W11
Understand the difference between an MHCI and MHCII, which cells would possess each, and what type of receptor they bind to
MHC I
Binds CD8 receptor
Tc
found on all nucleated cells (except RBCs)
Presents endogenous antigens
MHC II
Binds CD4 receptor
H.T
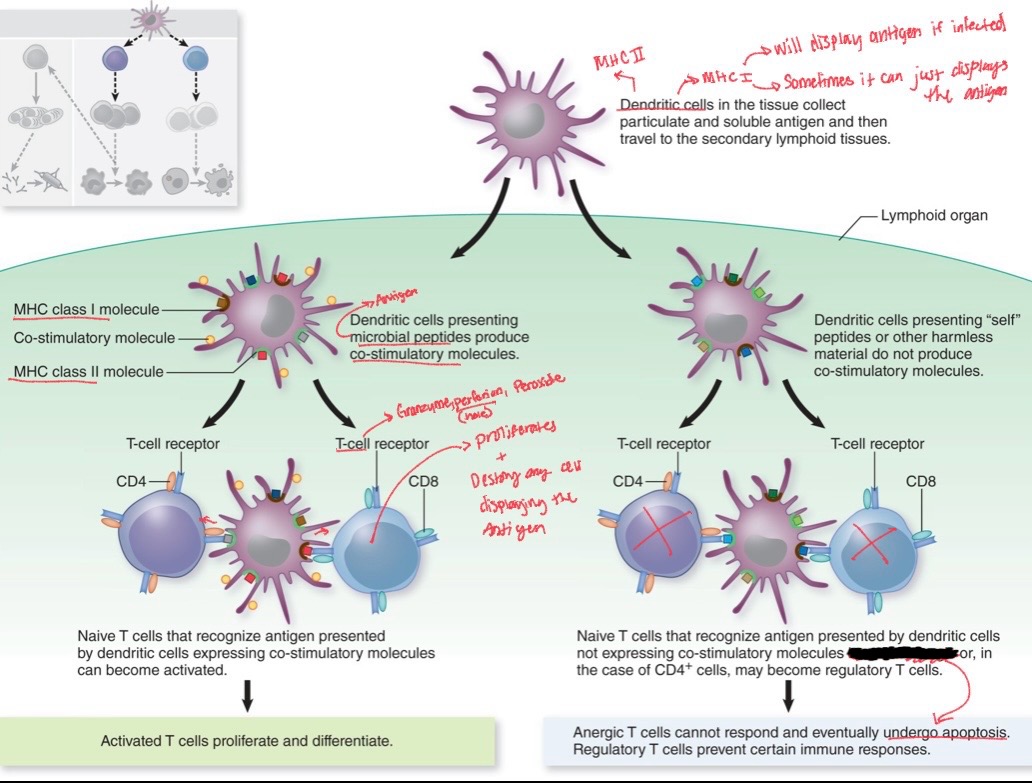
Found on APCs (Dendritic, macrophages, monocytes, b-cells)
Presents exogenous antigens
Understand the role of T-cells in both humoral and cell-mediated immunity
T-lymphocytes in humoral immunity (T-dependent immunity)
Antigen Recognition:
Naive B cells BCRs, will recognize a specific antigen pathogen. When the antigen binds to the BCR, it leads to the phagocytosis of the pathogen.
Antigen Processing and Presentation:
The B cell breaks it down into antigen fragments. These fragments are loaded onto (MHC) II.
T Cell Interaction & Co-Stimulation:
The B cell migrates to a lymph node, where it encounters Navie helper T cells. The Navie helper T cell recognizes the antigen via its Antigen binding clef and recognizes the MHC II via its CD4 receptor (TCR), thus becoming activated.
Cytokine Release & Clonal Expansion:
Effector helper T cells secrete cytokines to promote B cell proliferation and differentiation, this a population of B cells that can produce the specific antibody.
Class Switching:
Under the influence of cytokines (produced by effector helper T cells), B cells can undergo class switching to produce different types of antibodies (e.g., IgG, IgA, or IgE) instead of just IgM.
Differentiation:
B cells differentiate into plasma cells and memory B cells
T-lymphocytes in cell-mediated immunity
Antigen Presentation → An infected cell or an APC present an exogenous (viral antigen or non self-antigen) on an MHC I
Activation of T Cells and co-stimulation -> Proliferation
Naive Tc come into contact with APCs in the lymphatic tissues or at the site of infection. The CD8 receptors recognizes the MHC, and the antigen binds to the antigen binding clef.
It becomes an effector cytotoxic T cell; effector cytotoxic T is ready to find and kill infected cells displaying the same antigen.is
Function aka killing
Cytotoxic T cells travel to the site of infection and bind to infected cells displaying the exogenous antigen on their MHC I. The cytotoxic T cells release perforin (which creates pores in the infected cell’s membrane) and granzymes and peroxides. This process kills the infected cell, stopping the spread of the infection.
Formation of Memory T Cells
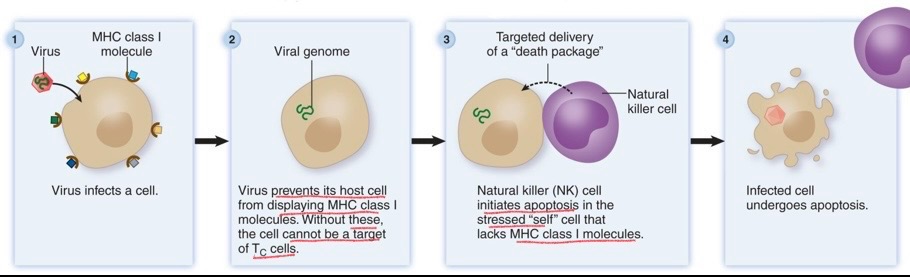
Know what a natural killer cell is and in general what it does
NK
In antibody-dependent cellular cytotoxicity (ADCC), antibodies (specifically IgG) attach to a virus-infected cell, marking it for destruction by natural killer (NK) cells.
Releases Perforins and granules
recognize cells lacking MHC I
Understand the difference between active and passive immunity, natural and artificial immunity, and how each might be acquired.
Passive (NO memory but protection)
Natural → Antibodies passing through breast milk (IgA) or placenta (IgG)
Artificial → donation of Antibodies & antivenoms
plasma infusion (BEER)
Antibodies infusion (VOKA)
Active (memory and protection)
Natural → You get sick and don’t die
Artificial → Vaccines
Understand how vaccines protect individuals and prevent the spreading infectious diseases through the population (herd immunity). Know the differences between and relative advantages and disadvantages of attenuated vs inactivated vaccines. Understand the basics of how the other vaccines we talked about in the video work
Vaccines
** Herd immunity: When most of a population is immune to a disease, preventing its spread due to a lack of susceptible hosts.
Attenuated: A weakened form of a pathogen that replicates in the body, usually causing no or mild disease.
Pros:
One dose typically provides long-lasting immunity since it multiplies in the body and may even spread immunity to others via virus particles.
Provides a stronger immune response and similar to active natural immunity
Cons:
May cause disease in people with weak immune systems
can sometimes mutate back to a harmful form
not ideal for pregnant women
needs refrigeration
Examples: Measles, mumps, rubella, chickenpox, yellow fever, and rotavirus vaccines.
Inactivated: pathogens that cannot replicate + an adjuvant
Pros:
Cannot cause infection or change back to a harmful form.
Cons:
Since they don’t replicate, they produce a weaker immune response, so boosters are often needed.
Need an adjuvant (a chemical needed to make the immune system response batter to the Inactivated vaccine)
Types:
Inactivated whole-agent vaccines: Made from killed microbes or viruses treated with chemicals to keep surface markers intact.
Examples: Influenza (flu shot), rabies, and hepatitis A vaccines.
Subunit: injects viral surface proteins or other specific parts of the pathogen as the vaccine
Ex. Hepatitis B
Know the different classes of hypersensitivities and the differences between them. Focus on Type I and Type II, know the general outline of type III and IV. Know what antibodies and cells are associated with each of the classes. Be able to distinguish between systemic and local hypersensitivities. Know the common treatments/preventative measures for each of the hypersensitivities and how they work. For Type I hypersensitivities know the entire molecular mechanism of both first exposure (sensitization) and secondary exposures
Immune system disorders:
Hypersensitivities:
Allergies, transfusion, and blood type reactions,
transplant rejection, over-reaction to infection (toxic
shock), etc. → pos. feedback loop*
Autoimmune diseases:
Type 1 diabetes, lupus, graves’ disease, myasthenia
gravis, MS, and others → attacks self*
Immune deficiency:
Can result from genetic defect, infection, environmental
factors, or treatment → bubble boy*
Hypersensitivities
Type I: Immediate IgE-Mediated
Process
Initial Exposure to Allergen
A person first encounters an allergen (e.g., pollen, pet dander, or food). Plasma cells near mucous membranes recognize the allergen and start producing IgE.
IgE Production → Sensitization
In allergic individuals, IgE is produced in response to the allergen. IgE Fc region binds mast cells or basophils.
After the first exposure, the person becomes sensitized to the allergen. IgE antibodies remain attached to mast cells and basophils, priming the immune system for future encounters.
Subsequent Exposure to Allergen
During a second exposure to the same allergen, the allergen binds to the IgE on the surface of mast cells and basophils.
Degranulation
The binding of the allergen triggers the release of histamine from mast cells and basophils.
Symptoms of Allergic Reaction
Result from the release of mast cells, which are local since there located in the tissues
Hay fever (sneezing, runny nose, itchy eyes) → mucus production
Hives (wheal and flare)
Asthma (bronchoconstriction)
Result from the release of basophils, which are systemic since there located in the blood stream
Anaphylaxis (swelling and ↓BP)
Treatment of symptoms & prevention
Hive & Hay fever → antihistamines
Asthma → antihistamines are ineffective but steroids work
Anaphylaxis → Epi-pen & hospital intervention
Desensitization basically exposure therapy
Causes immune system to produce IgG instead of IgE. The IgG neutralize the allergen
Omalizumab or rhuMab (Recombinant humanized Monoclonal antibody)
synthetically produce IgG
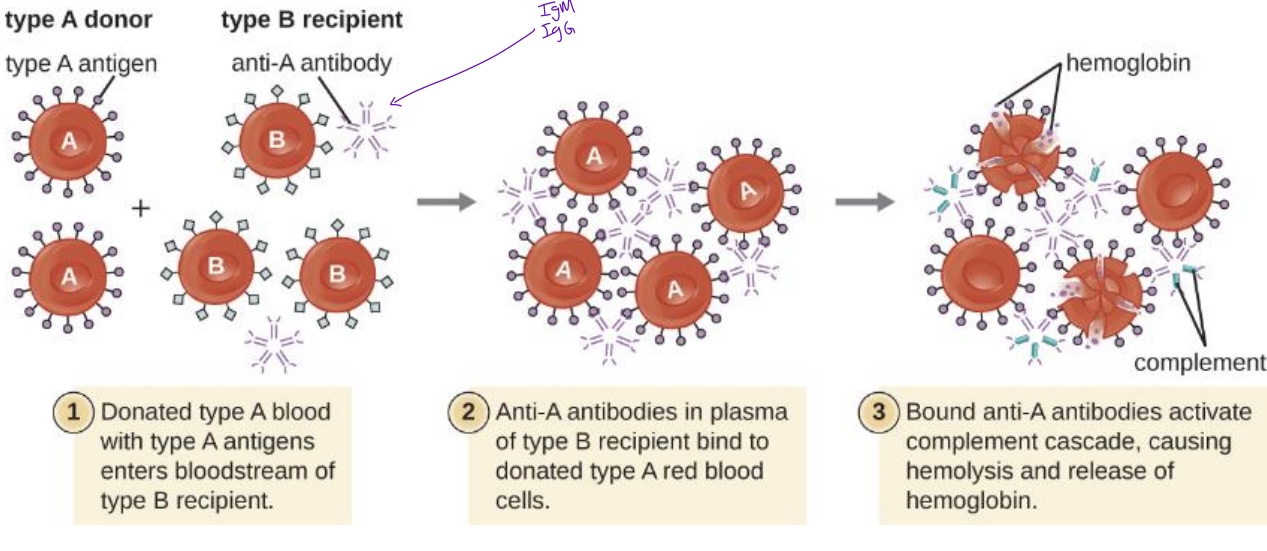
Type II: Cytotoxic/antibodies reactions
Sub-types
Incompatible Blood Transfusion → IgG or IgM
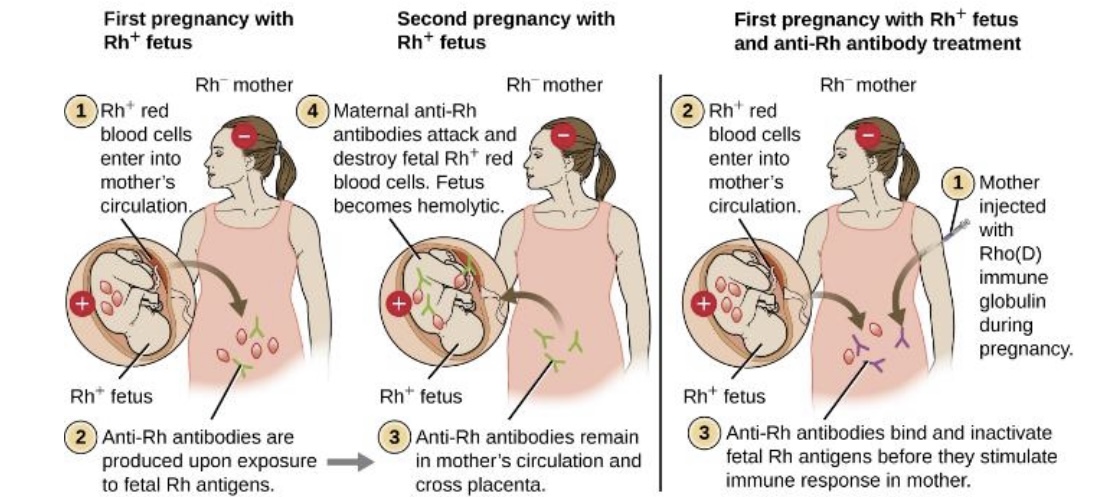
hemolytic disease of the newborn → mother antibodies attack the second Rh+ fetus
Type III: Immune Complex-Mediated
When ↓IgG or IgM antibodies bind to ↑soluble antigens, smaller complexes can form and remain in the blood or tissues.
These complexes can trigger blood clotting and activate the complement system, which recruits more phagocytes.
Caused by penicillin allergies
Immune complexes are linked to conditions such as…
joint pain → arthritis
such as farmer’s lung
systemic lupus erythematosus
bacterial endocarditis
early rubella infection
malaria
glomerulonephritis
Type III: Delayed-Type Cell-Mediated
Peaks 2-3 days after exposure.
Cytotoxic T cells destroy infected cells. While this helps control infection, it can also damage tissue, leading to chronic damage.
Caused by…
Cheap metal (nickel) jewelry
cosmetics
latex
poison ivy and oak
pos. tuberculin skin test
Ex.
Contact dermatitis
leprosy