Lec 3
Objectives
Pathological Presentation of Advanced Atherosclerosis (ASCVD) - Comprehensive overview of the disease mechanisms, biomarkers involved in pathogenesis, and methods for diagnosis including imaging techniques and laboratory tests.
Clinical Features and Considerations - In-depth review of risk factors including genetic predisposition, lifestyle choices, signs, symptoms, and the clinical staging of atherosclerosis (ASCVD) to facilitate early detection and intervention.
Evidence-Based Management - Cardiac Rehabilitation - Analysis of medication influences, the spectrum of side effects impacting exercise performance, medical interventions’ effectiveness, mechanisms that contribute to potential benefits, and identification of red-flags for exercise in patients.
A concept of supply. and demand
cardiac muscle can work for 30min before death
Angina Pertoris
Results in progressice cascade of abnormalities
Patient will feel unwell
Angina, SOB, Nausea, sweating
most worrying is no pain- silent ischemia
Flipped T wave is ischemia
Ischemic hears start to fill and pump inefficiently
Can lead to arrhythmias- VT, VF
Chest pain or discomfort as a consequence of poor coronary perfusion
Pain located
Chest
Neck
Jaw
Back pain
Pressure may radiate or may not radiate into the left arm
Brought on by exertion and relieved by rest and/or with nitoglycerin spray
Progressive Development of ASCVD
Stages of ASCVD
CVD Risk Factors: Major influences on heart health including hypertension, obesity, and sedentary lifestyle, along with their cumulative effects.
Endothelial Dysfunction: Impaired functioning of the inner lining of blood vessels resulting in increased permeability and inflammatory cell transmigration.
Atherosclerosis: Formation of atheromatous plaques in arteries causing narrowing and potential occlusion, with risk factors contributing to plaque development.
Coronary Artery Disease (CAD) Onset: Reduced blood supply to the heart muscle leading to angina and myocardial ischemia.
Myocardial Ischemia: Insufficient blood flow and oxygen to the heart muscle, particularly during exertion or stress, resulting in chest pain.
Coronary Thrombosis: Formation of a blood clot within a coronary artery exacerbating ischemia and leading to myocardial infarction.
Acute Coronary Syndrome (ACS) - Now recognizes myocardial infarction (MI): This stage requires immediate medical intervention to restore blood flow.
Arrhythmia & Muscle Loss: Altered heart rhythms that may lead to sudden cardiac arrest and deterioration of myocardial tissue.
Ventricular Dilation: Enlargement of the heart chambers as a compensatory mechanism which can lead to heart failure over time.
Congestive Heart Failure: The heart's inability to pump effectively, leading to systemic and pulmonary congestion.
End Stage Heart Disease: The final stage of cardiac deterioration where the heart fails to maintain adequate circulation leading to life-threatening complications.
Atherosclerotic Cardiovascular Disease (ASCVD) Overview
Definition: A term encompassing diseases of the heart (cardio) and blood vessels (vascular), including but not limited to the following:- Hypertension: Elevated blood pressure potentially leading to heart disease.
Angina: Chest pain due to insufficient blood flow during physical stress.
Ischemic Heart Disease (IHD): A significant condition characterized by imbalanced oxygen supply to the myocardial tissue.
Coronary Heart Disease (CHD): Affects coronary arteries, leading to reduced blood flow.
Coronary Artery Disease (CAD): Characterized by atherosclerosis in coronary arteries.
Peripheral Artery Disease: Reduced blood flow to limbs affecting mobility and function.
Ischemic Heart Disease (IHD) and Angina Pectoris
Definition of Ischemic Heart Disease (IHD): A condition arising from reduced blood flow to the heart muscle generally due to atherosclerosis, leading to symptoms of angina or even myocardial infarction if not treated timely.
Factors Influencing Atherosclerosis
Multiple pathological factors contribute to plaque instability and rupture, including:- Plaque composition involving cholesterol, cellular debris, and inflammatory cells.
Fibrous cap vulnerability due to matrix metalloproteinases degrading the protective layer.
Inflammatory mediators that aggravate endothelial injury…
Generally, asymptomatic until approximately 70% luminal narrowing is reached, significantly reducing the reserve capacity of coronary arteries.
Stable Angina: Characteristics include predictability upon exertion or emotional stress, typically relieved by rest or nitroglycerin, indicating the balance between myocardial oxygen supply and demand is restored.
Vulnerable Lesion: Often involves a lipid-rich core and thin fibrous cap, leading to increased risk for acute coronary events due to spontaneous rupture.
Cascade of Abnormalities: Disruptions in supply-demand dynamics can lead to a variety of clinical symptoms from exertional fatigue and angina pain to arrhythmias.
Oxygen Supply and Demand Concept
Myocardial Oxygen Supply-Demand Relationships:
Normal myocardial metabolism requires adequate oxygen supply to maintain cellular functions.
Myocardial ischemia occurs when oxygen supply falls short of metabolic needs, particularly pronounced during physical exertion or emotional stress, precipitating angina or infarction.
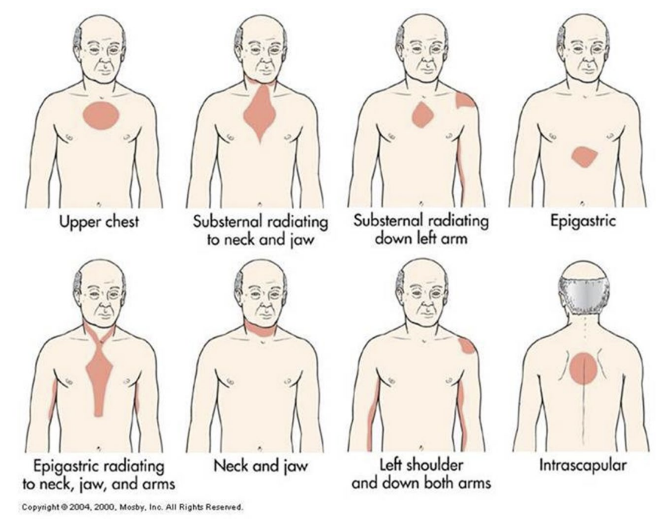
Angina Pectoris Definition and Symptoms
Definition: Angina is defined as chest pain or discomfort resulting from inadequate coronary perfusion, typically occurring during stress, physical exertion, or emotional turmoil.
Symptoms:
Patients often describe the pain as radiating to the neck, jaw, back, or arm, with a common sensation of pressure, squeezing, or tightness.
Symptoms tend to be aggravated by physical exertion and relieved upon rest or administration of nitroglycerin, a vasodilator that enhances blood flow to the myocardium.
Types of Angina:- Stable Angina: Predictable occurrences, usually during exertion; resolution upon rest indicates effective management of ischemic episodes.
Unstable Angina: Characterized by new onset or exacerbating symptoms that may occur at rest, representing a greater risk for progression to acute coronary events or myocardial infarction.
Symptoms and Related Risk Factors for Angina
Common Risk Factors: Tobacco use, abnormal lipid profiles (hyperlipidemia), diabetes mellitus, hypertension, significant family history of coronary artery disease (CAD), previous episodes of stroke, or peripheral vascular disease (PVD).
Symptoms of Angina:
Patients often report pressure in the sternum along with dull aches in the jaw/neck, back pain, fatigue, shortness of breath (SOB), nausea, and diaphoresis (excessive sweating).
Notably, silent ischemia may occur particularly in elderly patients and those with diabetes, highlighting the importance of regular cardiovascular monitoring.
Clinical Presentation of Angina
Location of Pain:
Pain can manifest in various locations including the chest, neck, jaw, shoulders, and back; it may vary with physical exertion or emotional stress, offering a critical diagnostic insight.
Critical Signs of Angina During Exercise
Symptoms warranting immediate medical attention include:- Chest discomfort felt as pressure or pain during exertion, potentially indicating myocardial ischemia.
Referred pain may occur in arms, neck, jaw, or back, hinting at cardiac distress.
Other concerning symptoms include shortness of breath, nausea, dizziness, profuse sweating, and unexplained fatigue.
Exercise Precautions: Patients are advised to promptly pause any activity that induces chest pain or discomfort and seek medical evaluation as needed to avoid adverse cardiac events.
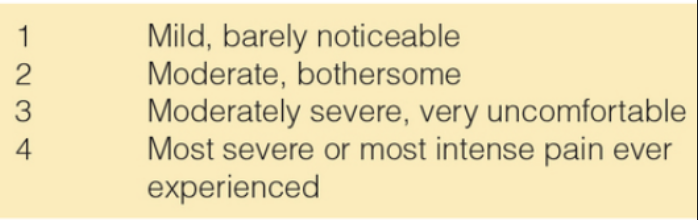
Angina Rating Scale
A tool designed for patients to quantitatively describe their experience of chest pain:- 1: Mild, barely noticeable
2: Moderate, bothersome
3: Moderately severe, very uncomfortable
4: Most severe or intense pain ever experienced, providing clinicians with valuable data on the patient's condition and symptom management.
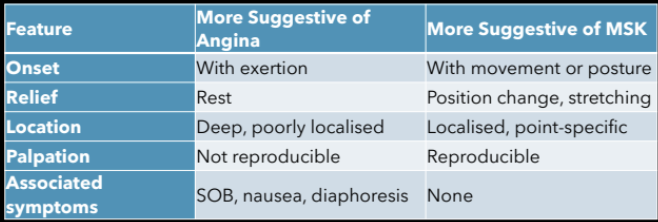
Identifying Atypical Back Pain as Possible Angina
Atypical presentations demand heightened vigilance among clinicians; atypical pain patterns may indicate underlying cardiomyopathy rather than straightforward musculoskeletal issues.
if they have a cardiac history with back pain- cardiac
if they have family history of cardiac with back- cardiac
cardiac cant be palpitated and stops with exercise
Key differences for cardiac vs muscoloskletal
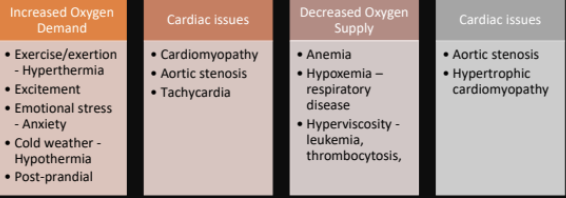
Factors Influencing Oxygen Demand and Supply
Increased Oxygen Demand:
Elevated demand can arise during activities such as vigorous exercise, acute emotional stress (anxiety), significant temperature fluctuations, and certain cardiac conditions like tachycardia or hypertension.
Decreased Oxygen Supply: Decreasing oxygenation can stem from conditions such as anemia, severe respiratory diseases (hypoxemia), increased blood viscosity (hyperviscosity), and various cardiac issues, compounding the challenge of maintaining adequate myocardial perfusion.
ECG Effects of Myocardial Ischemia
Key changes manifest primarily through variations in T waves and may include:- Abnormal Q waves, ST segment elevation, and inverted T waves during myocardial infarction, serving as crucial diagnostic indicators.
Atherosclerosis - Plaque Composition and Consequences
Increased lipid accumulation leads to LDL oxidation, exacerbating inflammation, destabilizing plaques, and heightening risks for thrombotic events.
Consequence: Acute coronary events, including myocardial infarction (MI), can occur due to sudden plaque rupture, emphasizing the need for effective management of atherosclerotic risk factors.
Myocardial Infarction (MI) Definition and Pathophysiology
Definition: Myocardial infarction is defined as a lethal arrhythmia or cardiac arrest resulting from inadequate coronary blood flow causing myocardial necrosis due to occlusion, typically from thrombus formation over a ruptured plaque.
Factors influencing the extent of injury include: location of occlusion, duration of ischemia, overall vascular supply, and demand proportion.
MI pathology involves a combination of endocardial, myocardial, and epicardial damage which is contingent on occlusion severity and the presence of collateral circulation.
Myocardial Infarction Diagnosis Criteria
Extent of injury depends on
Location
degree of occlusion
duration of the occlusion
amount of heart tissue supply by the vessel
metabolic needs the tissue
extent of collateral circulation
heart rate, pulse and cardiac rhythm
Diagnosed upon evidence of myocardial necrosis with clinical symptoms of ischemia, new ST segment/T-wave changes, or pathological Q waves observed on electrocardiogram (ECG).
Rises in cardiac biomarkers, i.e., cardiac troponins (cTn), are critical for confirming diagnosis, peaking approximately 12 hours post-injury and remaining elevated for 7 to 10 days post-event.
Symptoms
Clinical Manifestations of Myocardial Infarction
Typical symptoms differ markedly between men and women to enhance diagnostic awareness: men
Chest pain of discomfort
shortness of breath
Nausea
Women
Back
Neck
Jaw
Chest discomfort
dizziness
vomiting
fatigue
lightheadedness
nausea
shortness of breath
sweating ,
necessitating vigilance in recognition and treatment as they may not present with typical angina symptoms.
Acute Myocardial Infarction Clinical Signs and Symptoms
Marked variability may occur in pulse (bradycardia or tachycardia), potential hypotension, elevated jugular venous pressure (JVP), fine crackles on auscultation, and an elevation in leukocytes (↑ WCC), indicating inflammatory processes proceeding.
Special Considerations for Women and Cardiovascular Disease
Women are significantly underrepresented in clinical studies, creating knowledge gaps regarding cardiovascular disease (CVD) risk factors specific to them.
Special consideration is essential for distinct risk factors such as autoimmune diseases, hormonal influences, and the multifaceted impact of pregnancy on cardiovascular health. Women require individualized management strategies that account for unique clinical presentations, symptom expression, and responses to treatment for heart disease.
Principal biochemical consequence of AMI
CArdiac Troponin
none in a normal body, when you have a heart attack there is levels
cTn and cTnl detectable within one hour of myocardial injury have high specificity at 3-6 hrs following the onset symptoms and reach peak levels within 12 hrs
ECG
depression lead 3- anterior
elevated lead 3- inferior
cardiac rehab
Aims for cardiac rehab for angina and myocardial infarction
broad aims
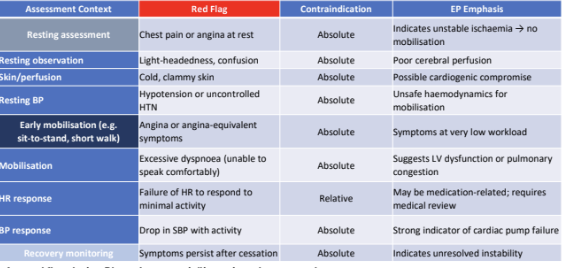
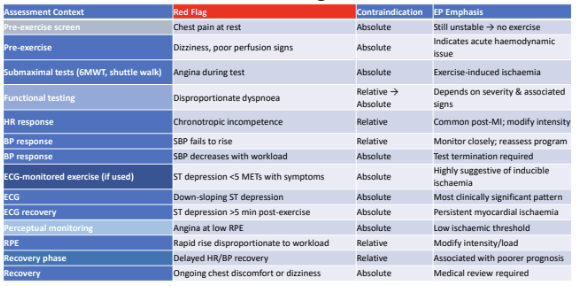
AEP Take-Home Messages for Clinical Practice on Exercise Prescription
Exercise should be prescribed below the ischemic threshold to avoid inducing symptoms.
Warm-up and cool-down periods are essential components in enhancing safety and reducing the risk of ischemic events.
Continuous monitoring is crucial during exercise, particularly in patients on rate-modifying medications to respond swiftly to any adverse changes.
Education is key to empower patients with the understanding that exercise can be safe and beneficial, helping them manage their condition effectively.
Components of Cardiac Rehabilitation
Programs aim to enhance overall health and well-being over a consistent period of 6-12 weeks through
Structured exercise, lifestyle education, psychological support, and behavior modification strategies while effectively managing risk factors.
Comprises: Interdisciplinary collaboration is vital among cardiologists, nurses, exercise physiologists, psychologists, pharmacists, physiotherapists, and occupational therapists to ensure comprehensive patient care.
Rehab
Phase 1
Phase 2
exericise rehabilitation
Frequency
intensity
Time
RPE
ideally 11-13

Overall Rehabilitation Goals
Address psychological barriers related to exercise engagement.
Maximize physical and social functioning to improve quality of life.
Prevent disease progression and subsequent deconditioning through ongoing assessments and adjustments.
Encourage sustainable behavior changes to minimize the risk of future cardiac events through lifestyle adaptations and health management practices.
Monitoring Response to Exercise
Rigorous monitoring is essential throughout each rehabilitation phase to appropriately adjust exercise regimens, ensuring patient safety and effectiveness of the interventions.
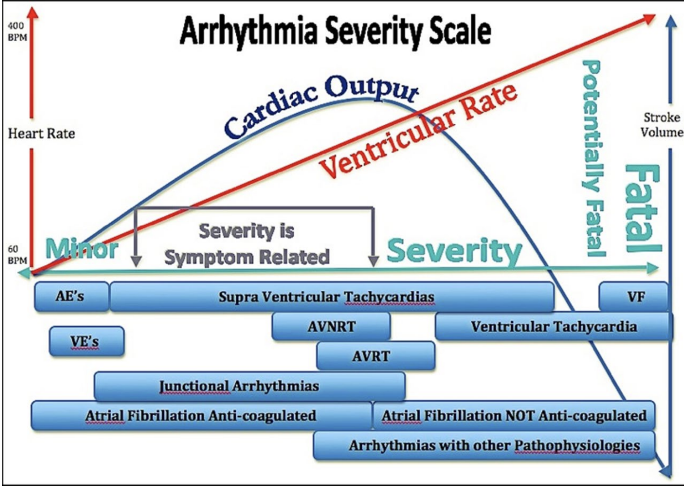
Arrhythmia severity scale
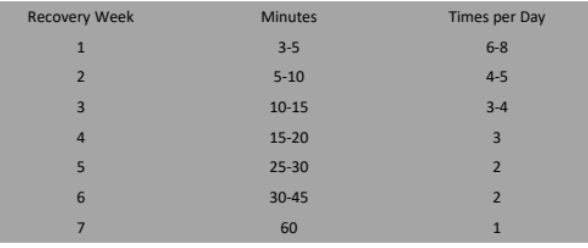
Cardiac warm
15-20min
Resistance training
Cool down
5-10min extended
Long-term Management and Adaptations
Emphasis on fostering sustainable exercise habits tailored to each patient's individual capacity and health status to significantly enhance the quality of life and achieve desirable functional outcomes.