Abdominal Cavity, Peritoneal Cavities and Mesenteries
Abdominal cavity is one in which the gut tube is suspended from the posterior abdominal wall and partly from the ventral abdominal wall by thin sheets of tissue called mesenteries.
abdominal cavity
Superior part of abdominopelvic cavity
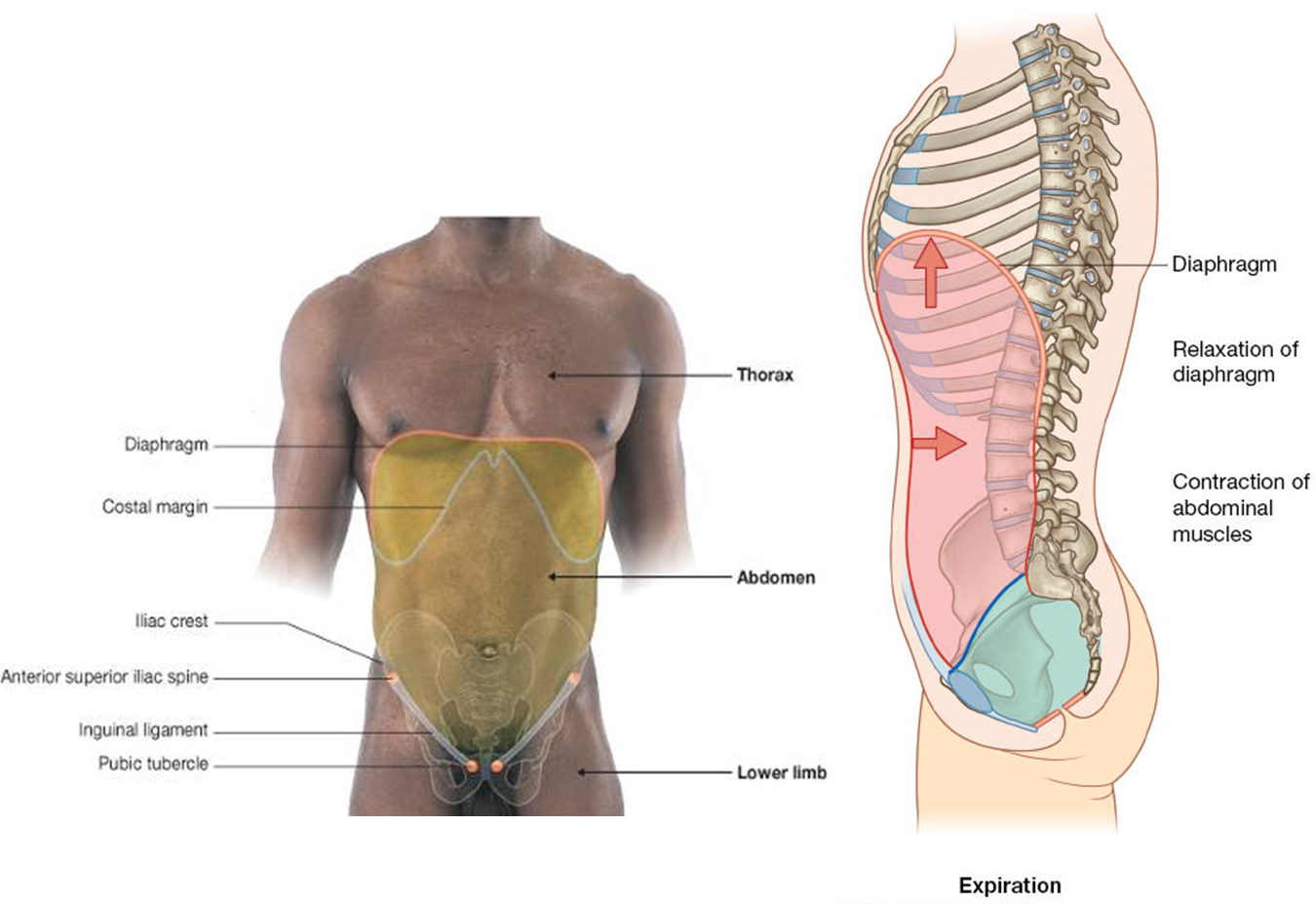
Upper boundary – thoracic diaphragm
Lower boundary – superior pelvic aperture or pelvic inlet
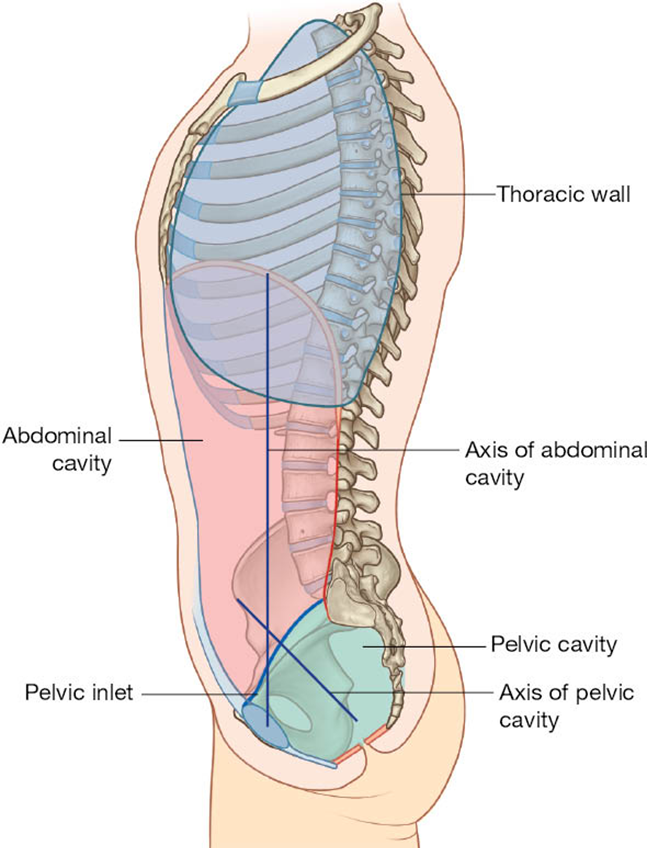
During expiration, extends as high as the 4th intercostal space, which is the level of the nipple in the male.
Contents
Peritoneum
Parietal: Lines the cavity
Visceral: Covers viscera
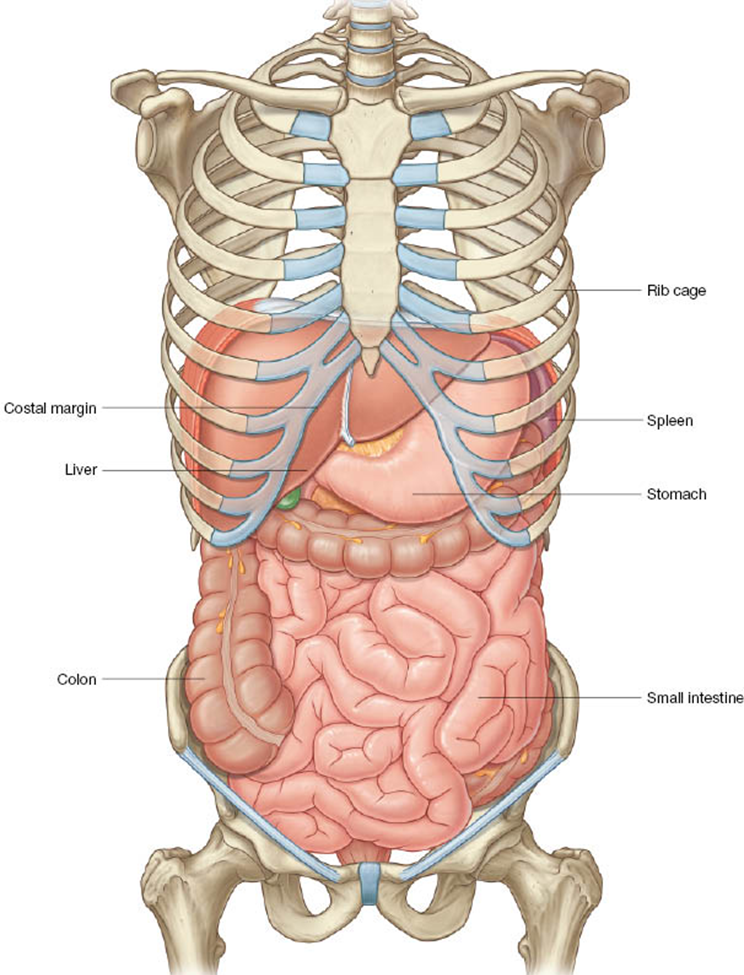
Abdominal viscera
Digestive organs
Spleen
Kidneys
Adrenal glands
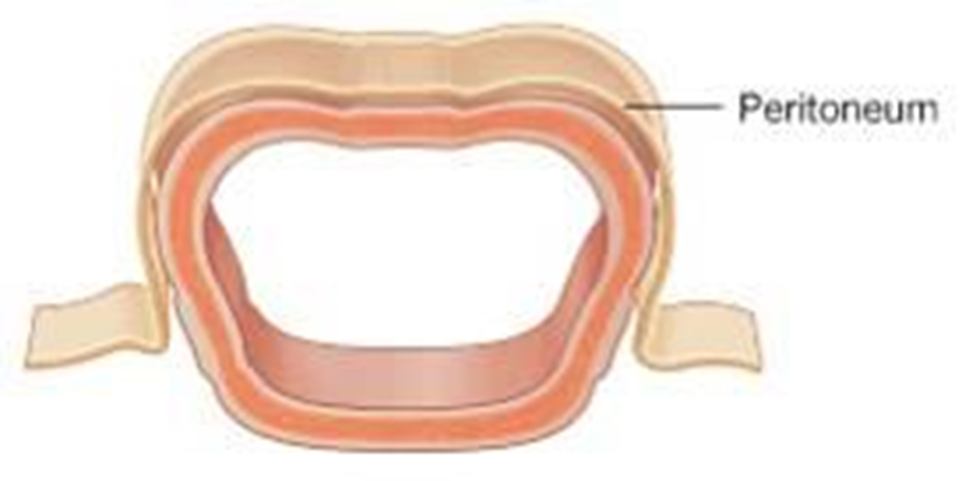
peritoneum
A continuous, glistening, transparent serous membrane
Parietal peritoneum: Internal lining of the abdominopelvic cavity
Visceral peritoneum: invests the organs, forms mesenteries, omenta and ligaments
The layers form the peritoneal sac that encloses the peritoneal cavity
the viscera lie outside of the peritoneal cavity
Both the parietal and the visceral peritoneum are glistening, slippery, transparent serous membranes made up of a simple squamous epithelium, mesothelium.
The parietal peritoneum lines the body wall and, therefore, has the same blood supply and innervation as the body wall.
The visceral peritoneum covers the viscera and, therefore, has the same blood supply and innervation as the organs it invests.
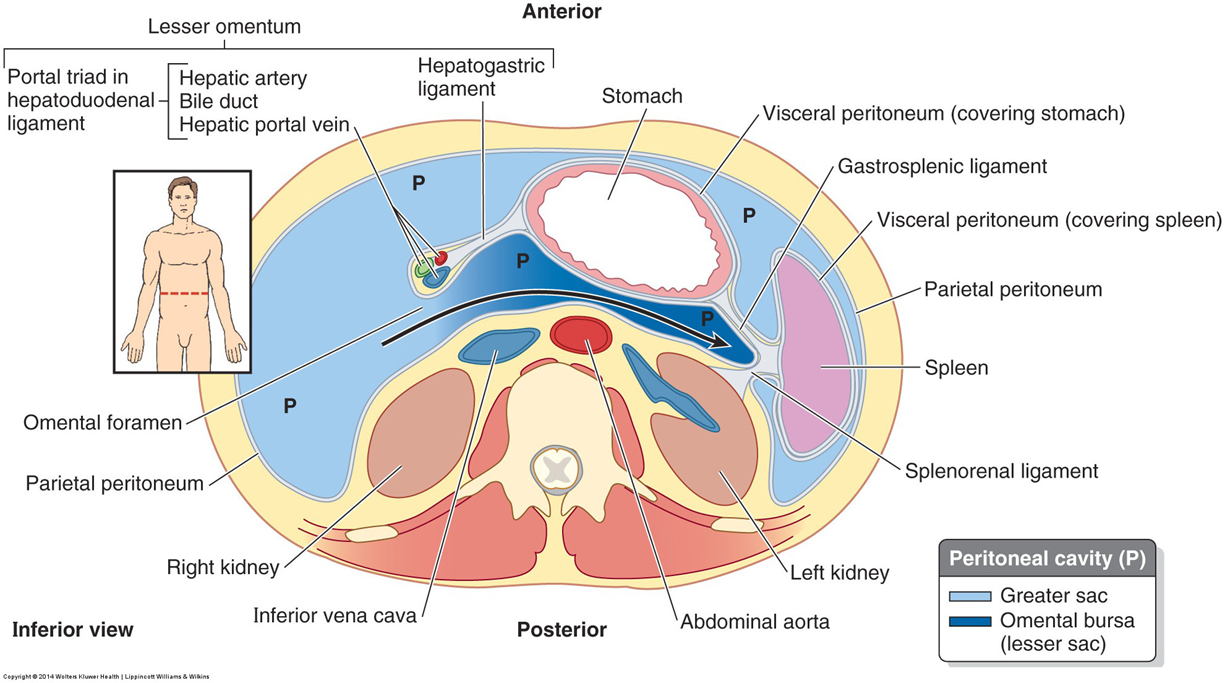
peritoneal cavity
can be divides into 2 spaces or sacs
The greater sac (cavum peritonei)
Lesser sac (omental bursa)
principle formations of peritoneum
development of peritoneum
Lateral mesoderm splits
Parietal or somatic mesoderm
Gives rise to parietal peritoneum which lines abdominopelvic cavity
Visceral or splanchnic mesoderm
Gives rise to connective tissue and muscular parts of gut wall
Forms visceral peritoneum and mesenteries
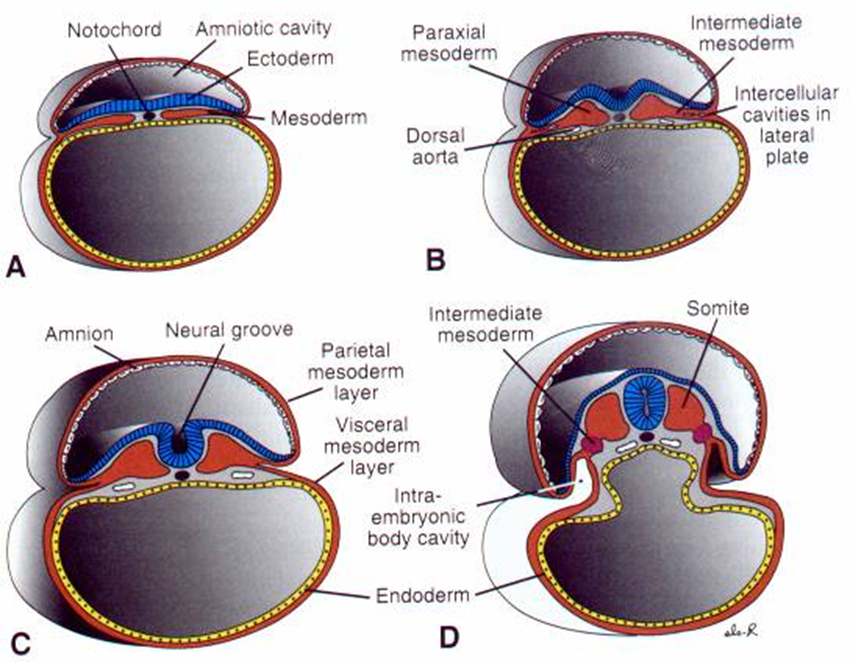
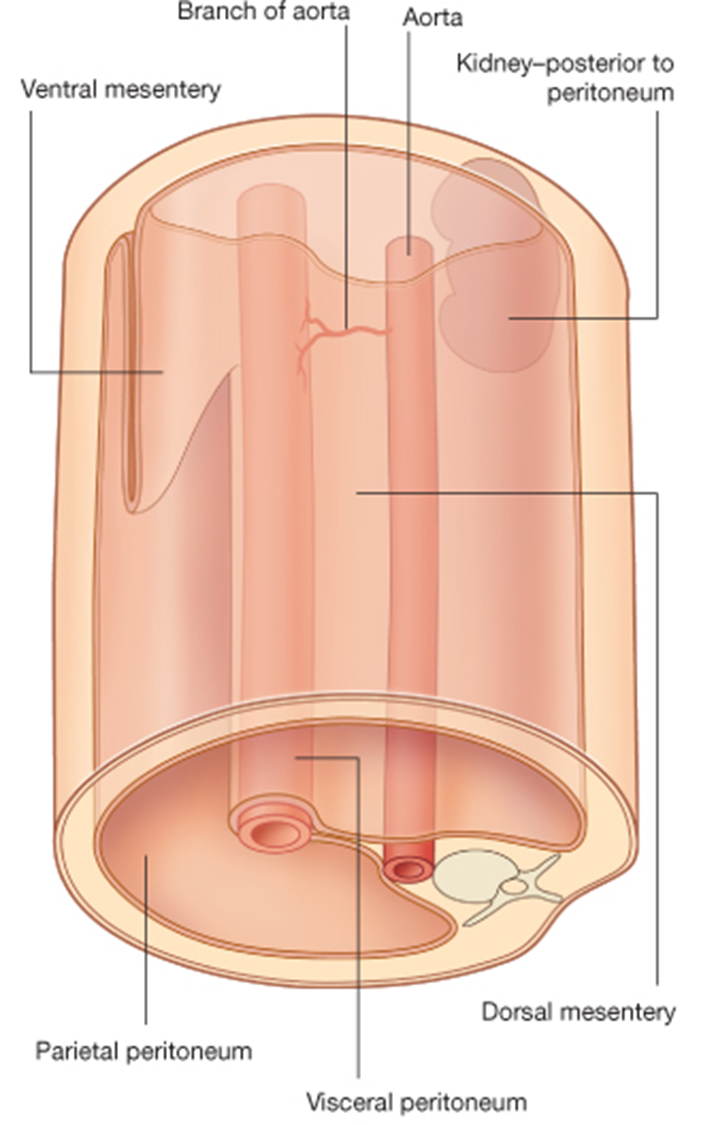
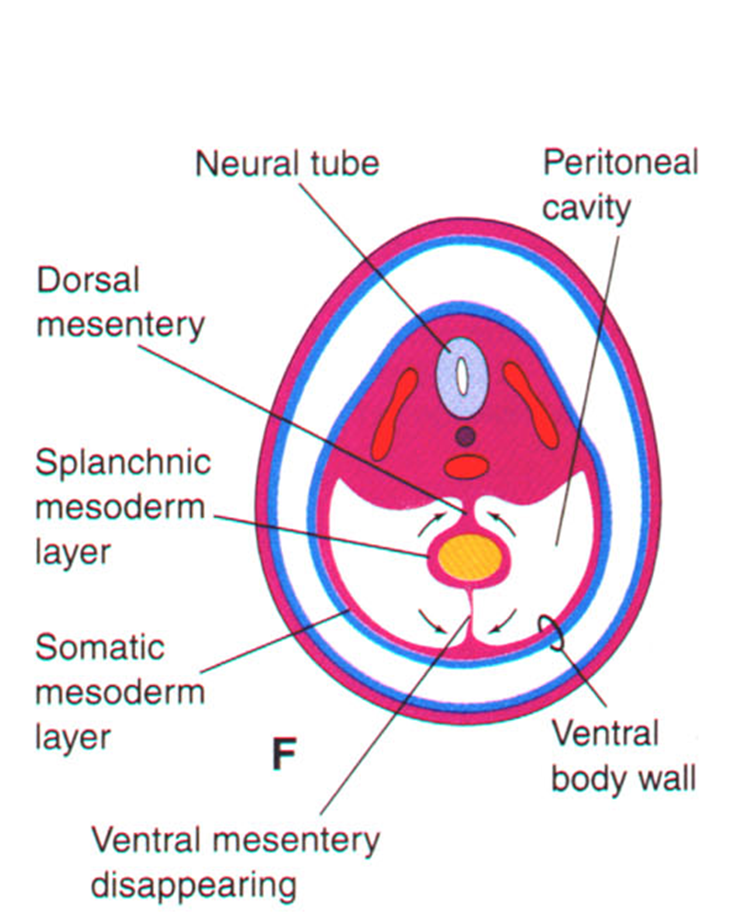
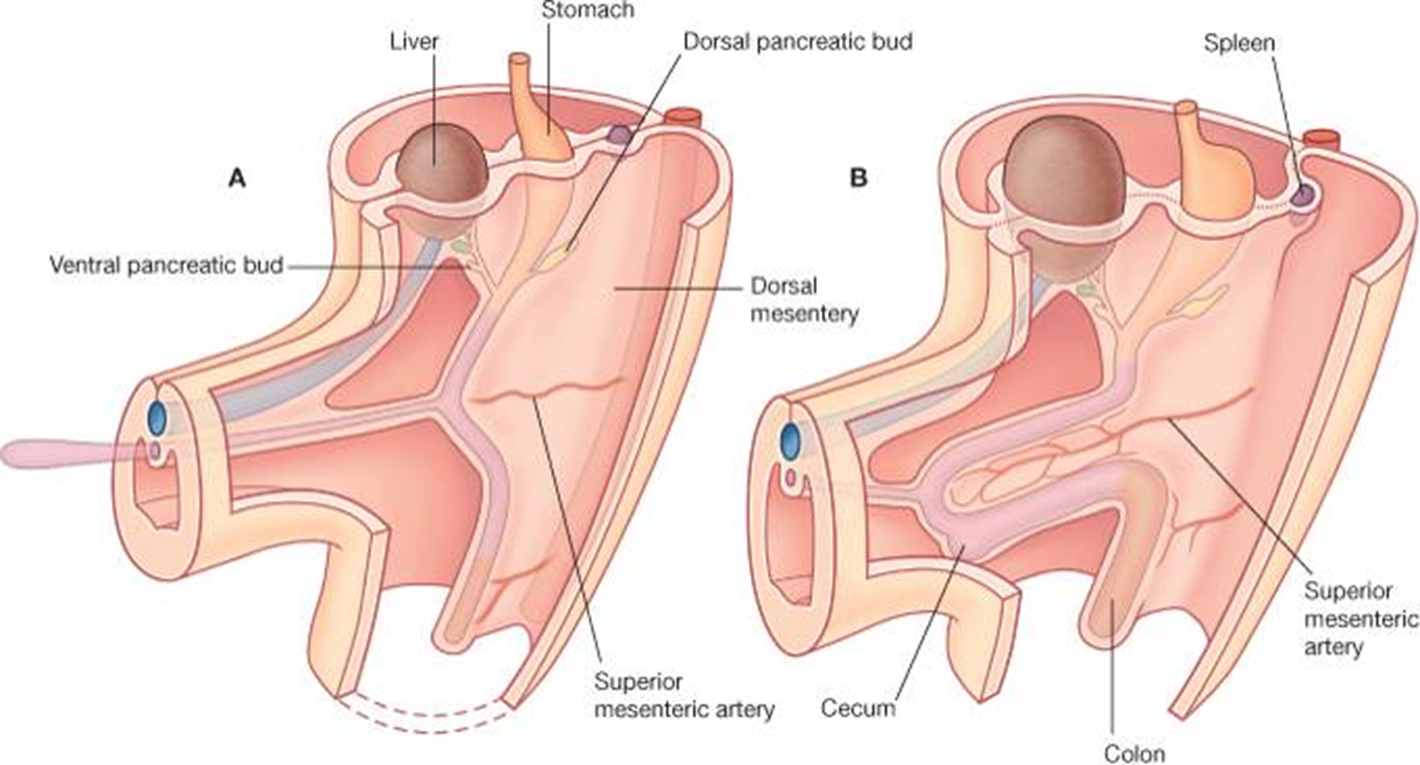
The folding of the embryo leaves the primitive gut as a tube suspended in the primordial abdominal cavity by mesenteries
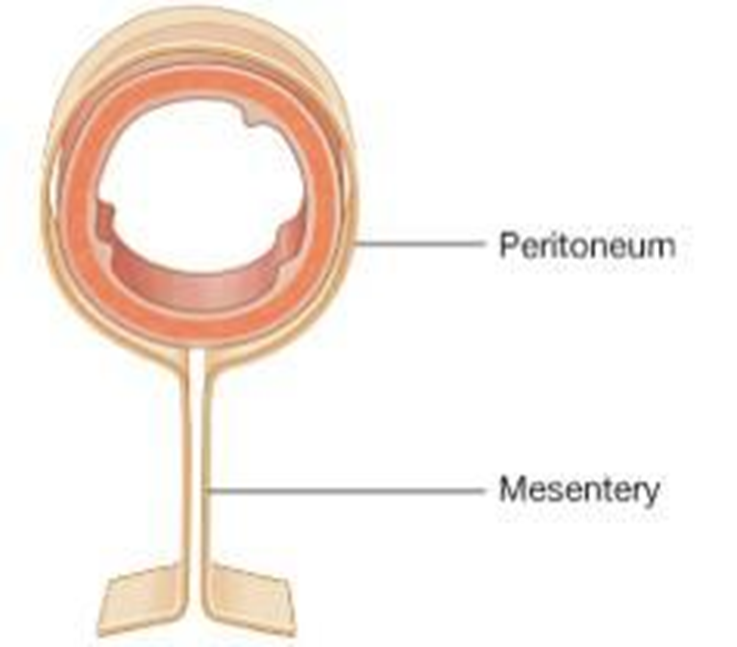
Mesenteries are formed by two layers of splanchnic mesoderm coming together
Dorsal mesentery suspends organs from the posterior body wall
Ventral mesentery suspends organs from anterior body wall
mesenteries
Dorsal mesentery: Extends from lower end of esophagus to the cloacal region of the hindgut
Ventral mesentery: Exists only in the region of the terminal part of the esophagus, the stomach, and the upper part of the duodenum
important concepts
Viscera are outside the peritoneal cavity.
The cavity normally contains a small amount of serous fluid.
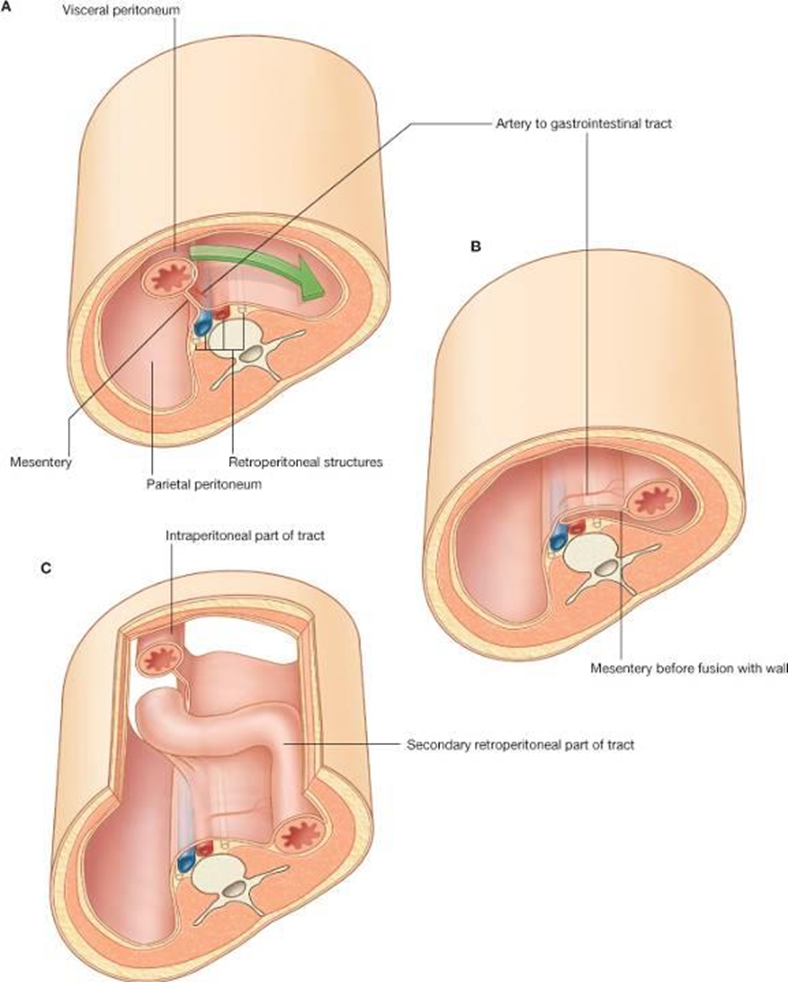
Organs described as peritoneal or intraperitoneal are surrounded or nearly surrounded by visceral peritoneum.
Retroperitoneal organs are only covered by peritoneum on their anterior surfaces.
Secondarily retroperitoneal organs lose their mesenteries during development as they are pushed against the posterior body wall.
GI tract development pushes some organs against the posterior body wall. The splanchnic peritoneum fuses with the parietal peritoneum of the posterior body wall.
The organ is then attached to the posterior body wall and is said to be secondarily retroperitoneal.
clinical note
Ascites is an abnormal accumulation of fluid in the peritoneal cavity
It is a type of edema
Patient will have a fluid wave when one presses on one side of the abdomen
Fluid can be sampled by paracentesis
Because the visceral peritoneum is thin and very vascular, drugs can be injected intraperitoneally (IP) for rapid delivery.
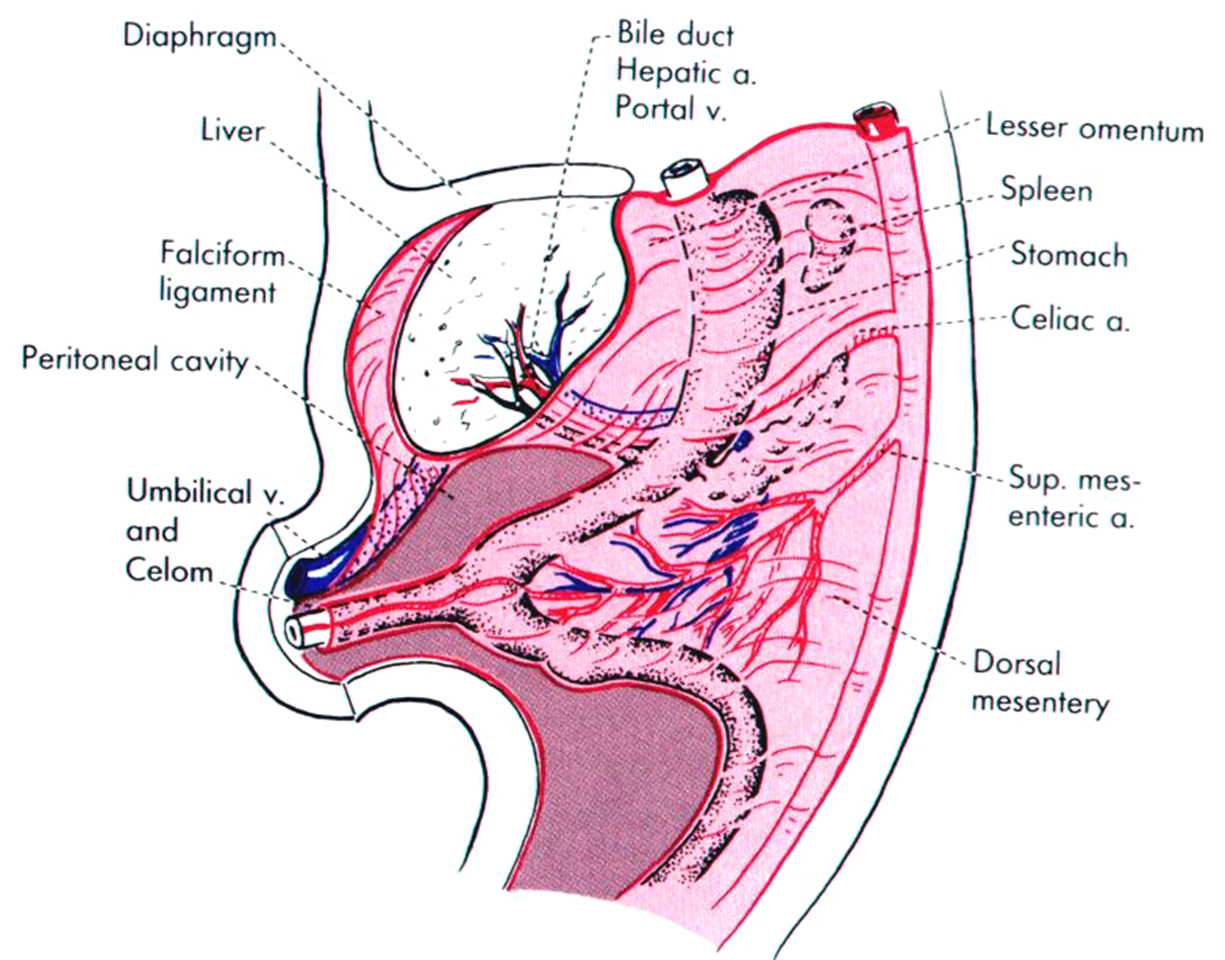
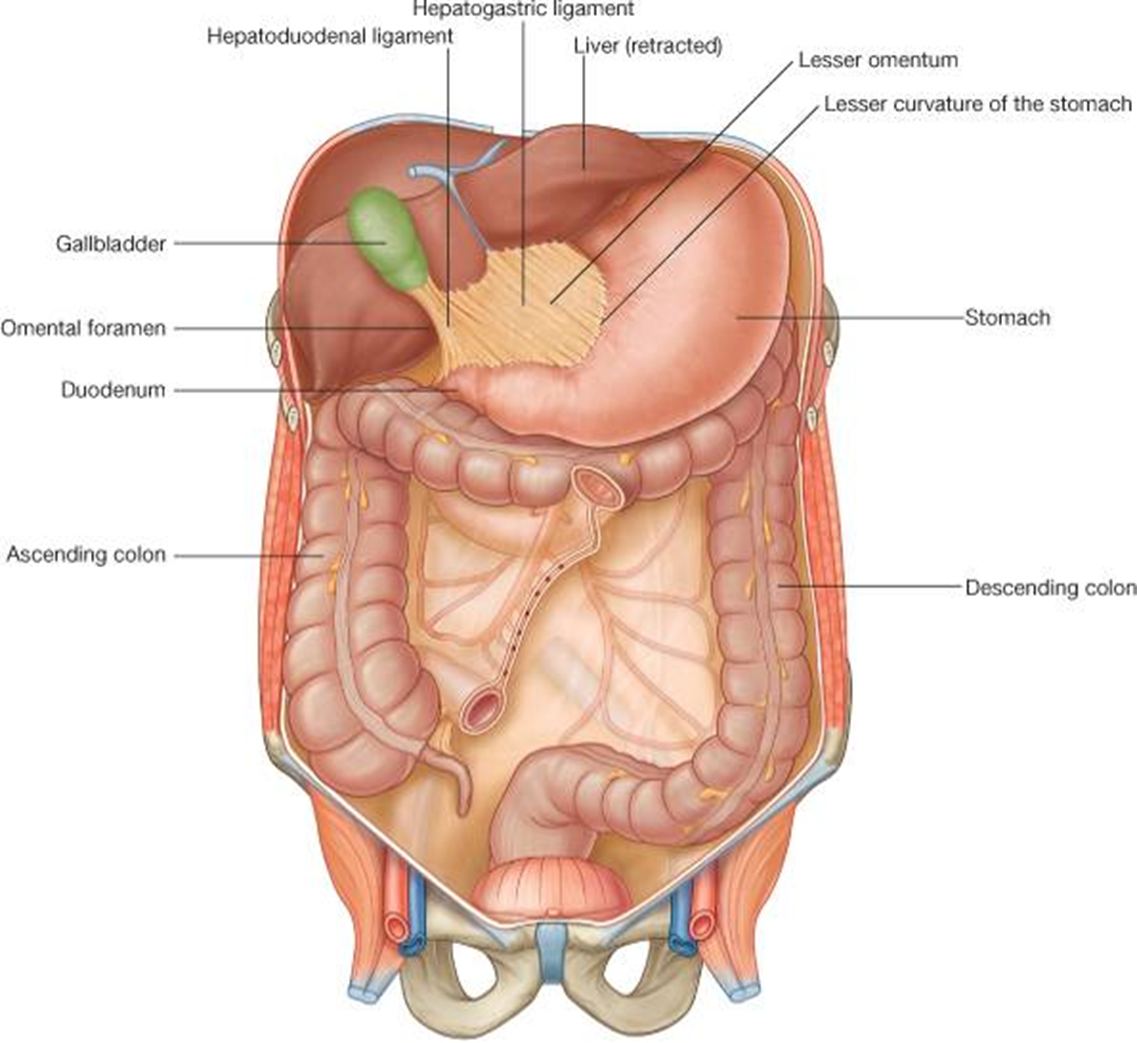
ventral mesentery
Remains only in region of stomach and proximal duodenum (caudal foregut)
The only adult remnants or derivatives are:
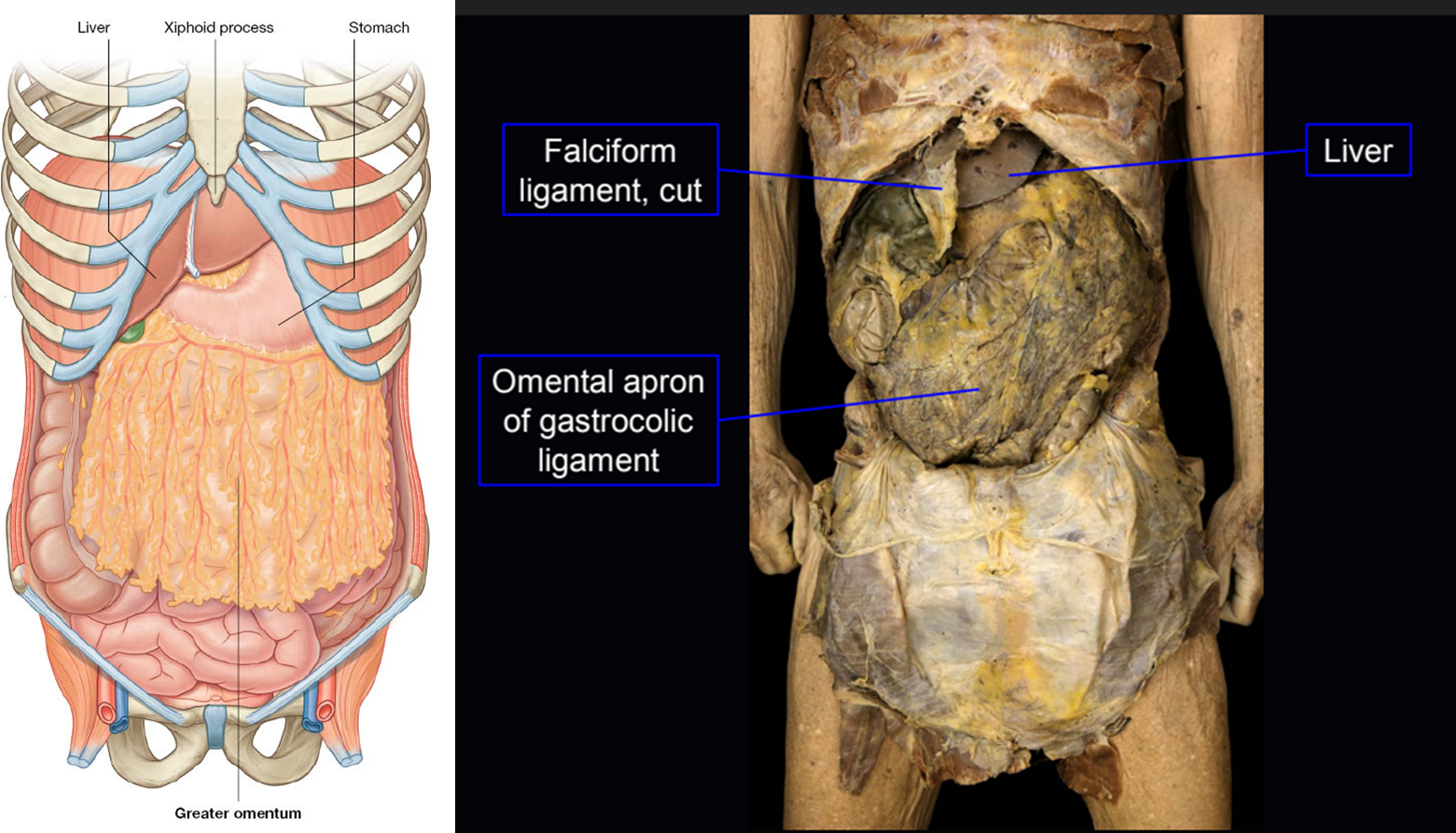
Falciform ligament: Contains, in its free edge, the ligamentum teres of the liver which is the obliterated left umbilical vein
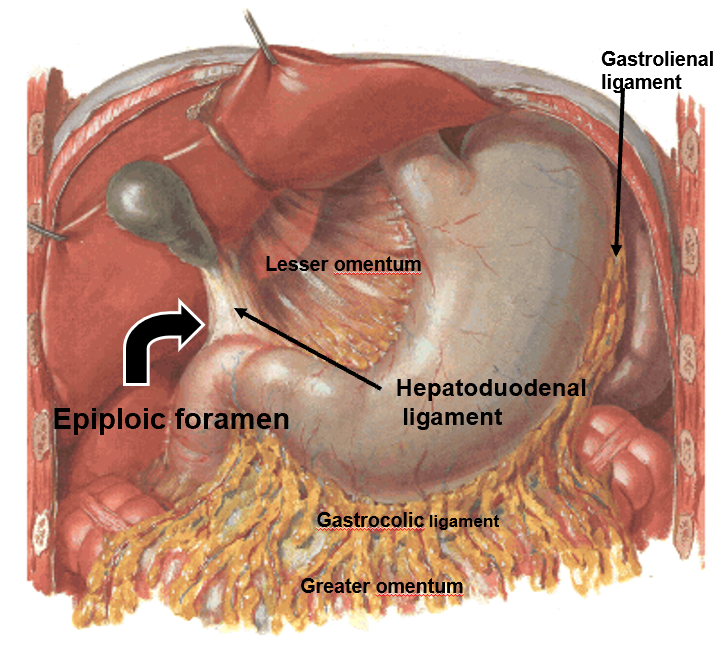
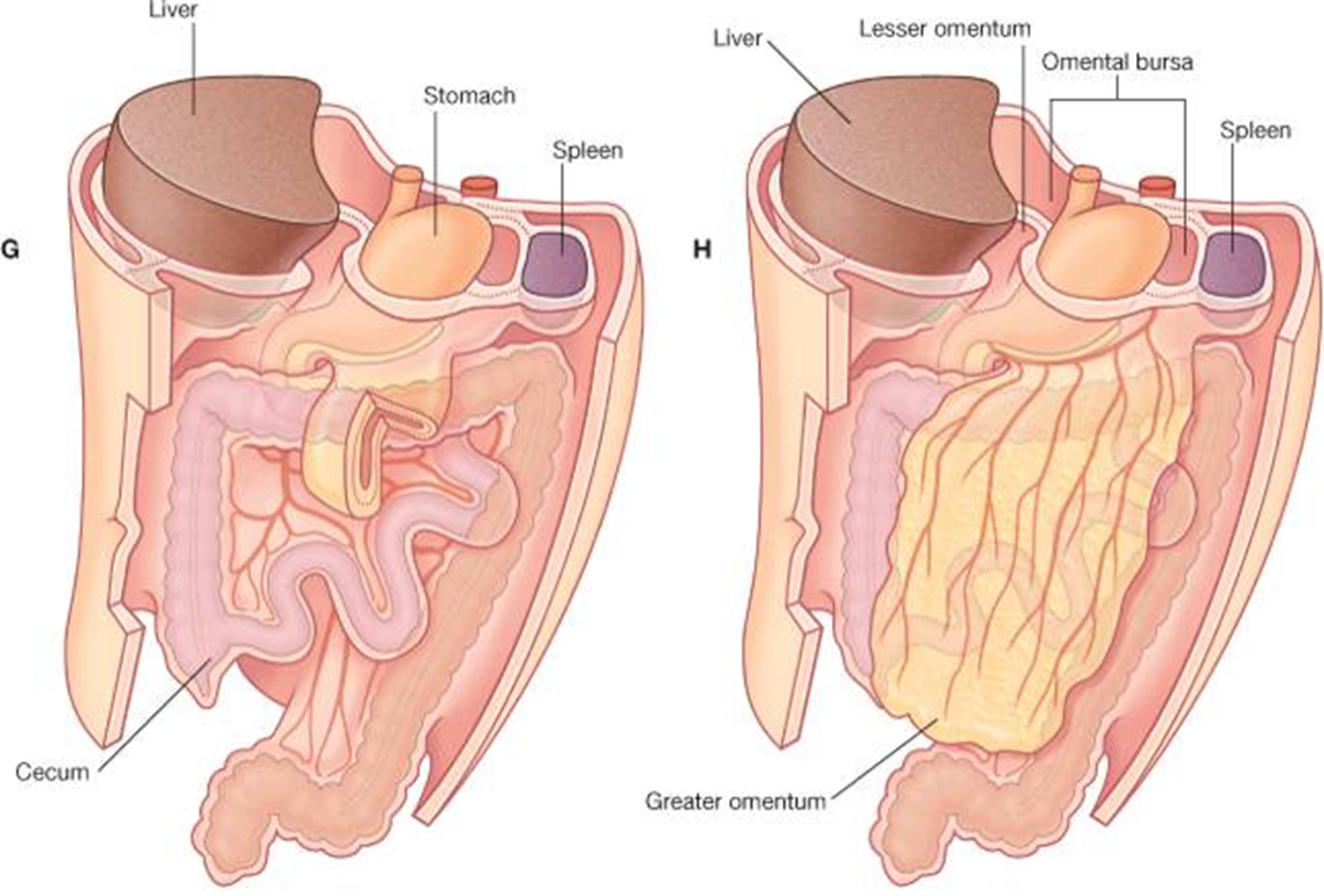
Lesser omentum: Free margin is the hepatoduodenal ligament which houses the hepatic artery, common bile duct and the portal vein
clinical note: peritonitis
Bacteria enter the peritoneal cavity by trauma, during laparotomy, or after rupture of a viscus, such as the appendix.
Patients commonly lie with knees flexed to relax muscle of the anterolateral wall.
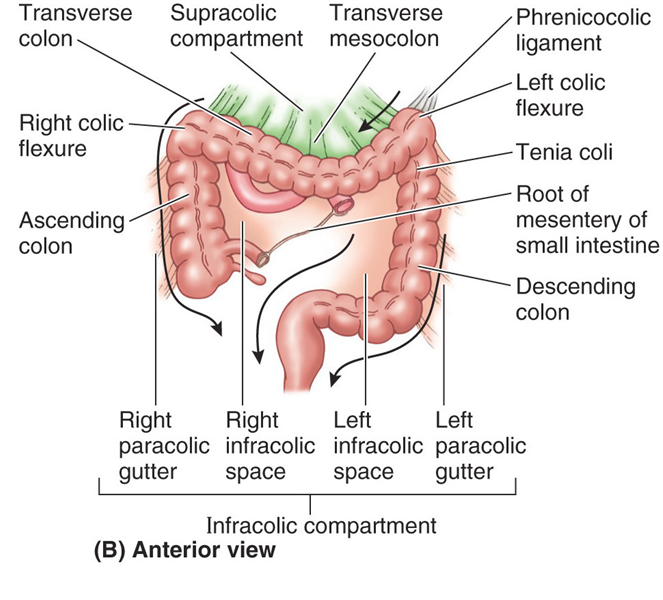
Infectious fluid can spread via the paracolic gutters.
Patients with peritonitis used to be placed in a sitting position (Fowler’s position) to cause flow of infectious fluid to the pelvic cavity where absorption of toxins is slower.
Peritoneointestinal reflex results from irritation of peritoneum and causes intestinal paralysis.
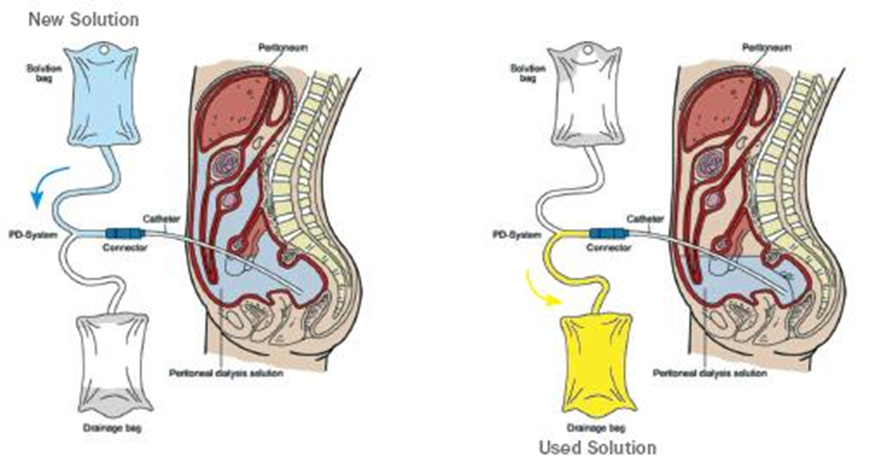
clinical note: peritoneal dialysis
Peritoneum has a large surface area, overlies blood vessel and lymphatics and is a semi-permeable membrane.
In renal failure, waste products, such as urea can be dialyzed by infusing the peritoneal cavity with a dialysis solution, which then can be removed after waste products have diffused from the blood into the peritoneal cavity.
dorsal mesentery
Carries blood vessels to and from the gut
Remnants or derivatives include:
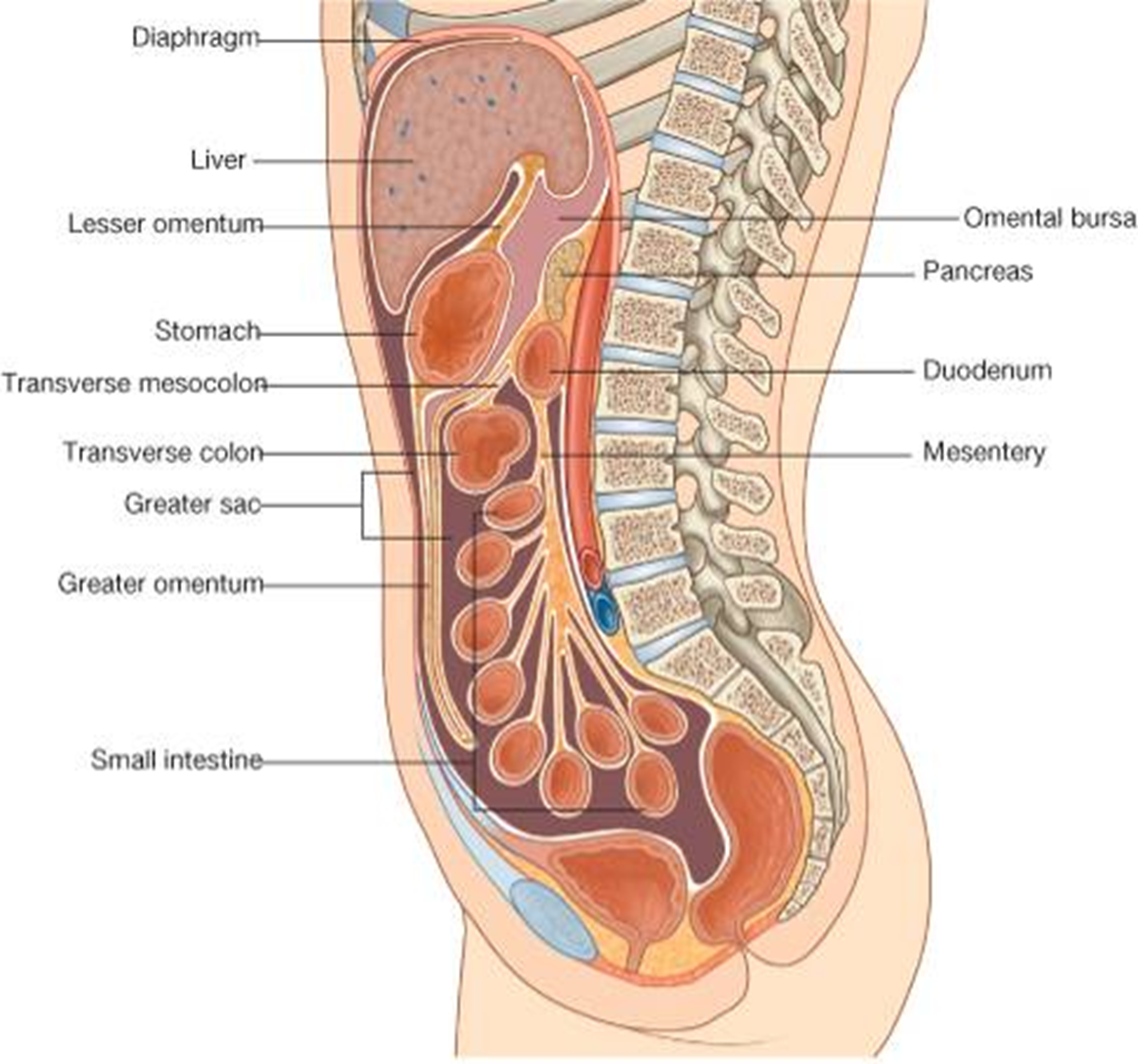
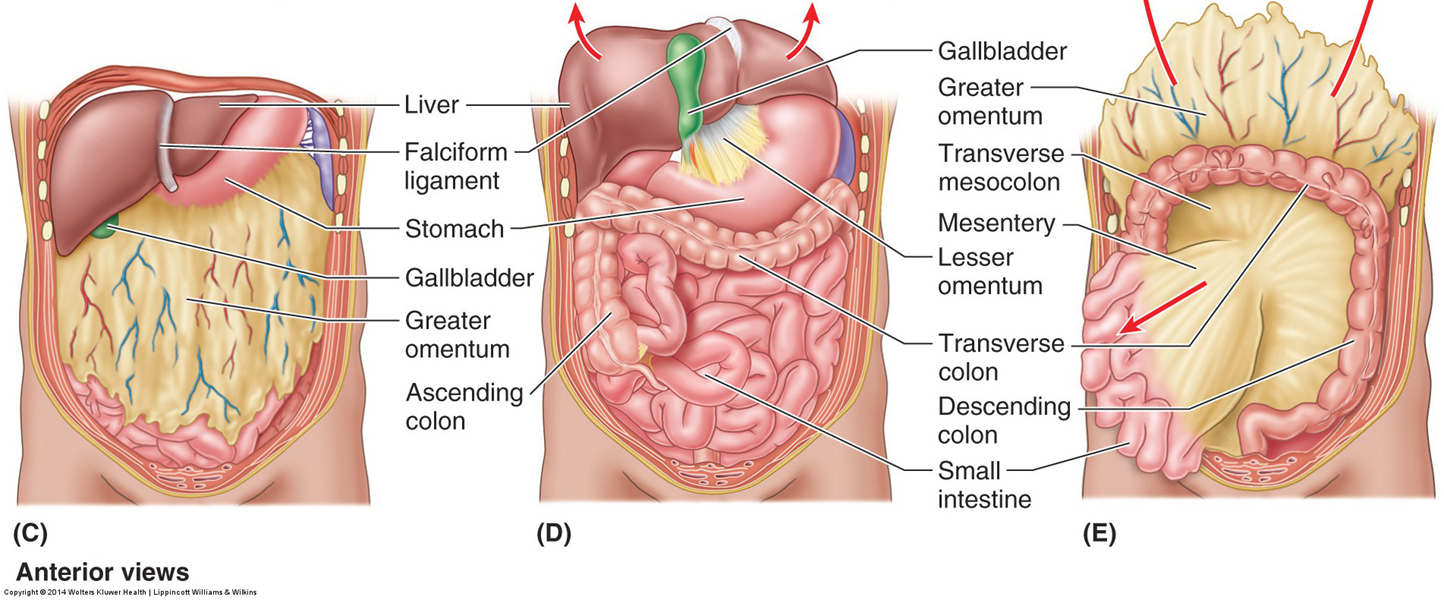
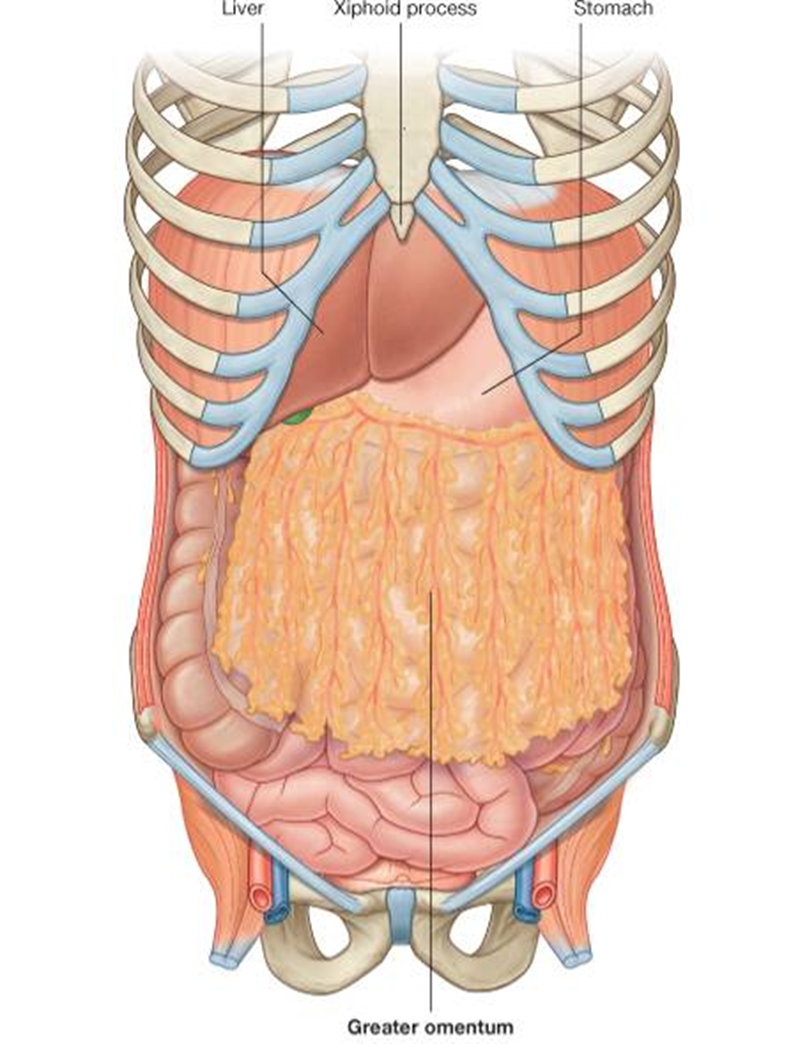
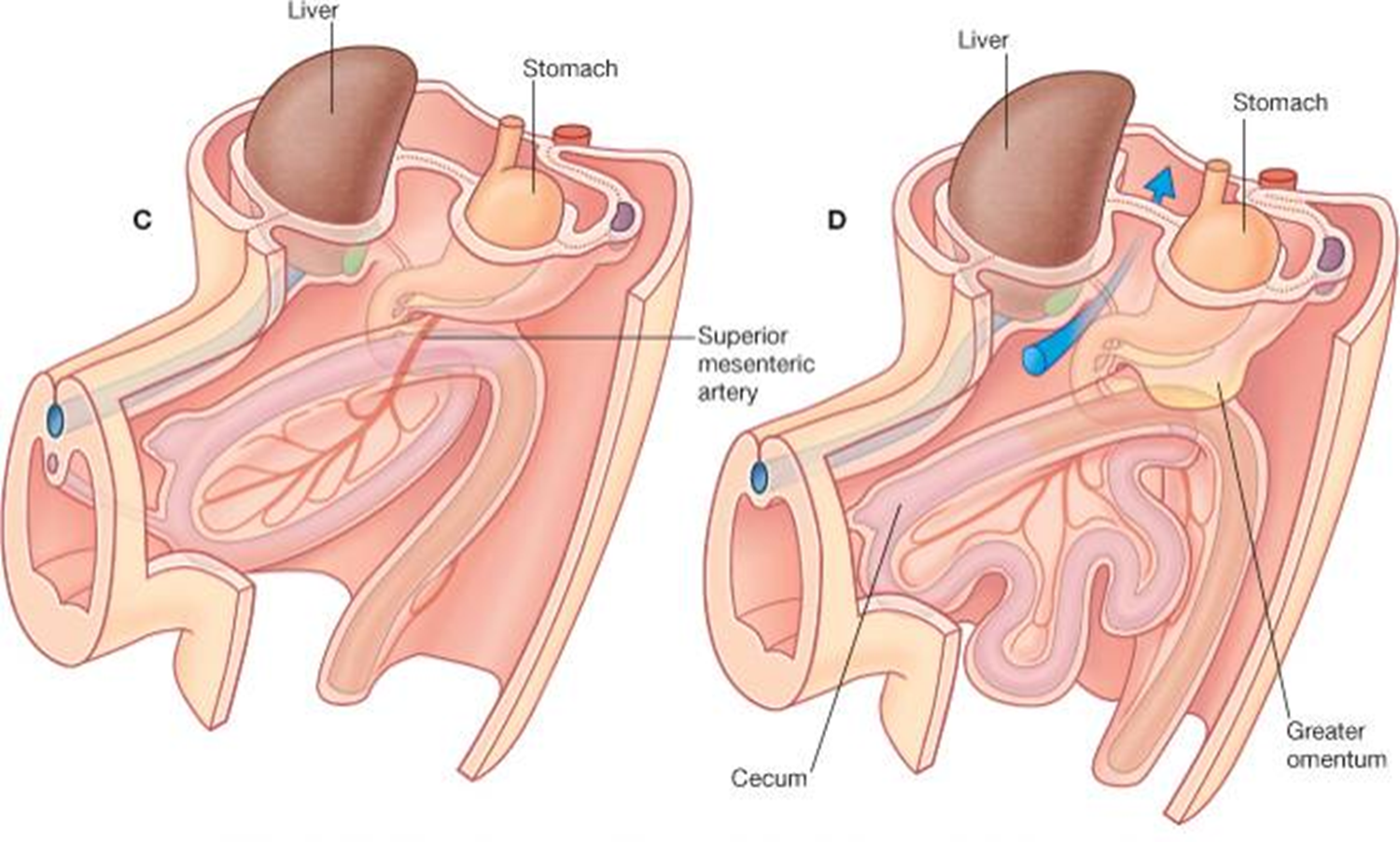
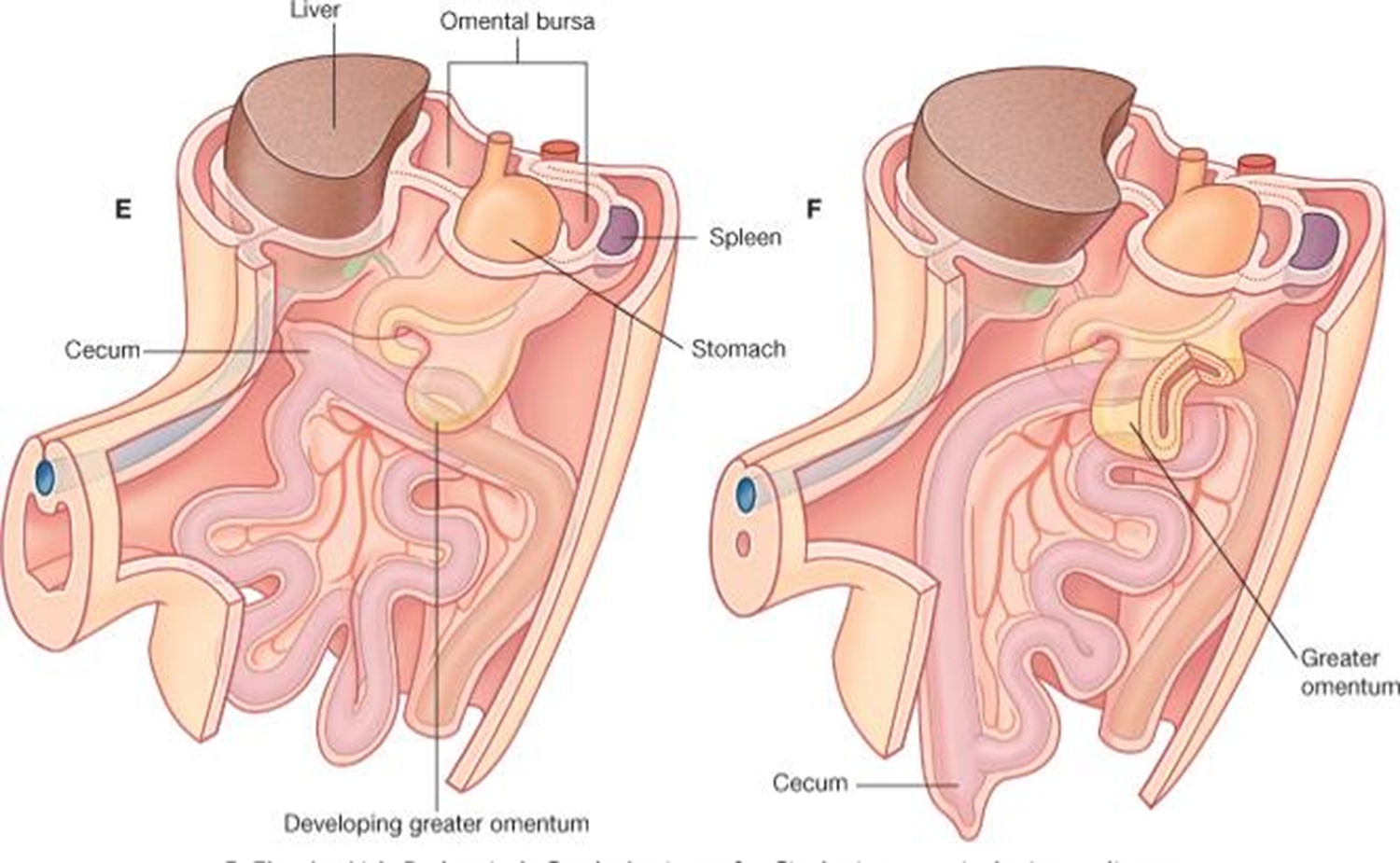
Greater omentum
Gastrocolic ligament – portion of greater omentum attaching the greater curvature of the stomach to the transverse colon
Gastrolienal –attaches stomach to spleen
Lienorenal – attaches spleen to left kidney
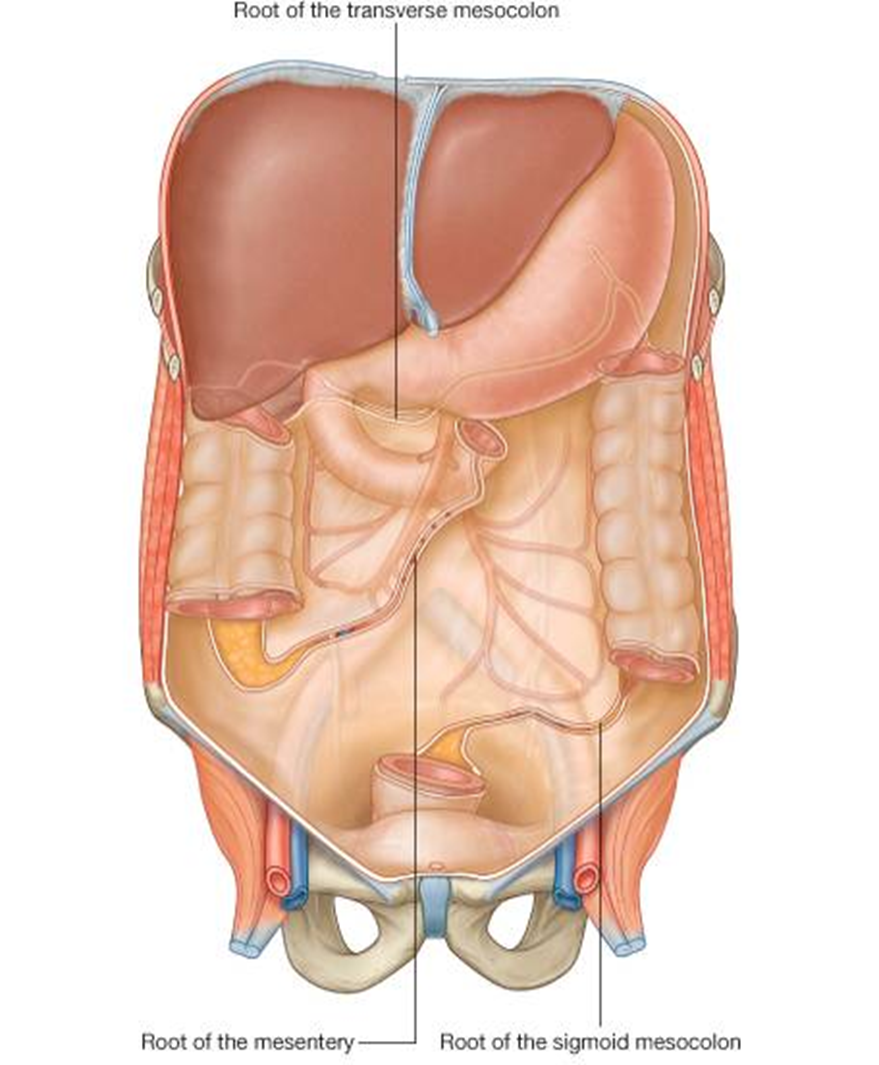
Mesentery of the small intestines (jejunum and ileum) –mesentery proper
Complex because of 270° counter-clockwise rotation of midgut
Sigmoid mesocolon
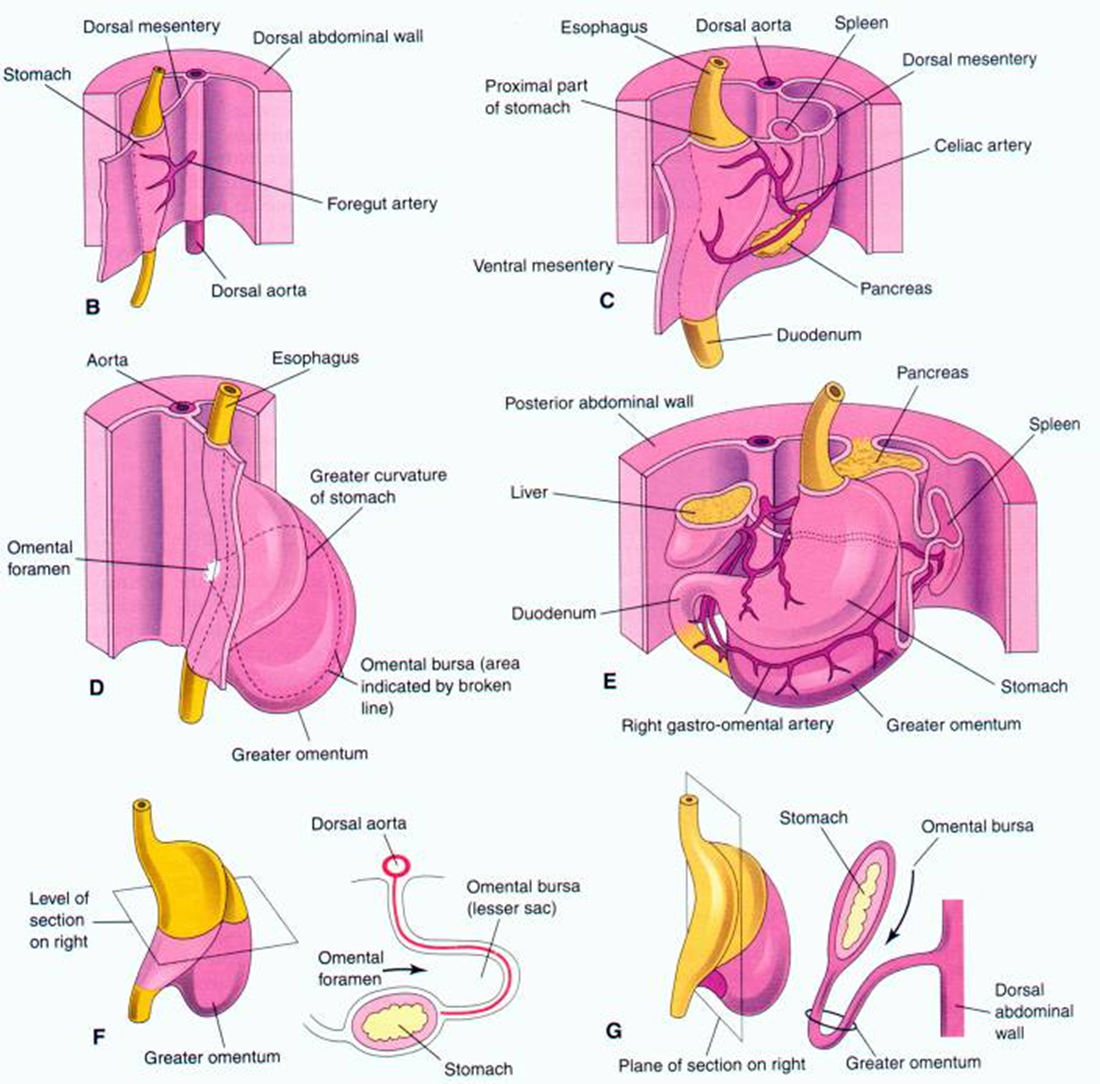
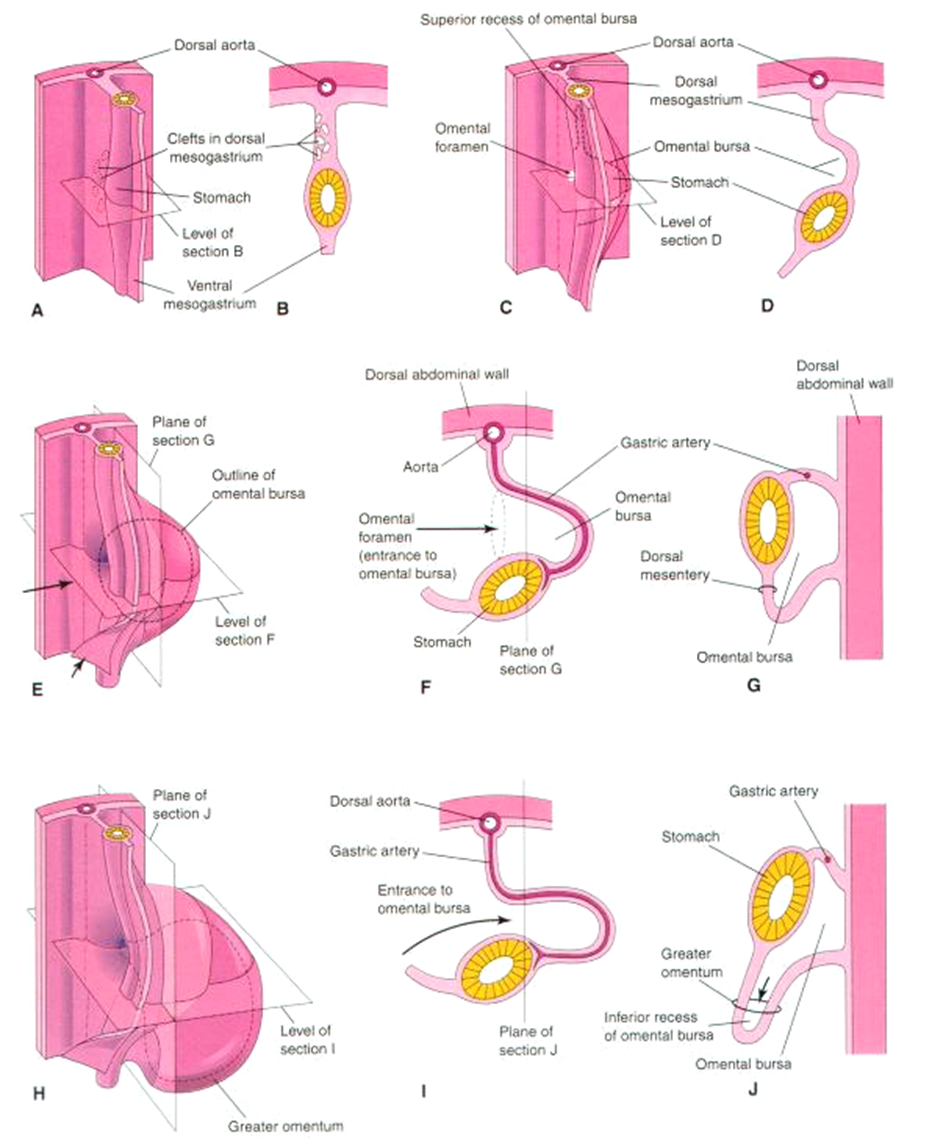
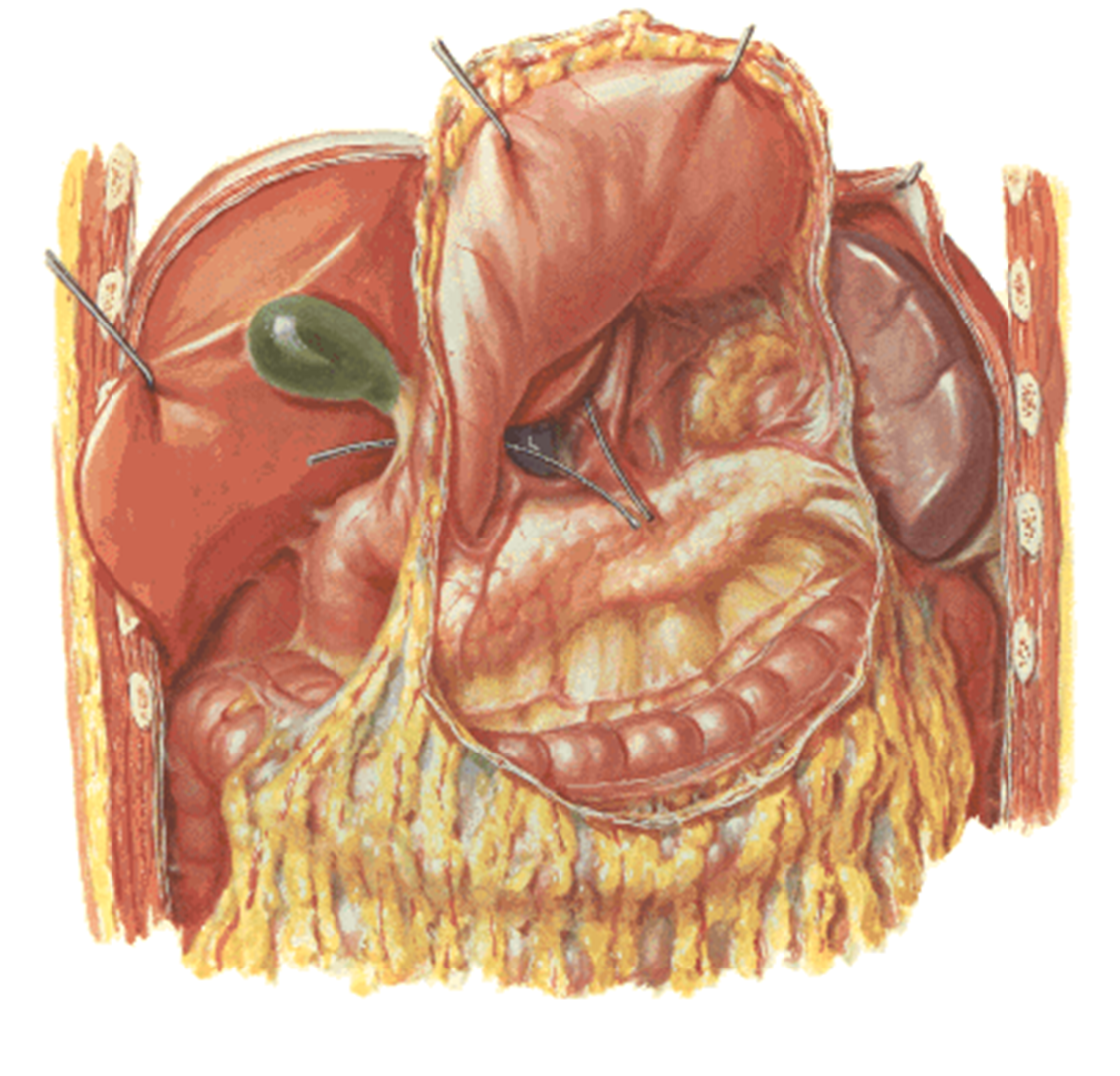
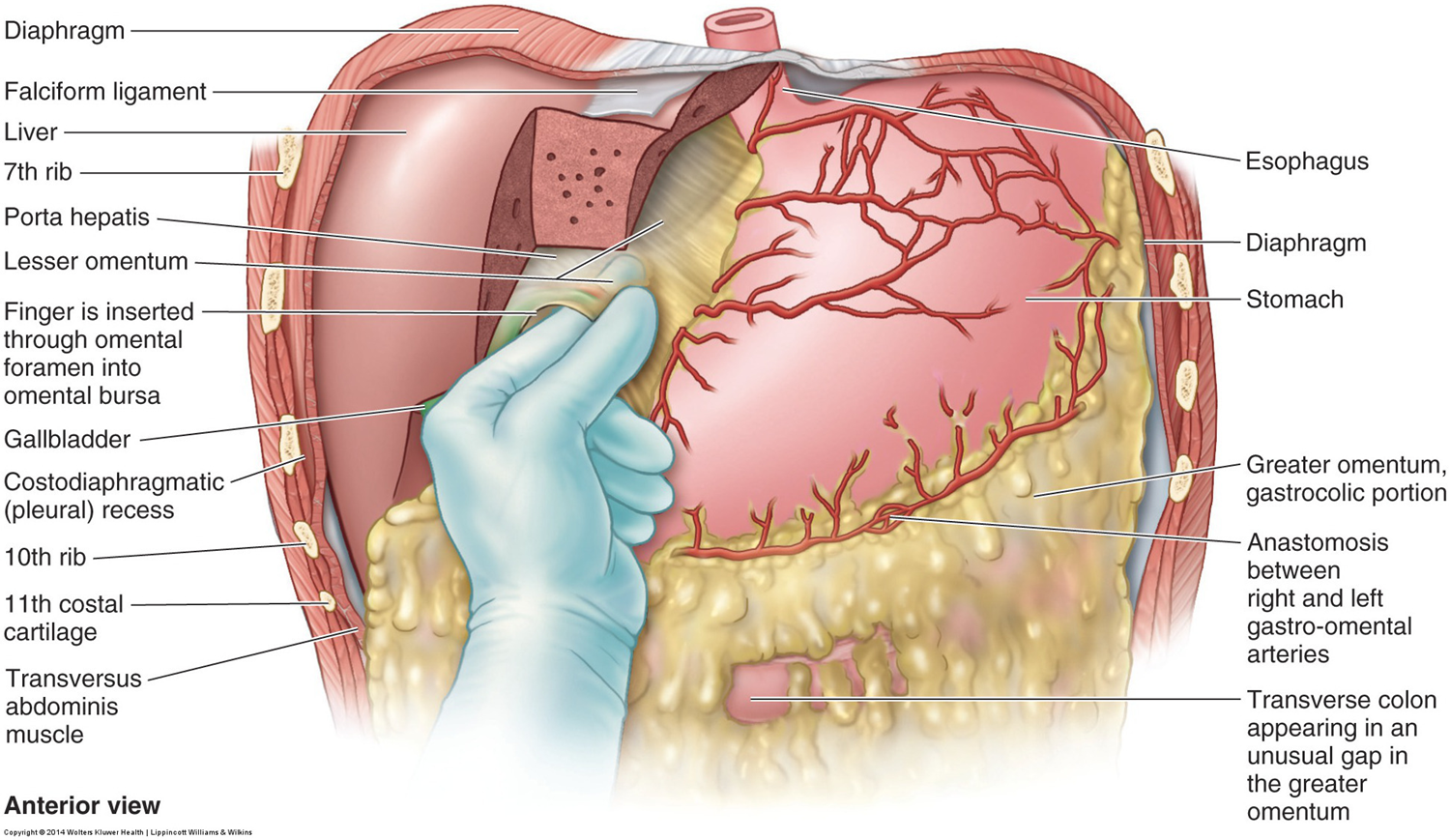
omental bursa
Lies posterior to the stomach
Superior recess – limited by diaphragm and posterior layers of the coronary ligament of the liver
Inferior recess – potential space between the layers of the greater omentum
Function – allows free, smooth movement, of the stomach over the structures that lie posterior and inferior to it.
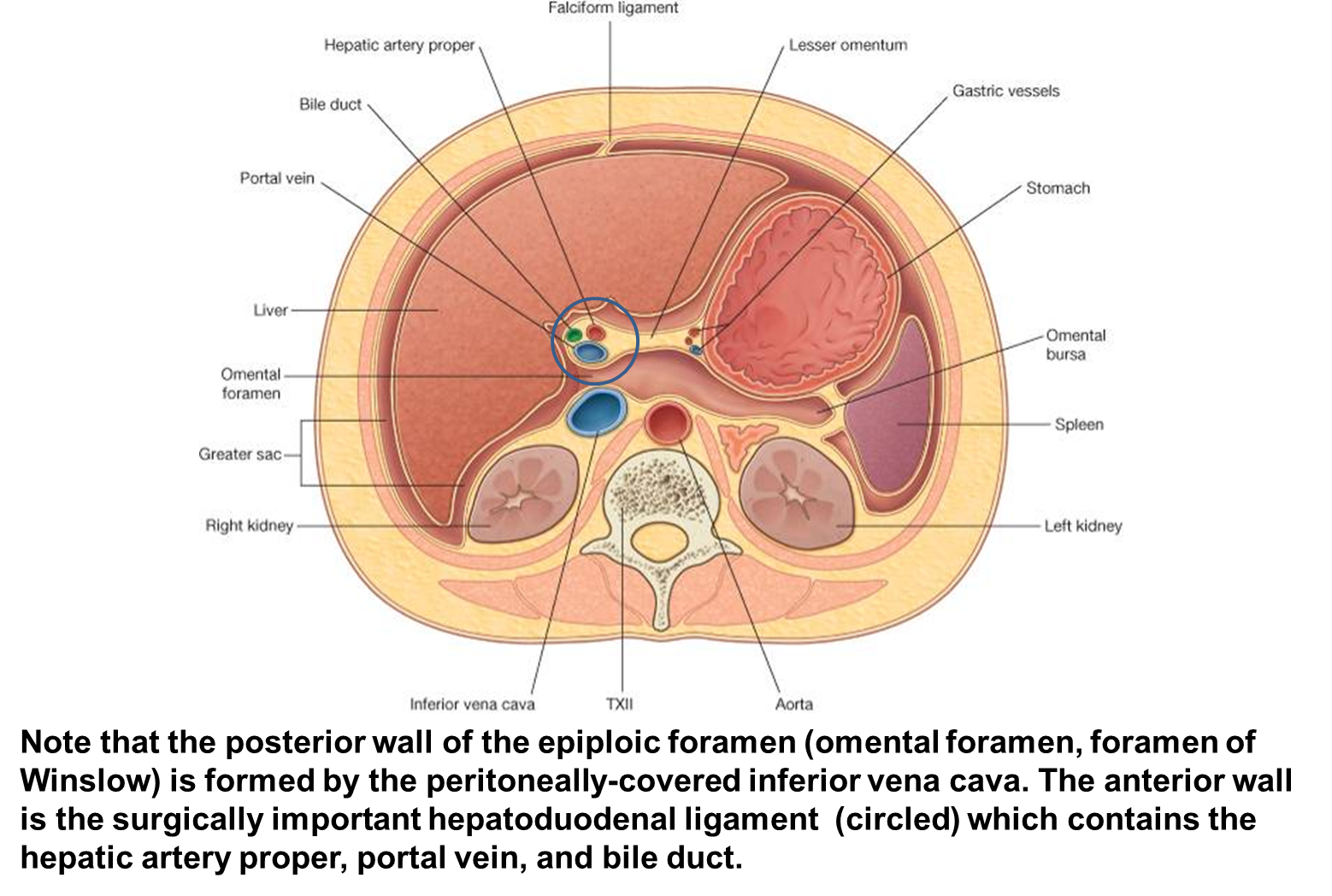
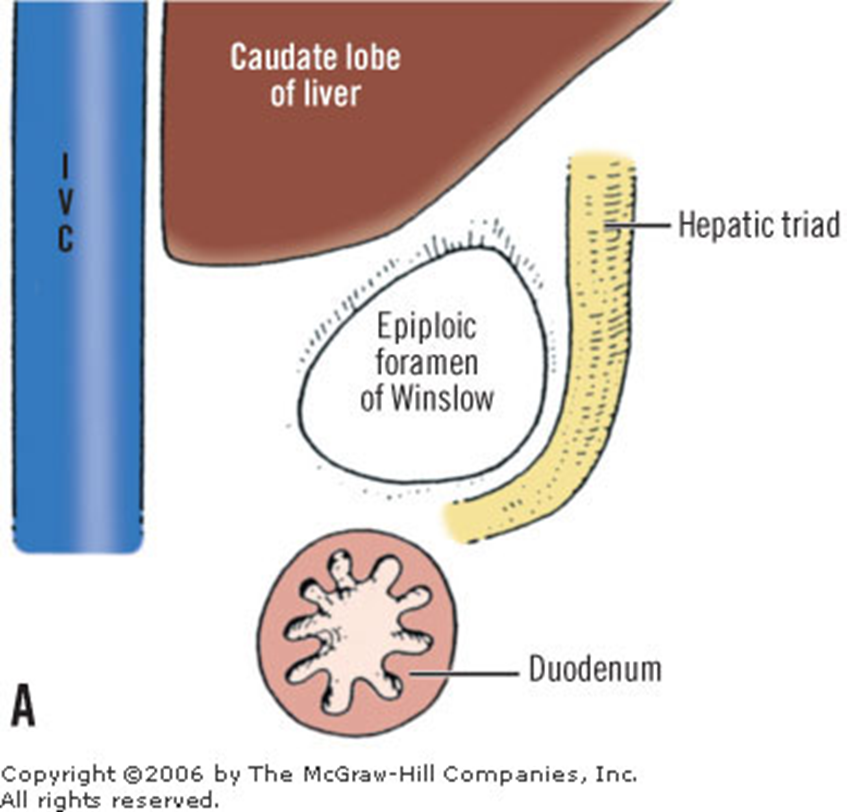
boundaries of foramen of winslow
Anterior: Hepatoduodenal ligament
Posterior: Inferior vena cava
Superior: Caudate lobe of liver
Inferior: 1st part of duodenum
clinical note: omental bursa
The omental bursa or lesser sac can fill with fluid as a result of ulceration of the posterior wall of the stomach or as a result of pancreatitis
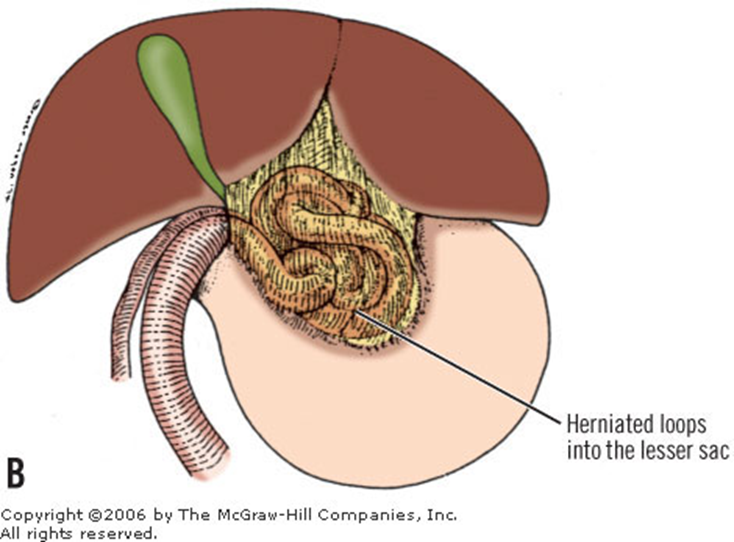
Rarely, a loop of bowel can herniate into the foramen of Winslow causing strangulation and necrosis of the bowel
omental bursa formation
Differential growth of the stomach, rotation of the stomach, and extensive growth of the dorsal mesogastrium (mesentery), which forms the greater omentum and related structures, contribute to the formation of the lesser sac
gut rotation
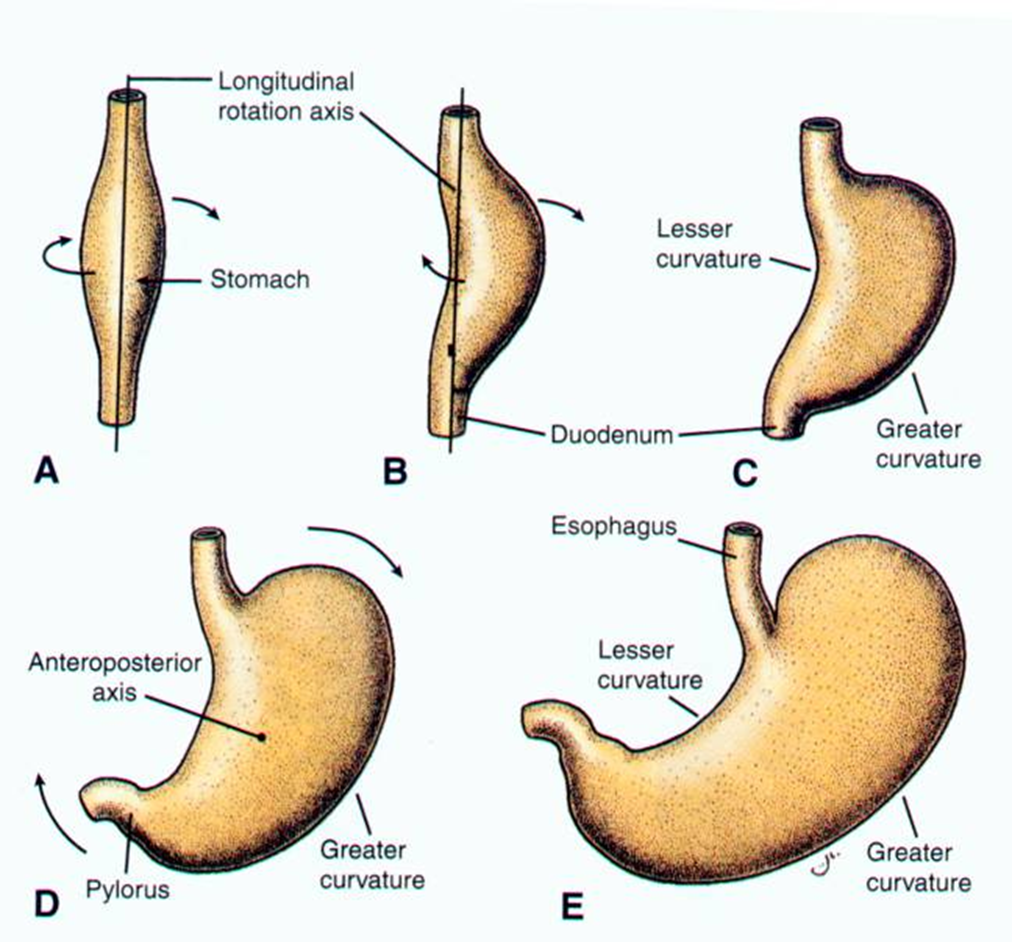
development of stomach
The distal part of the foregut begins as a simple tube.
During the 4th week, it begins to dilate and become fusiform.
It enlarges and broadens in the median plane.
Over the next two weeks, its dorsal border grows more rapidly than its ventral border.
stomach rotation
As the stomach grows, it rotates slowly, 90° clockwise around its longitudinal axis
During rotation and growth, the cranial region moves to the left and inferiorly
The caudal region moves to the right and superiorly