9. Motor Cortex and Supraspinal Control
Motor Cortex and Allied Areas
Overview
Previous lecture focused on spinal reflexes controlling muscle length, velocity, and force control.
This lecture focuses on supraspinal control from the motor cortex and associated areas.
Discusses roles of basal ganglia in initiating pre-programmed movements and cerebellum in movement coordination and correction.
Importance of Topic
Automatic and effortless nature of conscious movements (e.g., talking, walking).
Supraspinal structures oversee spinal reflex actions and are crucial for coordinated movement.
Disorders in these systems lead to significant locomotor difficulties.
Hierarchy of Integration – Summary
Neural integration occurs at three levels of sophistication, each associated with different anatomical structures and functions:
🔥 1. Spinal Level (Basic Reflex Integration):
Anatomical Substrate:
The spinal cord is responsible for basic reflex integration (e.g., stretch reflexes).
Function:
Controls simple, automatic movements.
Involves local reflex arcs and spinal circuits.
⚙ 2. Subcortical Level (Intermediate Control):
Pathways Involved:
Vestibulospinal and reticulospinal pathways.
Phylogenetically Old:
These pathways evolved early and control proximal limb musculature.
Function:
Primarily responsible for posture control and basic movement correction.
Cerebellum Involvement:
The medial cerebellum (also known as the spinocerebellum) plays a role in postural adjustments and basic motor coordination.
🎯 3. Cortical Level (Sophisticated Control):
Pathways Involved:
Corticospinal tracts.
Phylogenetically New:
These tracts evolved later and control distal limb musculature.
Function:
Responsible for skilled, voluntary movements and fine motor control.
Cerebellum Involvement:
The lateral cerebellum (also called the cerebrocerebellum) initiates and refines complex, precise movements.
💡 Key Takeaway – Evolutionary Pattern:
As you move laterally and dorsally through the nervous system:
The tracts become newer (more recently evolved).
The level of movement sophistication increases.
Decussation Rule:
Older tracts (for posture and crude sensation) decussate (cross over) lower at the spinal cord level.
Newer tracts (for skilled movements) decussate higher (closer to the brainstem).
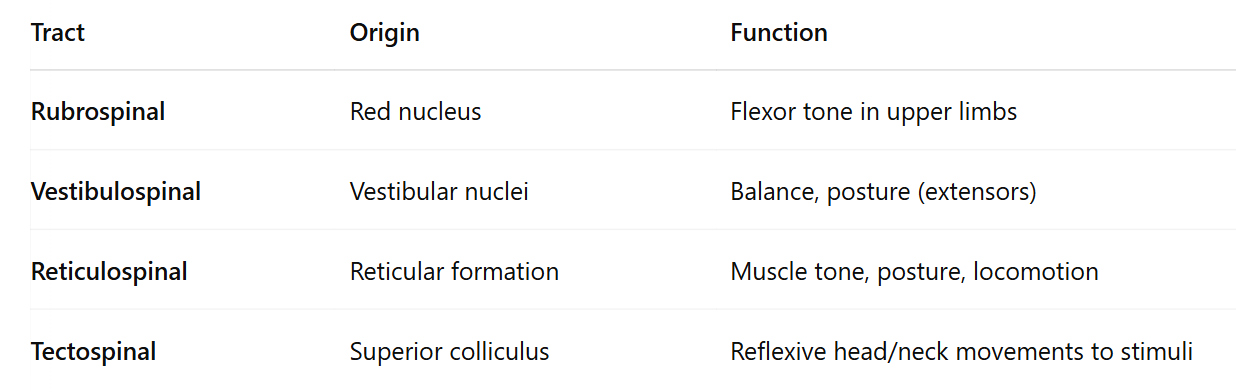
Motor Tracts, Rubrospinal Tract
The rubrospinal tract originates from the red nucleus (nucleus ruber) in the midbrain. It crosses over to the opposite side of the body and innervates distal musculature.
Key Functions:
Primarily involved in the control and modulation of the walking pattern generator in the spinal cord.
Acts as an alternative pathway for transmitting cortical and cerebellar signals to the spinal cord, helping with movement coordination.
Anatomical Importance:
The rubrospinal tract is positioned laterally in the spinal cord, which is associated with more sophisticated control of distal muscle movements, contrasting with more medial pathways that control posture.
Reticulospinal and Vestibulospinal Tracts
Reticulospinal Tracts:
Pontine (excitatory) and Medullary (inhibitory) tracts originate from the reticular nuclei of the medulla.
These tracts receive input from the motor cortex and cerebellum.
They help innervate anti-gravity muscles and play a critical role in maintaining upright posture during standing.
Gamma motor system (γ efferents to muscle spindles) helps modulate posture.
Vestibulospinal Tracts:
Originates from the vestibular nuclei of the medulla.
These tracts travel ventrally in the spinal cord and innervate neck and anti-gravity muscles, assisting in posture maintenance.
Tectospinal Tract:
Originates from the superior colliculus of the midbrain.
Primarily responsible for controlling eye movements.
Motor Cortex
CS Sherrington's Work: Sherrington conducted experiments in the early 1900s on the cortical influence of movement in animals (chimpanzees, gorillas, orangutans). He used mild stimulation of the cerebral cortex to produce movements in discrete body parts, helping map the brain's movement areas, now known as the primary motor cortex (area M1).
Wilder Penfield's Expansion: In 1951, Penfield and Jasper built upon Sherrington's work while treating epilepsy using the Montreal procedure. They mapped motor and sensory areas of the brain during brain surgery (patients under local anesthesia) and created the motor homunculus in the pre-central gyrus and the sensory homunculus in the post-central gyrus.
Motor Homunculus: Areas requiring fine motor control (e.g., lips, tongue, hands) occupy over 50% of the motor cortex due to the high number of nerves required for such precise movements.
Additional Cortical Areas
Premotor Cortex: Involved in setting posture, selecting movements.
Supplementary Motor Area: Integrates complex, planned movements.
Additional Inputs: The motor cortex receives input from the somatosensory map, posterior parietal cortex, thalamus, basal ganglia, cerebellum, and sensory areas like vision and hearing.
Motor Cortex: Now thought of as a "library of movements" rather than controlling individual muscles, with motor control signals traveling through interconnected cortical areas. It is also highly plastic.
Corticospinal Tracts
Major Descending Pathways for Motor Control:
Lateral Corticospinal Tracts (80%): Fine control over distal muscles (decussate in medulla).
Ventral Corticospinal Tracts (20%): Bilateral control of posture.
Corticobulbar Tracts: Innervate facial motor functions.
Final Common Path
The lower motor neuron, which innervates a motor unit, receives input from various neurons involved in posture and movement control, often through interneurons. This makes the lower motor neuron the final common path for signals from the upper motor neurons.
Upper Motor Neuron Lesions
Upper Motor Neuron (UMN) lesions are commonly seen in conditions like stroke and Brown-Sequard syndrome. Early experiments by Sherrington on cats helped understand the brain's role in posture and movement control. The most common UMN lesion in humans is a stroke, which can cause decorticate posturing, removing higher control over midbrain reflexes. This results in hyperactive reflexes, spastic rigidity (flexors in upper limbs, extensors in lower limbs), and a positive Babinski sign. These primitive reflexes are typically overridden by higher-order reflexes in healthy individuals with intact UMNs.
Basal Ganglia
Comprises five key structures including striatum (putamen and caudate nucleus, globus pallidus, substantia nigra, and subthalamic nuclei.
Functions in motor control and motor learning settings.
Disorders in this area manifest as excessive release or suppression of movement (e.g., Parkinson's, Huntington's).
The putamen circuit involves a loop from the cortex to the putamen, globus pallidus (GP), subthalamic nuclei, substantia nigra (SN), and thalamus, back to the cortex. Issues in this circuit lead to twisting or bending movements (such as in hands, arms, face, or neck), flailing limb movements, and dance-like flickering movements of the hands and face. It is believed to help release pre-programmed motor patterns.
The caudate circuit is involved in cognitive control of motor sequences, determining subconscious patterns of movement to achieve goals.
Both circuits' balance of movement release and suppression is maintained by a dopaminergic projection between the substantia nigra and striatum, and basal ganglia issues often arise due to disruptions in this connection.
IN THE HOSPITAL
Basal ganglia disorders cause either hyperkinesia (uncontrolled movement) or hypokinesia (suppressed movement), often due to disruptions in the dopaminergic pathway between the substantia nigra (SN) and striatum, affecting the balance of movement regulation.
In Parkinson's disease, degeneration of dopaminergic neurons reduces excitation of the striatum, leading to less inhibition of the globus pallidus (GP), resulting in greater inhibition of the thalamus, which impairs movement initiation (hypokinesia). This imbalance also causes hyperkinetic symptoms like resting tremor and rigidity (e.g., "lead pipe" or "cog wheel" rigidity).
In Huntington's disease, the breakdown of cholinergic and GABAergic pathways in the basal ganglia leads to unintentional movements such as athetosis, ballismus, and chorea.
Cerebellum
The cerebellum aids motor control by correcting movement errors and setting posture. It receives input from the cortex, brainstem, and sensory systems and outputs to the cortex and brainstem.
It is divided into three functional parts:
Vestibulocerebellum: Controls equilibrium and eye movements.
Spinocerebellum: Compares motor plans with actual movement, making adjustments.
Cerebrocerebellum: Involved in planning and programming movements, and skill development, including second language control.
Clinical Relevance of Cerebellar Control
Unlike basal ganglia issues (which cause akinesia), cerebellar problems lead to inaccurate movements, difficulty maintaining posture, and disrupted kinaesthetic learning. Damage to the vestibulocerebellum and spinocerebellum causes symptoms like wide stance, swaying, nystagmus, and ataxic gait. Damage to the cerebrocerebellum affects movement accuracy, causing dysmetria, decomposition of movements, intention tremor, and delayed movement initiation.
Interestingly, alcohol depresses cerebellar function, which is why sobriety tests often focus on cerebellar function, as seen in drunk driving tests.