AST - Skin Lesions
Eyelids Anatomy and Tumours
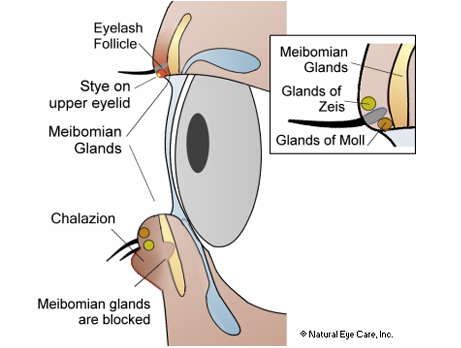
Eyelid Structure:
Benign tumours / growths
Cysts of the Eyelid
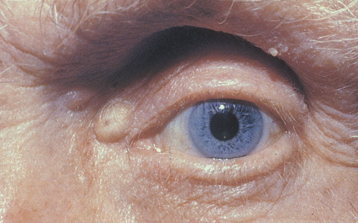
Cyst of Zeiss:
Description: Small, non-translucent cysts located on the anterior lid margin, resulting from modified sebaceous glands.
Characteristics: small, non-translucent cyst on anterior lid margin, often non-tender

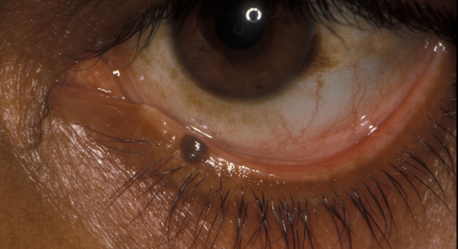
Cyst of Moll:
Description: Modified apocrine sweat gland cyst.
Aprocrine hidrocystoma
small retention cyst
Characteristics: Small, round, translucent; fluid-filled and usually more common in the lower lid.
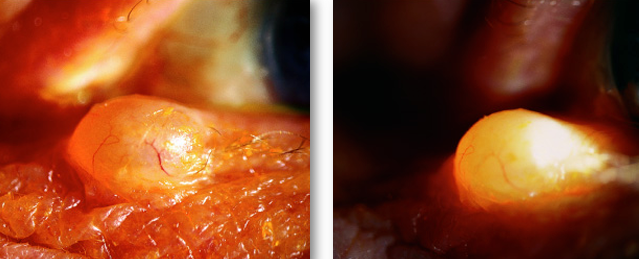
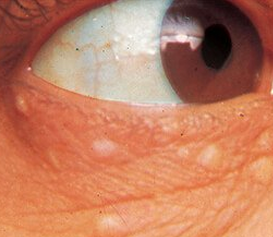
Eccrine Hidrocystoma:
Location: Found on the medial or lateral aspects of the eyelid, usually doesn’t involve lid margins.
fluid filled - will light up with slit lamp beam
similar to cyst of Moll
don’t usually self-resolve - cosmetic excision
bilateral, can be numerous
Sebaceous Cysts:
Arise from sebaceous glands
Central punctum with retained “cheesy secretion”
rarely found on eyelids, may occur at inner canthus.
can be massaged or squeezed.
Acne-Related Lesions
Comedones:
acne vulgaris
plug of keratin and sebum within dilated opening of hair follicle
if follicle open = blackhead: plug of melanin containing keratin
if follicle closed = whiteheads: cream coloured papules
common in older patients
don’t cause any significant problems

Milia:
occlusion of pilosebaceous units (hair follicles and associated sebaceous gland)
results in retention of keratin
tiny epidermoid cysts
white, round, superficial papules, usually in groups
typically seen in young children / infants
usually self resolving

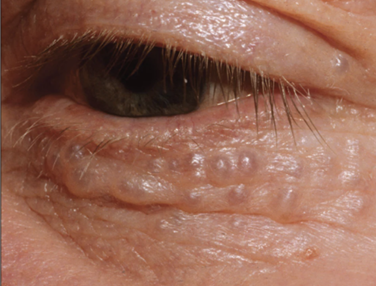
Syringoma
proliferation of intraepidermal sweat gland epithelium
multiple small papules
randomly distributed
don’t require any intervention
Infective Lesions
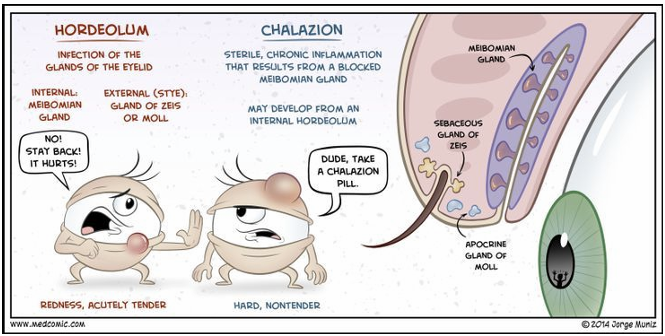
Hordeolum (Stye):
Internal: Infection of Meibomian gland.
External: Infection of glands of Zeis or Moll.
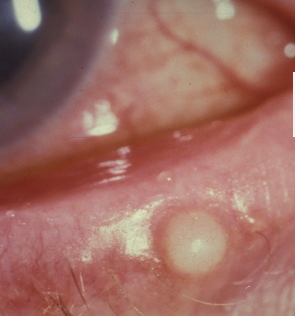
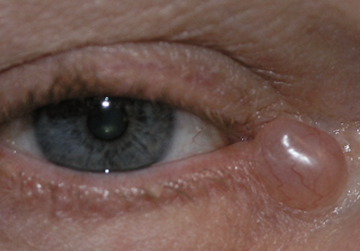
Chalazion:
Sterile inflammation due to blocked Meibomian gland, may evolve from an internal hordeolum.
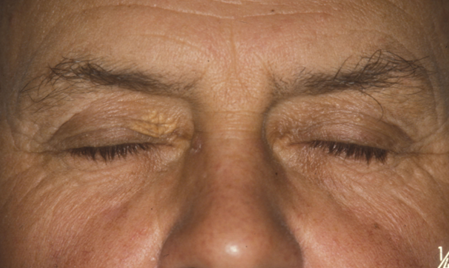
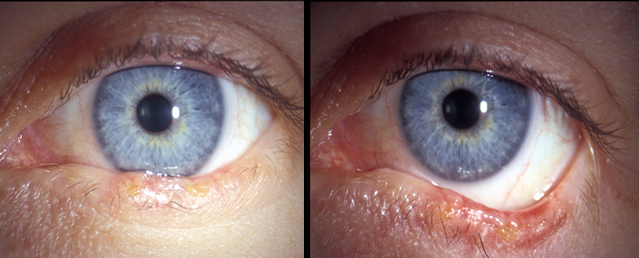
Xanthelasma:
common, often bilateral
middle aged to elderly patients
multiple yellowish subcutaneous plaques - lipid laden histiocytes in epidermis
most commonly at nasal aspect of lids
treatment for cosmetic reasons
may be associated with raised serum cholesterol and LDL cholesterol
high recurrence rate in patients with persistent elevated cholesterol.
increased risk of heart disease, heart attack within 10 years.
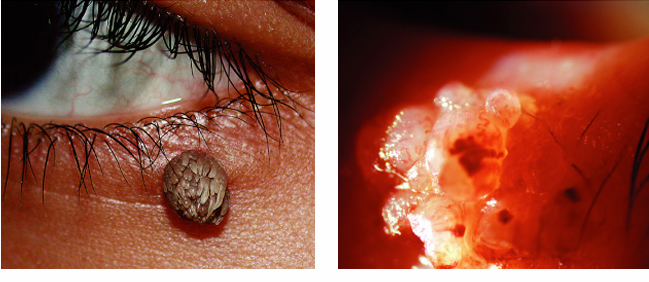
Squamous Papilloma
“skin tag”
very common
pedunculated: fresh coloured narrow based pedunculated lesion (skin tag)
Sessile: broad based flatter lesion
hyperkerotic filform lesion like a cutaneous horn
excision if necessary.


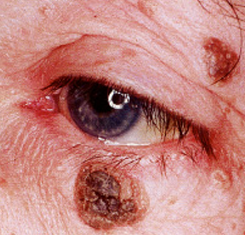
Seborrhoeic Keratosis
Basal Cell papilloma
Common and slow growing lesion found on face, trunk and extremities of elderly patients.
greasy looking brownish plaque with a verruca looking surface
looks stuck on to skin
treatment by excision (usually for cosmetic reasons)
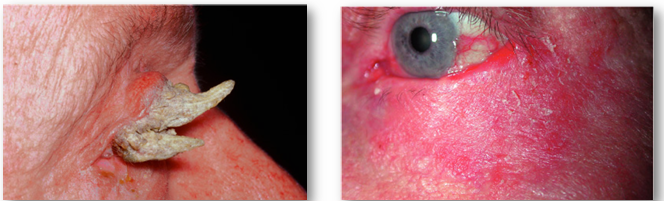
Actinic Keratosis
also called solar keratosis
common pre-malignant skin lesions
rare on eyelids
affects elderly faire skinned people with excessive amounts of sunlight exposure.
forehead & back of hands
flat, sclay hyperkeratotic lesions
may be nodular or wart-like
may be associated with cutaneous horn
Reasons for excision:
can develop into a skin cancer
often cosmetically problematic
cause changes to the architecture of the lids.
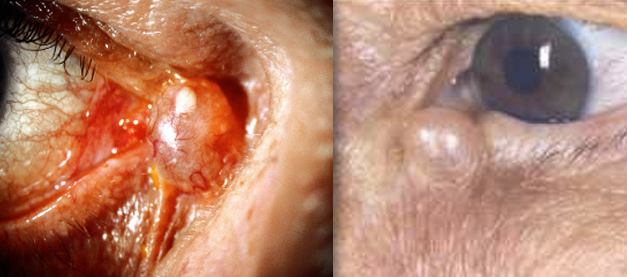
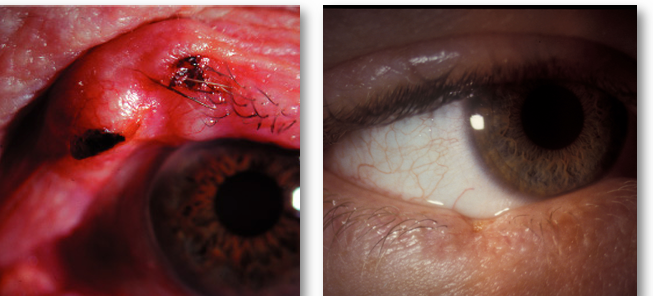
Pyogenic granuloma
fast growing vascularised proliferation of granulomatous tissue
follows surgery, trauma or infection
especially pterygium surgery
pink pedunculated or sessile mass
excised.
non-cancerous
normally arise from conjunctiva

Keratocanthoma
rapidly growing benign tumour
fair skinned individuals with chronic sun exposure
found frequently in immunosuppressed px following renal transplants
may resemble squamous cell carcinoma
pink papule which may rapidly increase in size in few days
usually stops growing and remains static for 2-3 months
end of growth phase is firm dome shaped nodule
may spontaneously involute
in regression central part becomes hyperkeratotic with possible keratin filled crater.
involution may take up to a year and leave a scar

Capillary Haemangioma
“Strawberry naevus”
demographic
common tumour of infancy
more common in females
may be familial tendency
signs / symptoms:
predilection for upper lid, possible orbital involvement
unilateral red raised lesion
blanches with pressure
mechanical ptosis possible
can cause amblyopia in young age group
usually grows quickly in first year life, and may resolve spontaneously around age 2
complete resolution by 4 in 40%, 70% by age 7
patients with large fast growing strawberry naevi:
Kasabch-Merritt syndrome – thrombocytopenia, anaemia and low coagulant factor levels
Maffuci syndrome – skin haemangiomas, enchrondromata of hands feet and long bones, bowing of long bones
treatment: treatment if vision threatened by amplyopia, ptosis or strabismus, steroid injection into tumour, beta blocking systemic medication (e.g., timolol gel)

Malignant Tumours
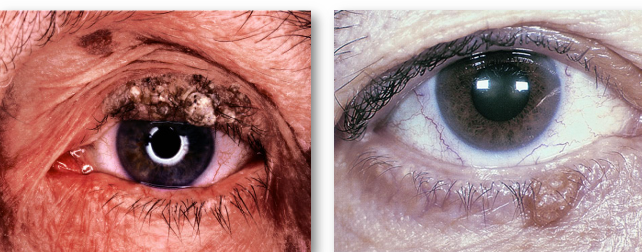
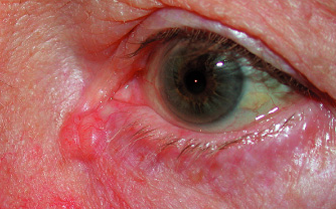
Basal Cell carcinoma
most common human malignancy
most frequently affects elderly patients
important risk factors:
fair skin
inability to tan
chronic exposure to sun
slow growing
frequent locations (most to least)
lower lid, medial canthus, upper lid, temporal canthus
90% occur in head and neck
10% involve eyelid
BCC in medial aspect more likely to invade orbit and sinuses, also more likely to reoccur
recurrent tumours following incomplete treatment more aggressive and harder to manage.
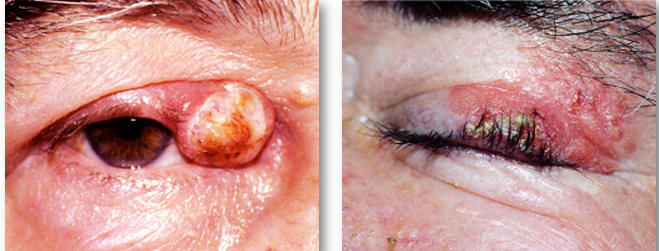
Nodulo-ulcerative BCC
shiny firm pearly appearing nodule
dilated BVs on the surface
initially slow growing
if untreated, growth can become rapid and BCC develops central ulceration
raised rolled edges with dilated BVs over margins (rodent ulcer)
Over time may erode large portion of the lid.

Sclerosing BCC (morphoeic / morpheaform)
infiltrates laterally beneath skin as a plaque which may distort lid
may be difficult to define margins clinically
sclerosing BCC may resemble localised area of “chronic blepharitis”
can cause thickening of the eyelid and small areas of madarosis

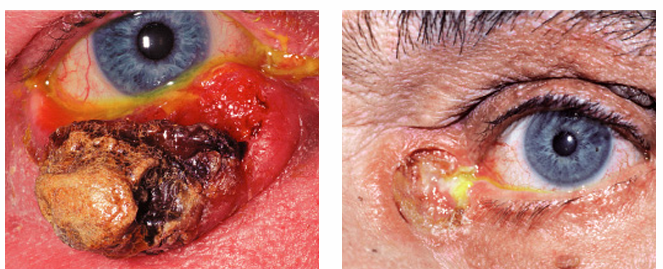
Squamous cell carcinoma (SCC)
less common but more aggressive
accounts for 5-10% of eyelid malignancies
metastasises to regional lymph nodes and can spread to intracranial cavity via orbit
may arise de novo or from pre-existing actinic keratosis
predilection for lower lid and lid margin
more common in elderly patients
risk factors: fair complexion, history of chronic sun exposure and skin damage
diagnosis is often difficult
other benign lesions may resemble SCC
keratoacanthoma may show squamous cell changes at deeper levels.
SCC may look similar to BCC
but usually no surface vascularisation
SCC has more rapid growth
Plaque like SCC: roughened scaly reddened (erythematous) hyperkeratotic plaque - may arise from existing actinic keratosis
Nodular SCC: hyperkeratotic nodule - crusty erosions and fissures may develop
ulcerating SCC: red base and sharply defined indurated and everted boarders.
treatment: surgery and radiation therapy
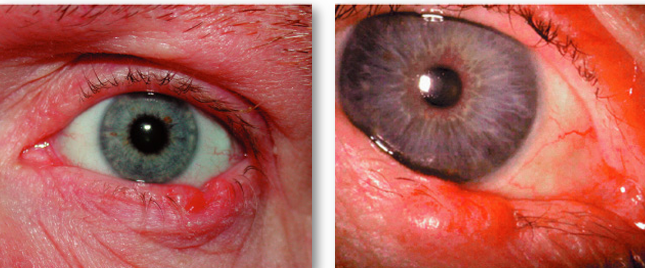
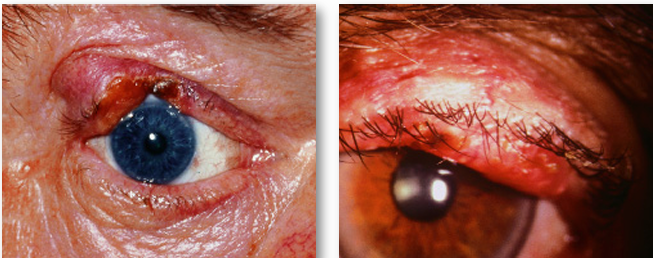
Sebaceous gland carcinoma
arises from meibomian glands, occasionally glands of Zeiss or sebaceous glands
most commonly occur on the upper lid
sometimes simultaneous involvement of both lids - intraepithelial spread or multiple primaries
early tumours may mimic less aggressive lesions (chalazion)
needs prompt treatment as it can travel through the lymphatics and bloodstream and metastasize very quickly
treatment with chemotherapy
Nodular Meibomian Gland Carcinoma
discrete, hard nodule in upper tarsal plate
NB: recurrent or non-resolving chalazion
Spreading meibomian gland carcinoma
diffuse thickening of lid margin
similar to sclerosing BCC
may invade conjunctiva
pagetoid spread: extension to palpebral, fornix or bulbar conjunctiva
misdiagnosis as chronic conjunctivitis, SLK
Suspicion index for malignancy
ulceration
lack of tenderness
induration - volcano appearance
irregular borders
destruction of lid margin architecture
loss of lashes or fine skin hairs
loss of skin pores
Other Lid tumours
Karposi Sarcoma
vascular tumour affecting AIDS patients
small tumours are pink, red-violet or brown which may resemble maemartoma or naevus
larger tumours may ulcerate and bleed

Merkel Cell carcinoma
fast growing tumour arising from Merkel cells in dermis
elderly patients
highly malignant and potentially lethal
frequent metastatic spread at diagnosis

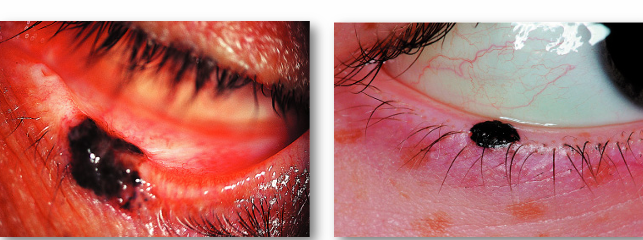
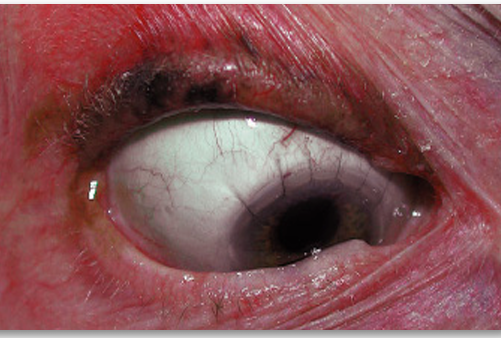
Pigmented lesions
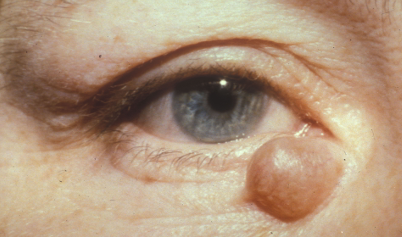
Intradermal Naevi
usually elevated and often papillomatous in appearance
maybe non-pigmented or brown-black
lashes may grow through if on margin
“kissing” naevi: symmetrical lesions on upper and lower lids
naevus cells are in dermis and no malignant potential
Junctional Naevi:
flat, well circumscribed and uniform colour
cells located at junction of epidermis and dermis
low potential for malignant transformation
Compound Naevi:
intradermal and junctional components
usually brownish
low malignant potential due to junctional component
Management of Naevi:
document
size, location
photograph
educate patient
refer if “nervous”
Melanoma
rare on eyelids - but potentially lethal
skin melanomas pigmented but lid melanomas may be clinically non-pigemented.
superficial spreading melanoma: plaque with irregular outline and variable pigmentation
nodular melanoma: blue-black nodule surrounded by normal skin
lentigo maligna: slowly expanding pigmented macule which affects elderly patients most commonly.
Hutchinson freckle
sometimes associated with melanoma development.
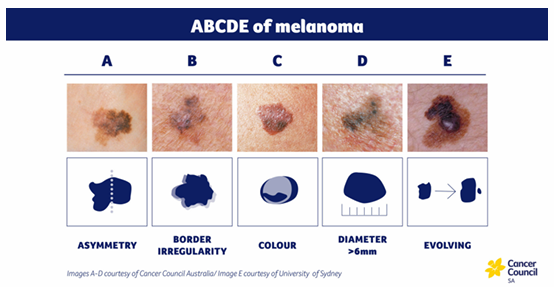
ABCDE of Melanoma:
A: Asymmetry
B: Border irregularity
C: Colour variation
D: Diameter (>6mm)
E: Evolving nature