(5) Cost-benefit analysis (CBA)
Analysis based on the idea of Welfare economics (decisions regarding public policies by balancing effective use of resources with public preferences).
Started in 1960 to assess polio vaccine cost benefit to children. The benefit of the program was weighed against the loss of productivity & reduced survival (monetized by wages). Those benefits were changed to monetary terms in Pharmacoeconomics.
It is theoretically the best way of analysis, but is practically still underdevelopment. Mostly used for awareness programs.
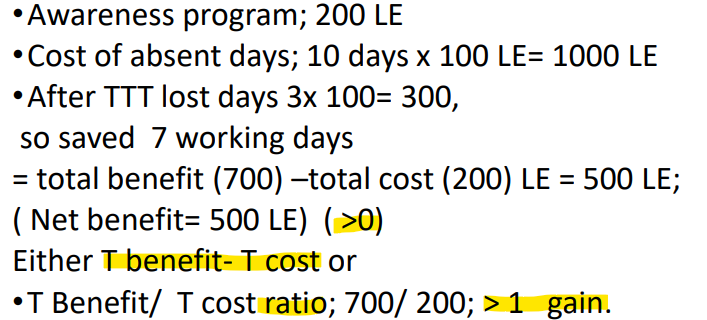
Awareness programs
Impart health education to the community
Could be for acute or chronic diseases
Data should exist regarding number of cases before and after the program
Advantages:
Different outcomes can be compared (outcomes in monetary values)
Programs can be ranked.
Ranking the programs is considered very important because decision makers need to determine which to implement and how to implement.
Disadvantages:
Difficult to outcome in monetary value
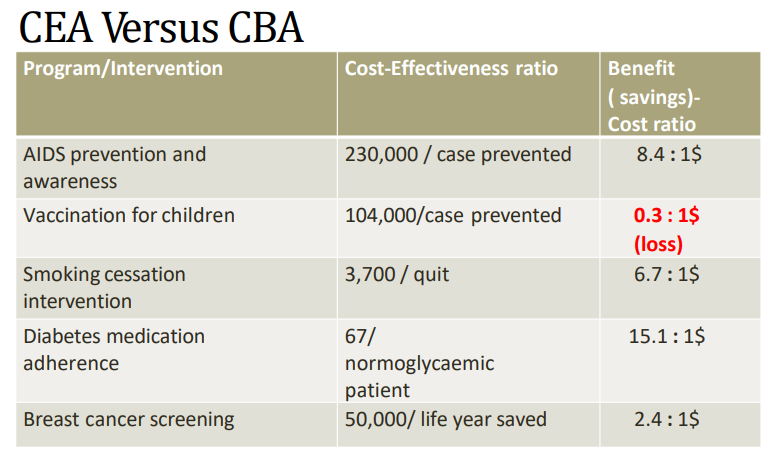
Quantifying life controversial (AIDS Vaccination).
Steps of conducting CBA
Determine type of program intervention
Identify alternatives
Identify costs and benefits of each
ex: Asthma clinic; clinic vs. no clinic or full operating clinic vs emergency patients only.
Because of its focus on social welfare and policies, and the incorporation of indirect (productivity) or intangible benefits, economists recommend that CBAs should be done from a Societal Perspective.
If only direct medical benefits are considered (not productivity as well), then study may be classified as cost analysis (not PE analysis) by some researchers.
Components of CBA
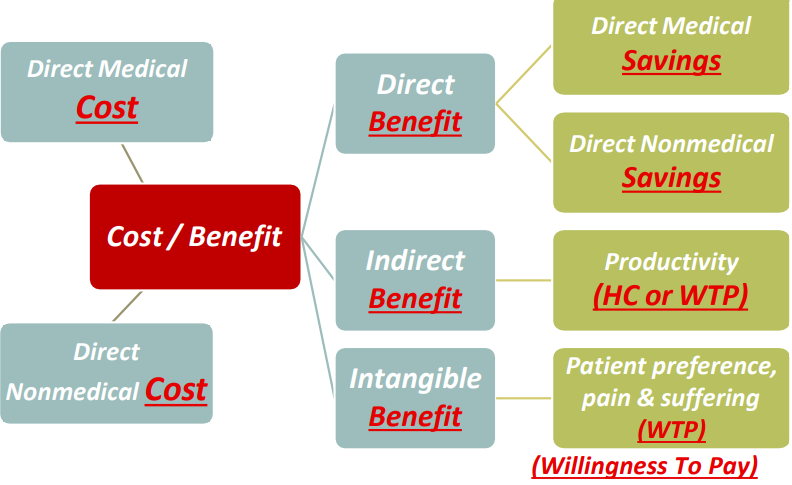
Difference between cost and benefit
Cost | Both | Benefit |
The money paid. | Are medical and non-medical factors | The money saved |
Measured in dollars |
Measuring Indirect & Intangible benefits
Most commonly used methods are:
Human Capital Approach
Willingness to Pay
Less common methods are implied values or cost preference
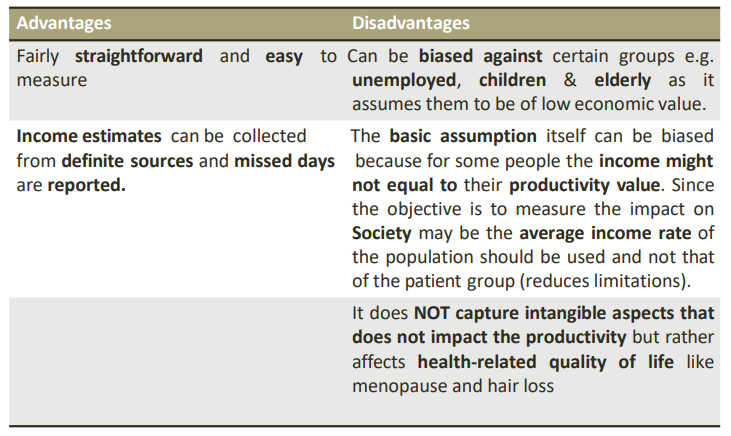
Human capital method
Measures cost benefit in productivity level. It assumes that the VALUE of health benefits EQUAL the economic PRODUCTIVITY they permit. Done by estimating wage loss due to illness, disability or death (absent days).
The usual working days/year= no. of days/year- annual leaves-weekends- sick leaves = 240 days.
This method depends on wage rate and missed work times.
Calculating wage rate from:
Yearly wage rate (if program/intervention for reducing long term disability or death)
Daily income (for acute illness or short-term disability)
Fringe benefits should be included.
Missed time because of illness includes categories:
Missed work days; for the employed (Self reported/ from the HR)
Missed housekeeping, for the unemployed.
Restricted activity days, did not miss but could not work the full time.
Caregiver’s time, ex parent with ill child.
Willingness to pay method
How much people are willing to pay to reduce the chance of an adverse health care outcome. This method incorporates patient preference and intangible outcomes.