right
Compresses the abdominal contents
Supports abdominal organs
Increases intra-abdominal pressure (coughing, sneezing, vomiting, defecation, childbirth)
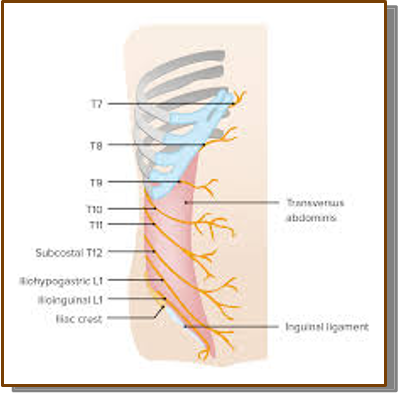
Innervation:
Motor:
Intercostal nerves (T7–T11)
Subcostal nerve (T12)
Sensory:
Iliohypogastric nerve (L1)
"External FOP 7-11 Open 12, Last is L1."
✅ F = Flexes trunk
✅ O = Opposite rotation
✅ P = Pressure (compresses abdomen)
Innervation:
✅ 7–11 = Intercostal nerves
✅ 12 = Subcostal nerve
✅ L1 = Iliohypogastric nerve
Internal oblique: Deep in the external oblique
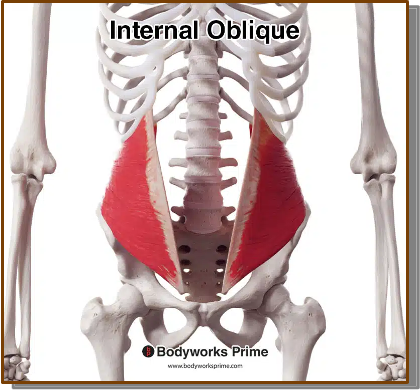
ACTION:
○Flexion and Rotation of the Trunk:
■Flexion of the trunk - when both sides contract
■Rotation of the trunk to the SAME side - when one sides contract
This contrast with the external oblique is a favorite anatomy exam concept:
External = Opposite
Internal = Same
●Right internal oblique helps rotate the trunk to the right.
○Compression and Structural Support
Innervation:
T7–T11 = Intercostal
T12 = Subcostal
L1 = Iliohypogastric
L1 = Ilioinguinal
○Intercostal nerves, subcostal nerve, iliohypogastric nerve, ilioinguinal nerve
Transverse Abdominis: Deepest of the abdominal muscle
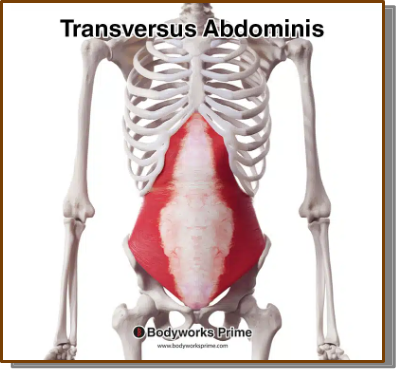
Action:
Compression the abdominal viscera - essential for activities like coughing, sneezing, vomiting, and childbirth.
-The transversus abdominis is the deepest abdominal muscle; it compresses the abdominal contents, increases intra-abdominal pressure, stabilizes the core
Innervation: ○Intercostal nerves, subcostal nerve, iliohypogastric nerve, ilioinguinal nerve.
T7–T11 = Intercostal nerves
T12 = Subcostal nerve
L1 = Iliohypogastric nerve
L1 = Ilioinguinal nerve
Muscle | Main Actions | Innervation | Easy Memory |
|---|---|---|---|
External Oblique (EO) | • Flexes trunk (both sides) • Rotates trunk to the OPPOSITE side (one side) • Compresses abdomen | T7–T11 (Intercostal) T12(Subcostal) | External = Exit to the Opposite |
Internal Oblique (IO) | • Flexes trunk (both sides) • Rotates trunk to the SAME side (one side) • Compresses abdomen | T7–T11 (Intercostal) T12(Subcostal) L1 (Iliohypogastric & Ilioinguinal) | Internal = Stay on the Same Side |
Transversus Abdominis (TA) | • Compresses abdominal contents • Increases intra-abdominal pressure • Stabilizes the core | T7–T11 (Intercostal) T12(Subcostal) L1 (Iliohypogastric & Ilioinguinal) | TA = Tightens the Abdomen |
Muscle | Innervation |
|---|---|
External Oblique | T7–T12 |
Internal Oblique | T7–T12 + L1 |
Transversus Abdominis | T7–T12 + L1 |
Rectus Abdominis: “Six-pack”
Action:
○Primary muscle for Flexion of the Trunk
○Helps flex the lumbar vertebrae, contributing to movements like curling the lower back.
○Compression of Abdominal Viscera.
○Stabilization and Control of Pelvic Tilt
Main muscle used to bend the body forward.
Example: Sit-ups or crunches.
Innervation: ○Intercostal nerves (T7-T11), subcostal nerve (T12)
Pyramidalis:
The pyramidalis is a small, triangular muscle located anterior to the lower part of the rectus abdominis within the rectus sheath.
ACTION:
Tenses the linea alba (tightens the midline tendon of the abdominal wall).
Helps stabilize the lower anterior abdominal wall.
Does not significantly flex the trunk because it is a very small muscle.
INERVATION: Subcostal nerve (T12)
Describe the deep fascial layers:
Transversalis fascia:
a thin fibrous layer of the endoabdominal fascia that lines the deep surface of the transversus abdominis, separates the abdominal muscles from the peritoneum, supports the abdominal wall, and forms the deep inguinal ring.
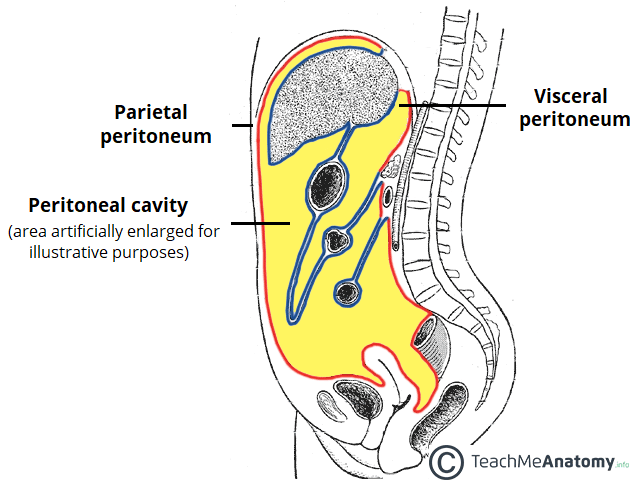
Peritoneum
Parietal (outer) = Wall = Sharp pain
Visceral (inner) = Viscera (organs) = Vague pain
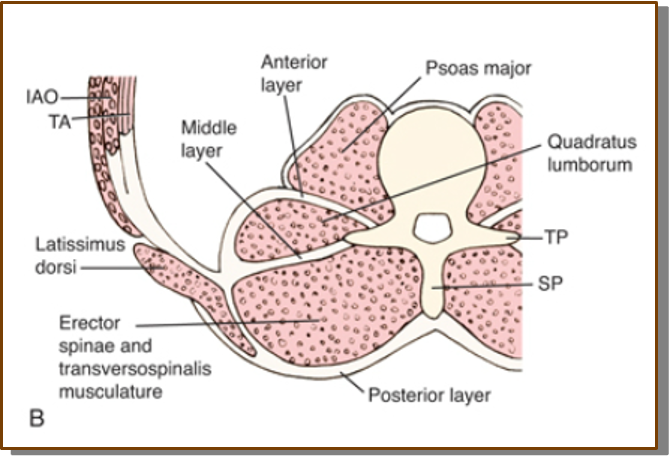
Transversalis Fascia
Thin aponeurotic layer of endoabdominal fascia
Lines the inner surface of the transversus abdominis
Separates muscle from the peritoneum
Feature | Description |
|---|---|
Type | Thin aponeurotic layer of endoabdominal fascia |
Location | Inner surface of transversus abdominis |
Function (from slide) | Separates muscle from the peritoneum |
Parietal peritoneum:
Description
More superficial
Lines the abdominopelvic wall
Innervation
Somatic nerves
Intercostal nerves
Phrenic nerve
Pain Characteristics
The slide describes pain from the parietal peritoneum as:
Sharp
Intense
Well localized
It also carries sensation for:
Pressure
Pain
Heat
Cold
Feature | Parietal Peritoneum |
|---|---|
Location | Lines the abdominopelvic wall |
Innervation | Somatic nerves (intercostals or phrenic nerve) |
Pain | Sharp, intense |
Localization | Well localized |
Sensations | Pressure, pain, heat, cold |
Visceral peritoneum:
Description
Deeper layer
Covers the intraperitoneal organs
Also known as the serosa
Innervation
Autonomic nerves
Pain Characteristics
Pain is described as:
Dull
Crampy
Poorly localized
Clinical Correlation
The PowerPoint explains appendicitis pain:
Initially: dull ache near the belly button (visceral pain)
Later: becomes sharp, stabbing pain in the lower right abdomen once inflammation reaches the parietal peritoneum
Feature | Visceral Peritoneum |
|---|---|
Location | Covers intraperitoneal organs |
Other name | Serosa |
Innervation | Autonomic nerves |
Pain | Dull, crampy |
Localization | Poorly localized |
Identify the vascular supply of the anterior abdominal wall
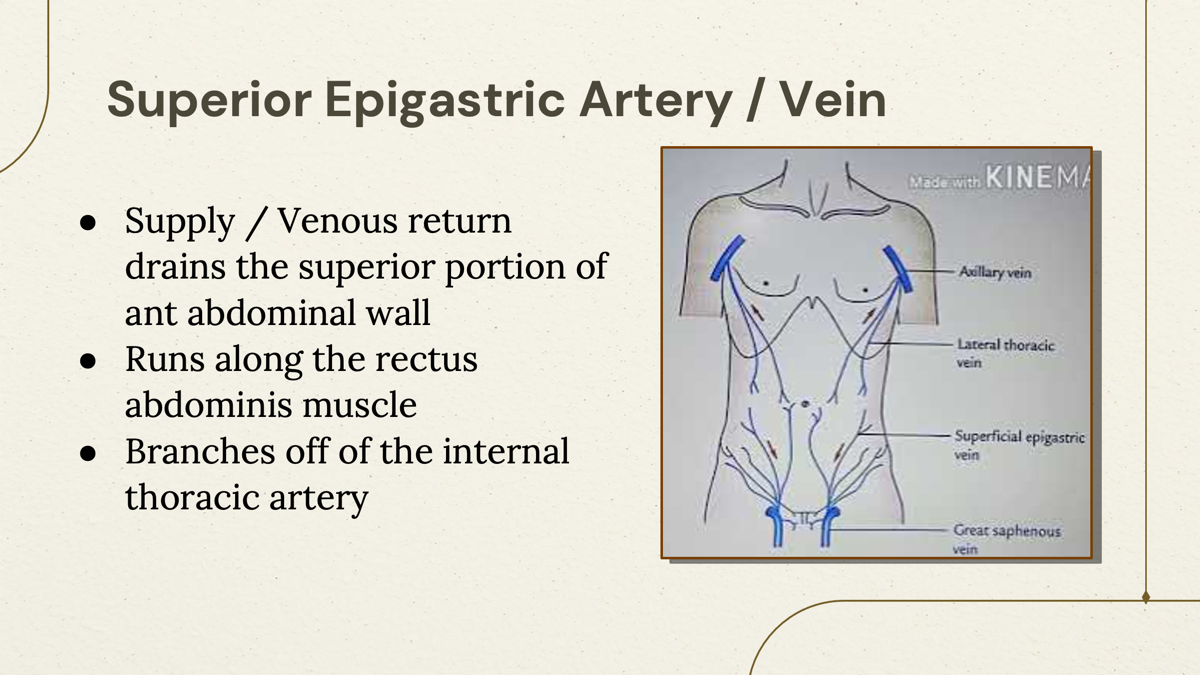
Superior epigastric artery
A. Superior Epigastric Artery
Blood Supply
Supplies the superior portion of the anterior abdominal wall
Venous return drains the superior portion of the anterior abdominal wall
Course
Runs along the rectus abdominis muscle
Origin
Branches off the internal thoracic artery
Feature | Superior Epigastric Artery |
|---|---|
Supplies | Superior portion of the anterior abdominal wall |
Course | Runs along the rectus abdominis muscle |
Origin | Internal thoracic artery |
Inferior epigastric artery:
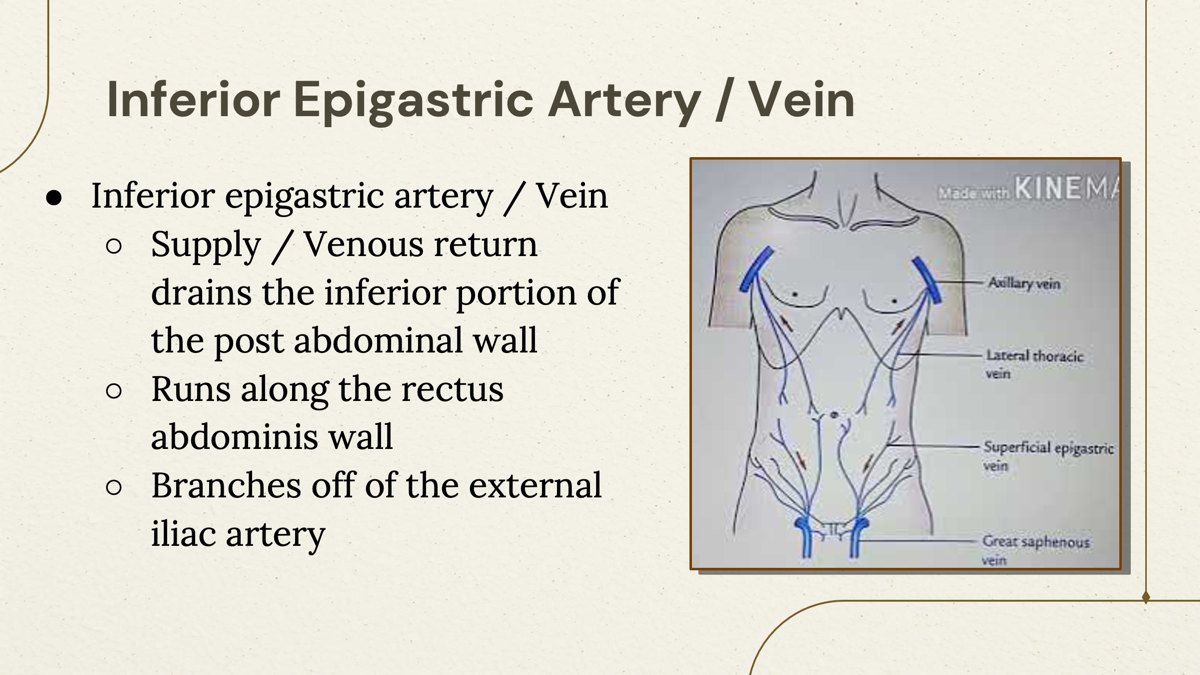
B. Inferior Epigastric Artery
Blood Supply
Supplies the inferior portion of the abdominal wall
Venous return drains the inferior portion of the abdominal wall
Course
Runs along the rectus abdominis muscle
Origin
Branches off the external iliac artery
Feature
Inferior Epigastric Artery
Supplies
Inferior portion of the abdominal wall
Course
Runs along the rectus abdominis muscle
Origin
External iliac artery
Feature | Superior Epigastric Artery | Inferior Epigastric Artery |
|---|---|---|
Supplies | Superior portion of anterior abdominal wall | Inferior portion of abdominal wall |
Runs Along | Rectus abdominis | Rectus abdominis |
Branches From | Internal thoracic artery | External iliac artery |
Identify the location and innervations of the anterior abdominal nerves
Iliohypogastric nerve:

A. Iliohypogastric Nerve
General Information
Listed as one of the anterior abdominal nerves
Covered further in the Posterior Abdominal Wall Lecture
Location
The nerve:
Passes around the iliac crest
Travels between the internal oblique and transversus abdominis muscles
Sensory Innervation
Provides sensory innervation to:
Skin of the upper lateral thigh
Skin over the pubic symphysis
Lower abdomen
Feature | Iliohypogastric Nerve |
|---|---|
Course | Passes around the iliac crest |
Location | Between the internal oblique and transversus abdominis |
Sensory Supply | Upper lateral thigh, pubic symphysis, lower abdomen |
Ilioinguinal nerve:
B. Ilioinguinal Nerve
General Information
Listed as one of the anterior abdominal nerves
Covered further in the Posterior Abdominal Wall Lecture
Location
The nerve:
Follows the same path as the iliohypogastric nerve
Passes through the inguinal canal
Exits through the superficial inguinal ring
Sensory Innervation
Provides sensory innervation to:
Upper medial thigh
Root of the penis and scrotum (males)
Mons pubis and labia majora (females)
Clinical Correlation
The PowerPoint states:
The ilioinguinal nerve may become entrapped following:
Abdominal surgery
Groin surgery
Hernia repair
Laparoscopic surgery
This may result in:
Pain
Tingling
Hypoesthesia in the areas it innervates
Identify the boundaries, structures, and contents of the inguinal canal
Inguinal Canal
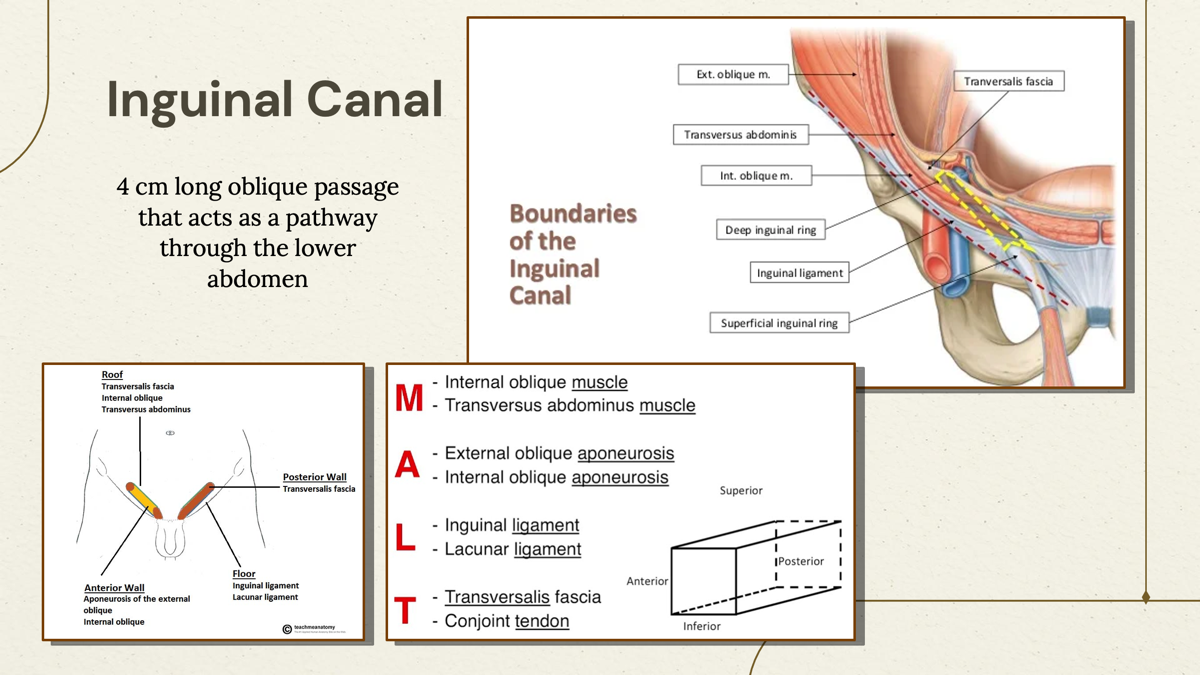
Definition
The inguinal canal is:
A 4 cm long oblique passage
Acts as a pathway through the lower abdomen
Anterior superior iliac spine (pelvis):
1. Anterior Superior Iliac Spine (ASIS)
According to the slides:
The deep inguinal ring is located halfway between the ASIS and the pubic symphysis.
Pubic tubercle (pelvis)
2. Pubic Tubercle
According to the slides:
The superficial inguinal ring is located superior and lateral to the pubic tubercle.
Inguinal ligament:
3. Inguinal Ligament
The inguinal ligament is listed as one of the important anatomical landmarks for the inguinal canal in the objectives. It is also identified as an origin for the internal oblique and transversus abdominis muscles.
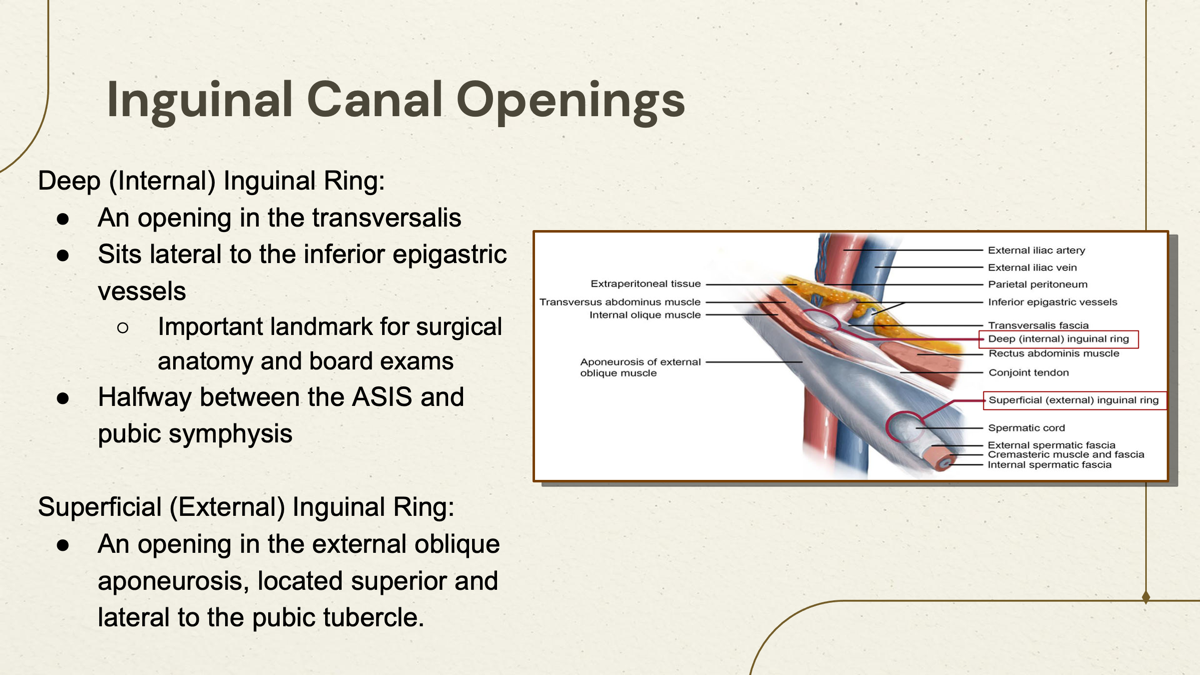
Superficial:
C. Superficial (External) Inguinal Ring
Description
The superficial inguinal ring is:
An opening in the external oblique aponeurosis
Located superior and lateral to the pubic tubercle
Superficial Inguinal Ring |
|---|
Opening in external oblique aponeurosis |
Superior and lateral to the pubic tubercle |
Deep inguinal rings:
B. Deep (Internal) Inguinal Ring
Description
The deep inguinal ring is:
An opening in the transversalis fascia
Located lateral to the inferior epigastric vessels
An important landmark for:
Surgical anatomy
Board examinations
Located halfway between the ASIS and the pubic symphysis
Deep Inguinal Ring |
|---|
Opening in the transversalis fascia |
Lateral to the inferior epigastric vessels |
Halfway between the ASIS and pubic symphysis |
Important surgical landmark |
D. Contents of the Inguinal Canal
According to the PowerPoint, the inguinal canal contains:
Nerves
Ilioinguinal nerve
Genital branch of the genitofemoral nerve
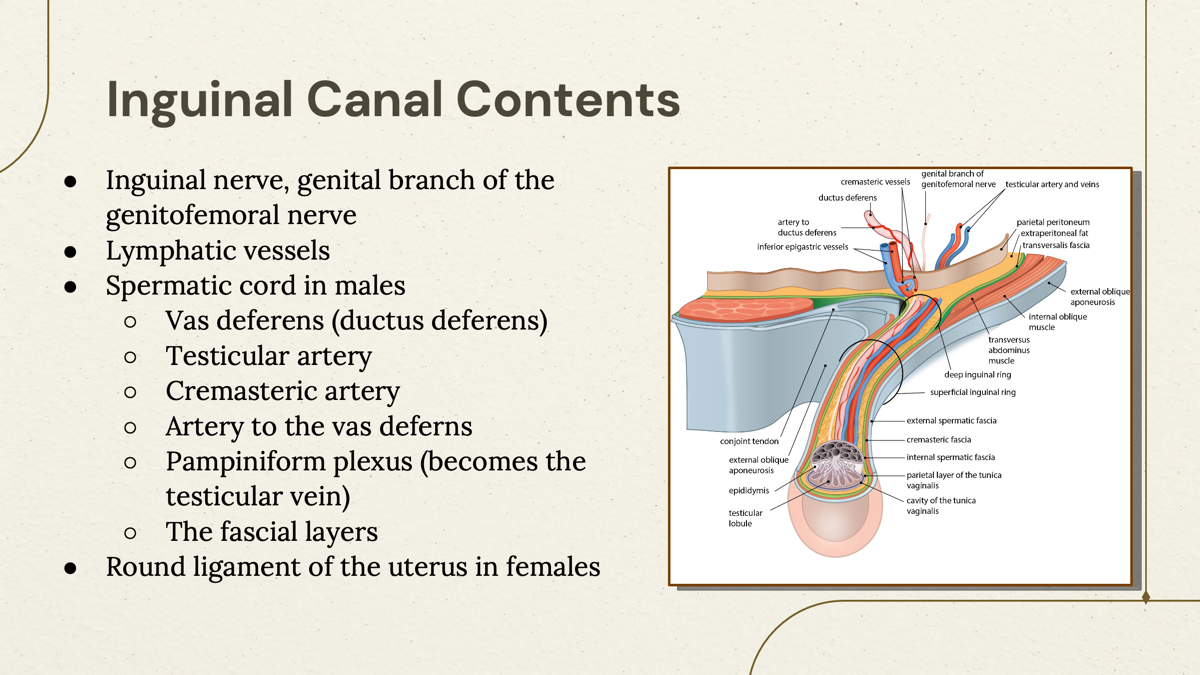
Lymphatics
Lymphatic vessels
Male Contents
Spermatic cord
Vas deferens (ductus deferens)
Testicular artery
Cremasteric artery
Artery to the vas deferens
Pampiniform plexus (becomes the testicular vein)
Fascial layers
Female Contents
Round ligament of the uterus
Contents Summary Table
Present in Canal | Structures |
|---|---|
Nerves | Ilioinguinal nerve, genital branch of genitofemoral nerve |
Lymphatics | Lymphatic vessels |
Male | Spermatic cord, vas deferens, testicular artery, cremasteric artery, artery to vas deferens, pampiniform plexus, fascial layers |
Female | Round ligament of the uterus |
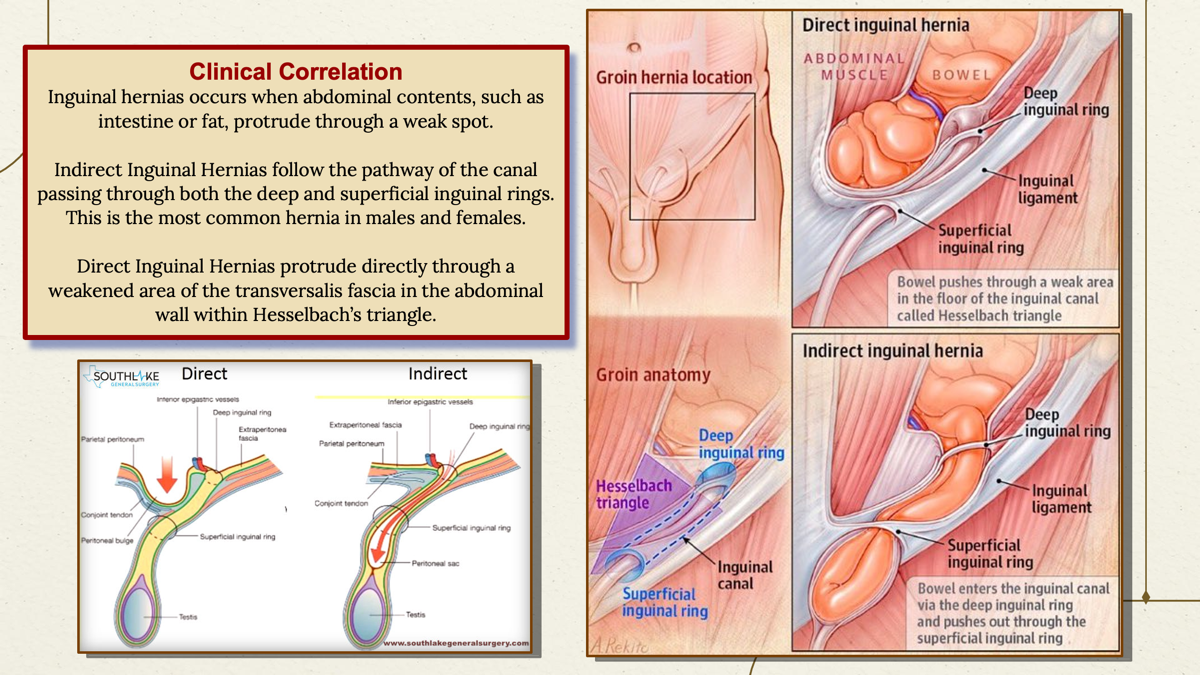
Clinical Correlation
Inguinal Hernias
According to the slides:
An inguinal hernia occurs when:
Abdominal contents (such as intestine or fat)
Protrude through a weak spot in the abdominal wall.
Indirect Inguinal Hernia
The PowerPoint states that an indirect inguinal hernia:
Follows the pathway of the inguinal canal
Passes through:
Deep inguinal ring
Superficial inguinal ring
Is the most common hernia in males and females.
Direct Inguinal Hernia
According to the slides:
Protrudes directly through a weakened area of the transversalis fascia
Occurs within Hesselbach's triangle.
Feature | Deep Inguinal Ring | Superficial Inguinal Ring |
|---|---|---|
Opening in | Transversalis fascia | External oblique aponeurosis |
Location | Lateral to inferior epigastric vessels | Superior and lateral to pubic tubercle |
Landmark | Halfway between ASIS and pubic symphysis | Near pubic tubercle |
Indirect | Direct |
|---|---|
Travels through the inguinal canal | Pushes directly through the abdominal wall |
Passes through both the deep and superficial inguinal rings | Through a weakened area of the transversalis fascia |
Most common hernia in males and females | Occurs within Hesselbach's triangle |
PA School Exam Pearls (From the Slides Only)
The inguinal canal is a 4 cm oblique passage through the lower abdomen.
The deep inguinal ring is an opening in the transversalis fascia, located lateral to the inferior epigastric vesselsand halfway between the ASIS and pubic symphysis.
The superficial inguinal ring is an opening in the external oblique aponeurosis, located superior and lateral to the pubic tubercle.
The inguinal canal contains the ilioinguinal nerve, genital branch of the genitofemoral nerve, lymphatic vessels, the spermatic cord (male), and the round ligament of the uterus (female).
Indirect inguinal hernias pass through both inguinal rings along the canal, while direct inguinal herniasprotrude through a weakened area of the transversalis fascia within Hesselbach's triangle.