Exam Uno Study Guide
Vital Signs
Methods of examination of vital signs
Blood Pressure
Measurement of the amount of pressure exerted by the blood
Measurement
mm Hg
systolic pressure/diastolic pressure
used a sphygmomanometer (blood pressure cuff) and a stethoscope
Systolic pressure
maximum amount of pressure exerted when the heart contracts and forces blood into the aorta
First Korotkoff sound heard
Diastolic pressure
minimum amount of pressure exerted when the heart is relaxed
Last Korotkoff sound heard
Cardiac Output (CO)
amount of blood pumped into the circulatory system by the heart within one minute
CO = SV x HR
Stroke Volume (SV)
amount of blood ejected by the ventricle during one heart contraction
Will an increase in CO causes an increase or decrease in BP
Increase
Contractility
the heart’s ability to contract efficiently
measured in the left ventricle
Decrease Contractility = decrease CO = decrease BP
Preload
amount of blood inside the ventricles before they contract
Decrease preload = decrease SV + decrease BP
Afterload
amount of resistance that the heart must overcome to eject the blood into the systemic circulation
increase afterload = decrease contractility = decrease CO = decrease BP
Manual Method
Place the appropriate size bp cuff on the pt
Too tight lead to higher bp
Too loose lead to lower bp
Place the cuff 1 in above the antecubital fossa
Palpate the brachial artery
Then inflate cuff to 30-50 mm Hg of pt normal bp
Slowly release at 2 to 3 mm Hg
Pay attention to the Korotkoff sounds
1st Korotkoff sound is systolic
Last one is diastolic
Electrical Methods
Use a machine to detect pt bp
Only used for pt who normal have an expected bp
Manual is more accurate and reliable than the machine
If pt have edema on arms where do you place the cuff
on the thigh
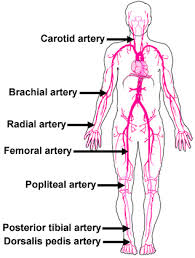
Pulses
Sinoatrial node (SA)
pacemaker of the heart
Produce electrical impulse to travel to the atrioventricular (AV) node
Cause contraction in the heart
Can hear pulse using a stethoscope or palate
apical pulse for 1 min
Listen at 5th intercoastal space for adults
4th for children
Heart Sounds
S1
dull, low-pitched “lub” sound
the mitral and tricuspid valves close
heard using the bell
S2
shorter, higher-pitched, “dub” sound
the aortic and pulmonic valves close
heard using the diaphragm
Doppler ultrasound stethoscope (DUS)
Used to find pulse if pulse is difficult or nonpalpable
Must notify provider to use
Temperature
Measurement of balance of heat produce and loss to the environment
Temperature measure site
Core
rectum
tympanic
temporal
Axillary
Surface
Oral
Axillary
Oral Temp Method
Perform hand hygiene, provide privacy, and apply clean gloves
Place thermometer under the tongue
Oral temperature range
(96.8° to 100.4° F)
Use for pt who are
4 or older
DO NOT
pt breathe through mouth
experience trauma to face or mouth
Rectal Temp Method
Assist pt to Sims’ position w/ upper leg flexed
Wearing gloves, expose the anal area while keeping other body areas covered.
Spread the buttocks to expose the anal opening.
Ask the client to breathe slowly and relax. Insert the rectal probe of the thermometer into the anus
What to do if resistance occur during a rectal temperature
Pull back immediately
Clean pt anal
Rectal temperatures range
(0.9° F) higher than oral and tympanic temperatures
When to used rectal temperature
unconscious pt or pt experiencing hypothermia
DO NOT USE
Pt have diarrhea
Have surgery in the rectal area
Rectal disorders
on infants younger than 3 m
Axillary
Place oral probe of thermometer in center of pt clean, dry axilla
Hold arms down
Axillary temperatures range
(0.9° F) lower than oral and tympanic temperatures
Tympanic
If the pt is an adult pull the ear
up and back
If the pt is younger than 3 pull the ear
down and back
Place thermometer into pt
outer ear canal
What can affect tympanic reading
ambient temp
excess earwax
DO NOT USE
on pt 3 months or younger
Temporal
Wipe lens w/ alcohol wipes
Hold probe against the temporal artery and hold button until reading occur
Temporal temperatures range
close to rectal
nearly (1° F) higher than oral
(2° F) higher than axillary temperatures
What factors can affect temp
age
hormonal changes
activity level
illness and injury
Food or fl intake
Smoking
Stress
Respiration
body’s mechanism for exchanging oxygen and carbon dioxide
Ventilation
The exchange of oxygen and carbon dioxide in the lungs through inspiration and expiration
Diffusion
The exchange of oxygen and carbon dioxide between the alveoli and the red blood cells.
Perfusion
The flow of red blood cells to and from the pulmonary capillaries.
Eupnea
regular rhythm
What all factors that affect respiratory rate
Age
Sex
Pain
Anxiety
Smoking
Position
Brain injury
Illness
Count a regular rate for 30 seconds and multiply by 2.
Count the rate for 1 min if
irregular, faster than 20/min
slower than 12/min
Oxygen Saturation
noninvasive, indirect measurement of the oxygen saturation (SaO2) of the blood
What is SaO2
percentage of hemoglobin that bound to oxygen
Capillary Refill
Test the speed of blood flow through capillaries
What is a typical normal capillary refill
less than 3 sec
What can alter the result of SaO2
nail polish or artificial nails
poor circulation
medical dye used in procedures
cold temp
Assessment findings associated with abnormal vital signs
Blood Pressure
Elevated BP
120-129 systolic
and
less than 80 diastolic
Hypertension Stage 1
130-139 systolic
or
80-89 diastolic
Hypertension Stage 2
140 or higher systolic
or
90 or higher diastolic
Hypertensive crisis
Higher than 180 systolic
and/or
higher than 120
Hypotension
less than 90 systolic
less than 60 diastolic
Orthostatic hypotension
drop of 20 systolic or 10 diastolic w/i one min after moving from sitting or standing
Pulses
Tachycardia for Adult
greater than 100/min
Bradycardia for Adult
less than 60/min
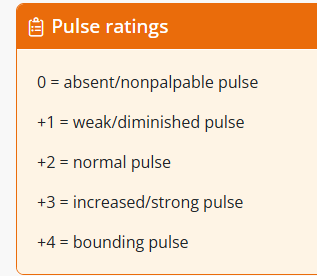
Pulse rating 0
Absent or nonpalpable pulse
Pulse rating +1
Diminished or weak pulse
Pulse rating +4
bounding pulse
Temperature
What is consider as a fever
(101.2° F)
Hyperthermia is when the body temperature
greater than (104° F)
Hypothermia
less than (95° F)
Respiration
Dyspnea
difficulties of breathing
Apnea
Absence of breathing
Bradypnea
rate less than 12/min
Hypoventilation
Shallow breathing pattern with an abnormally low rate
Tachypnea
rate greater than 20/min.
Hyperventilation
Deep breathing pattern with an increased rate
Hyperpnea
Increase in rate and depth of breathing
Cheyne-Stokes respirations
a pattern of breathing that alternating periods btw apnea and hyperventilation
Kussmaul respirations
Increase in rate and deep but regular pattern of breathing
Oxygen Saturation
Less than 95%
Placement of stethoscope
For pt younger than 7 place at 4th intercoastal space
Older than 7 place at the 5th intercoastal space
Assessing manual blood pressure
Manual Method
Place the appropriate size bp cuff on the pt
Too tight lead to higher bp
Too loose lead to lower bp
Place the cuff 1 in above the antecubital fossa
Palpate the brachial artery
Then inflate cuff to 30-50 mm Hg of pt normal bp
Slowly release at 2 to 3 mm Hg
Pay attention to the Korotkoff sounds
1st Korotkoff sound is systolic
Last one is diastolic
Documenting vital signs
Blood Pressure
systolic/diastolic, where
Pulses
Site, rate, how
Temperature
Degree C or F, site
Respiration
Rate, where
Oxygen Saturation
SpO2, %, where
Infection Control & Isolation
Isolation precautions
Standard Precautions
aka universal precaution
isolation precautions that applied to all pt
Contact Precautions
Used when pt have an infection agent that can spread through contact (direct or indirect)
Have private room
If shared do client cohorting and separate pt 3 ft
Client cohorting
grouping pt who have same infection in one area
Droplet Precautions
Used when infection agent can spread through droplets
Pt have a private room
If shared make sure both pt have the same disease and stay 3 ft away
What should pt wear when transferring
mask
Airborne Precautions
Used when infection agent can spread through small air droplet
Pt transferred to negative pressure room
12 air exchange per hr
Sterile gloving
Break in sterile technique
Below the waist
Touching non sterile items
Principles of infection prevention
Hand washing for 15-30 sec
When to use sanitized
if there isn’t visible soiled on hands
Vaccines
Nutrition balance meal and staying hydrated
Taking medicine PRN
Disinfect medical equipment
Aseptic techniques
Multi-drug resistant organisms (MDROs)
a bacterium is resistant to one or more classes of existing antimicrobials
How to decrease MDROs spread
handwash
wearing gloves
used contact precautions
What are examples of MDRO
Methicillin-resistant Staphylococcus aureus (MRSA)
Vancomycin-resistant Enterococcus (VRE)
Vancomycin-resistant Staphylococcus aureus (VRSA)
Vancomycin-intermediate Staphylococcus aureus (VISA)
Extended-spectrum beta-lactamase (ESBL)
Multidrug-resistant Streptococcus pneumoniae (MDRSP)
PPE
Gloves
Potential for direct contact w/ blood, body fl, mucous member, etc
Gowns
Potential of contacting infected material
potential for blood or body fl contaminate HCS
Mask
Used for droplet precautions
N95 respiratory mask for airborne precaution
Googles
Potential when procedures may splashed blood or body fl into the eyes
Protect eyes, nose, and nose
Face shield
provide additional support to goggles
Hygiene
Perineal care
Cleaning the area btw tail bone and pubic arch
female perineum
btw anus and vulva
male perineum
scrotum and anus
What type of soap is used for perineal care
pH balance soap
urinary catheter care
Hand hygiene and don gloves
For males
pull back the foreskin and clean everything
For females
clean area btw labia (anterior to posterior)
Next clean the urethra and then clean the catheter
Perineal care (male)
Clean penis from meatus outward in circular motion
Pull the foreskin back and clean the skin
Place the foreskin back after cleaning
prevent swelling, pain, and decrease circulation to penis
Perineal care (female)
Wash anterior to posterior
Why shouldn’t nurses wash female pt posterior to anterior
increase risk of UTI due to bacteria moving closer to urethra
Bariatric skin care
Bariatric
Medical field specialize in treating obesity
Skin folds
area with excessive skin that overlap with each other
Why is it bad for moisture occur in skin fold
can developed a rash which can turn into an infection
What is the nursing interventions to help prevent the skin fold be moist
washing skin with pH-balance soap and gentle dabbing skin dry
What to do if pt w/ obesity have a fungal infection
notify provider and ask nystatin powder is needed
What used to clean the perineal for obese pt
barrier creams and films
Foot care
Keep the foot entirely dry especially area btw toes
Apply lotion to feet but avoid btw toes
prevent fugal infection
Inspect toes for any
cuts, blisters, cracked skin, or discoloration
Nurses should monitor the feet of clients who have ____ _____ due to having higher risk for having an ____
diabetes mellitus; infection
If approval, trim pt’s toenails straight across and file the edges
Tissue Integrity
Assessing wounds
What should be assessed during dressing changes
healing
infection
color, amount, and odor of exudate
surrounding skin char
measure wound
clock format for loc and extent of tunneling
l x w x depth
Tunneling
a wound that form passageways underneath the surface of the skin
Wound Exudate
Serous
thin, watery wound drainage

Serosanguineous
thin, watery wound drainage mixed with blood

Sanguineous
bloody wound drainage


Purulent
green/yellow wound drainage

Staging pressure injuries
Stage 1
Non Blanchable Erythema
Remain red even after applying pressure

Stage 2
Partial Thickness Skin Loss
see a pink or red tissue in wound bed

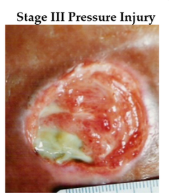
Stage 3
Full Thickness Skin Loss
Adipose tissue is visualize
Granulation tissue
new skin tissue that forms on surface of wound
Dead tissue, undermining, and tunneling may formed
Tunneling
a wound that form passageways underneath the surface of the skin
Undermining
separation of the wound edges from the surrounding healthy tissue
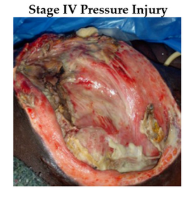
Stage 4
Full-Thickness Skin and Tissue Loss
The fascia, muscles, tendons, ligaments, cartilage, and/or bone are visible
Edges are rolled
Undermining, dead tissue, and tunneling may be present
Unstageable Pressure Injury
Obscured Full-Thickness Skin and Tissue Loss
Full damage in wound bed can’t be determined
Covered in either slough or eschar
Slough
Yellow, stringy nonviable tissue found in the base of the wound
Eschar
Hard nonviable black/brown tissue found in the wound bed.
Must removed eschar to reveal if wound is stage 3 or 4 pressure injury

Deep Tissue Pressure Injury (DTPI)
Persistent non-blanchable tissue injury of the skin appearing deep red, maroon, or purple color.
Skin may be intact or broken
Result of intense or persistent pressure and shearing

Risk factors for impaired skin integrity
Age
Impaired Mobility
Moisture
nutritious
Impaired sensory
Weight
Skin fragility
skin tears
cellulitis
inflammation of skin and underlying tissue
Skin changes in older adults
Thinning of skin
Decreased in
elasticity
subcutaneous tissue
blood
hydration
Skin Problems
skin tears
pressure injuries
itchy, dry, flaky skin
skin infections
cellulitis
Mobility
Bed mobility
Prone
Lying on abdomen with the head turned to one side
hips are unflexed
Supine or dorsal
Lying at on the back and knees bent
Lateral
Side-lying
hips and knees are flexed with a pillow separating the knees/legs
Fowler
Semi-seated or reclined position with the head of the bed
Semi-Fowler
Head of the bed is elevated 15 to 30 degrees
High-Fowler
Head of the bead is elevated 60 to 90 degrees
Lateral semi-prone
Placed between the prone and lateral positions
with the top leg flexed up toward the chest and supported with a pillow
the bottom arm is placed to the side of the torso
Trendelenberg
Lying at on the back, with the foot of the bed above the HOB
Reverse Trendelenburg
The foot of the bed is lower than HOB
Patient transfers
Maximum assistance:
The client cannot bear weight, assist, or maintain a seated position.
Use a total mechanical lift or sling.
Moderate assistance:
The client can maintain a seated position and has some upper extremity strength
lacks enough lower extremity strength to transfer safely.
Use sit-to-stand powered lifts and assistive devices.
Minimum assistance:
The client can rise from a seated position and sustain a steady stand.
Use a gait belt and ambulation assistive devices as indicated.
No assistance:
The client can stand, march or step in place, and walk without any
Slide or transfer board
allows the lateral transfer of a client without imposing the physical exertion of lifting on the HCS
used for immobile or acutely ill and unable to assist patients
Pivot disc
used for sitting or standing transfers for clients who are cooperative and have weight-bearing capabilities
cooperative and have weight-bearing capability patients
Mechanical sit-to-stand
used to assist the client in rising from a seated to a standing position
Surgical pain or trauma patients
possesses the lower extremity strength and balance required to maintain an upright position
Mechanical lift
clients who cannot support their own weight
ROM exercises
Passive ROM
The movement of a joint by another individual.
Active ROM
Voluntary movement of a joint.
Flexion
bend
Extension
straighten the limb
Abduction
move away from baseline
Adduction
bring closer to baseline
Pronation
turning to face backward
Supination
turning to face forward
Circumduction
circular motion
Rotation
side-to-side
Inversion
turn inward
Eversion
turn outward
Safety
Fall prevention interventions
Fall risk screening used for all pt upon admission
Nurses removed anything that could caused a potential fall in pt’s room
Keeping bed in low position
Locked bed’s wheel and wheelchairs
Have call light near pt and encourage them to use it
Good lighting
Non-skid footwear
Educate pt and family
Surgical “Time out”
a brief pause in the surgical procedure to verify critical information and ensure patient safety
confirm the patient's identity, procedure, and surgical site
review any potential risks
ensure that all necessary equipment and supplies are available
coordinate communication among the surgical team members
Hospital-acquired infections (HAIs)
SSIs, CUATIs, CLABSIs
burns/electrical shock
Blood transfusion
Injury from falls
Insulin usage
Optimal blood sugar management
DVT
Pressure injuries
Unexpected Events
client safety event
an unexpected event that occurred with or without injury to the client but that had the potential to cause harm to the client
Near miss
potential event that could have caused harm but that was caught and avoided.
adverse event
a situation that caused unexpected harm to the client.
A sentinel event (never event)
critical, unexpected adverse event that causes severe physical or psychological harm to a client