Blood Vessels
Blood Vessel Structure
Blood Vessels - made of fibrous tissue, elastic tissue, and smooth muscle
fibrous for structural support and stiffens
elastic lets vessels expand and hold more blood as well as recoil and exert pressure on blood to push it forward
smooth muscle arranged in circular or spiral layers to contract (vasoconstrict) narrowing the vessel and decreasing blood flow or to relax (vasodilate) widening the vessel and increasing blood flow
Tunica layers - often in medium to large blood vessels as 3 layers
interna - made of endothelium lining the lumen, acellular basement membrane supporter, and internal elastic lamina to let blood vessel expand and recoil
media - made of smooth muscle cells that express contractile proteins needed for vasoconstriction (narrowing) and vasodilation (widening)
adventitia - outermost layer of a blood vessel wall made of loose collagen fibers that protect and anchor vessel to surrounding tissues
Capillaries only have a intimal layer of endothelial cells resting on basal lamia for easy diffusion of materials in and out
Microcirculation - made of arterioles and venules that have smooth muscle to support vasoconstriction and vasodilation, and capillaries that have pericytes that regulate blood flow
Continuous Capillaries - most common type with inter-endothelial junctions 10-15 nm wide that have a interrupted lining and only allow very small molecules like water or ions to pass through. can be absent in some vascular beds like BBB
Fenestrated Capillaries - endothelial cells are thin and perforated with pores about 60 - 88 nm wide to allow small molecules and limited protein amounts through into exocrine glands and small intestine (epithelia)
Sinusoidal or Discontinuous Capillaries - large gaps of about 30 - 40 um wide in addition to fenestrate to allow blood cells and various serum proteins through to liver and spleen
Hydrostatic and Oncotic Pressures
Body fluid divided into intracellular and extracellular fluid compartments with extracellular subdivided into intravascular fluid (plasma or blood) and interstitial fluid
Diffusion, transcytosis, and bulk flow enable continuous exchange of water and solutes among body fluid compartments in capillaries to maintain balance
diffusion - small uncharged and lipid soluble substances (O2 and CO2) freely diffuse through the endothelial cells anytime along capillary
transcytosis - transport of large non-lipid solute molecule (hormones and proteins) across the capillary wall to target tissues
bulk flow - movement of water and dissolved solutes (glucose, AA, ions,electrolytes) across capillary wall through water-filled pores in endothelial cells regulated by hydrostatic and osmotic pressure
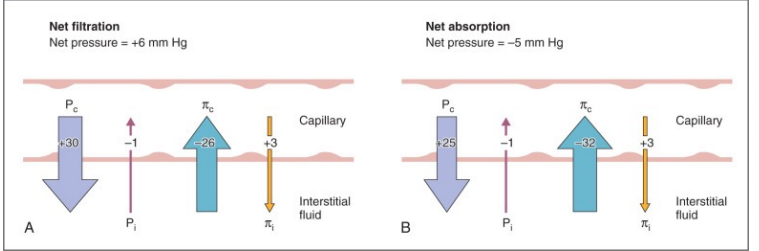
Forces determining the movement of fluid in or out of capillaries
blood capillary hydrostatic (BHP/PC) - push fluid into interstitial
interstitial fluid hydrostatic (IFHP/Pi) - push fluid into capillaries
plasma colloid osmotic (BCOP/πc) - pull fluid into capillaries
interstitial fluid oncotic (IFOP/πi) - pull fluid into interstitial
Filtration - pressure driven movement of fluids and solutes from capillaries into interstitial fluid supported by BHP and IFOP
Reabsorption - pressure driven movement of fluid into blood capillaries from interstitial fluid supported by BCOP and IFHP
Starlings Equation of Net filtration Pressure (BHP + IFOP) - (BCOP +IFHP)
Varicose Veins - enlarged bulging superficial veins felt beneath the skin
starts with valvular dysfunction that lets backflow resulting in blood pooling and raising BP. High BP gets transmitted to capillaries that suffer damage and get more permeable. increasing BHP to push fluid out into interstitial space of surrounding tissues
Edema in CKD - decline in kidney function results in increased total blood volume (hypervolemia) that raises BHP forcing fluids into interstitial space.
also causes proteinuria resulting in a reduced BCOP lessening the force that normally pulls fluid back into capillaries
Lipoprotein Classification to explain Dyslipidemia
Lipoproteins - chylomicrons 2%, VLDL 5-10% ,IDL,LDL 25%,HDL 50% (protein %)
based on the densities from low to high
more protein content the higher the density and more heavy
Lipoproteins - combination of cholesterol and triglyceride and water soluble proteins (apoproteins) making a transport molecule
Apolipoprotein B - primary water-soluble protein associated with VLDL and LDL and contributes to plaque formation and atherosclerosis
Dyslipidemia - imbalance of lipid components in blood in which TC,LDL,TG are all high while HDL is low meaning more lipids in storage sites than liver
non-HDL = TC - HDL includes increased risk of fat in arteries and is a strong predictor of ASCVD
apolipoprotein B - high risk marker and indicator of the progression of atherosclerosis which starts when it gets trapped in vascular wall
primary dyslipidemia - develops independently of other health problems of behaviors, but may have a genetic basis
secondary dyslipidemia - associated with other health problems and behaviors like diet, obesity, and TZD
Lipid Metabolism
Chylomicrons transport dietary TG to peripheral tissues and liver after lipoproteins are synthesized in the small intestine and liver
VLDL transports endogenous TG and cholesterol to peripheral tissues and make IDL after VLDL releases TG and returns to liver
Three pathways
LDL receptor - mediated transports cholesterol from liver to cells throughout the body
HDL mediated (good) - reverse transport of cholesterol by transporting excess from periphery to liver
Scavenger Pathway - phagocytic monocytes and macrophages ingestion oxidized or chemically-modified LDL by immune cells
removing apoproteins and triglycerides, VLDLs are transformed into IDL and LDLs
LDLs deliver cholesterol to various body sites like peripheral tissues and liver and are also part of artherocloerotic plaques.
Pathophysiologic Basis of Arteriosclerosis
Arteriosclerosis - abnormal hardening or excessive resistance in arteries
medial calcific Sclerosis - calcium deposits in medial layer of an artery, but usually benign
arteriosclerosis - hardening of arterioles by pink hyaline material causing leakage of proteins into the vessel wall across damaged endothelium or basement membrane. as seen in hypertensive and diabetics
Atherosclerosis - artery wall thickens from accumulation of white blood cells (foam cells or fatty streaks) and proliferation of intimal-smooth-muscle-cell creating atheromatous (fibrofatty).
Accumulation contains living/active WBC and remnants of dead cells like cholesterol and triglycerides, Ca, and other crystalized materials, reducing the elasticity of artery walls but not blood flow
Pathophysiology
chronic inflammatory process in response to injury of vascular endothelium by glycoxidation products, shear stress, excess free fatty acids, bacterial products, neurohormonal abnormalities
Damaged endothelium becomes prothrombotic, reduced release nitric oxide and impaired vasodilatory capacity, release of chemoattractants for inflammatory cells and platelets
regulation of blood cholesterol levels and management of other risk factors can restore endothelial function, nitric oxide release, and vasodilatory response
Mechanism of Action of Classes of antilipidemic drugs
Normal Lipid Panel
Good | Risk | |
TC | < 200 | > 240 |
LDL | < 100 | > 160 |
HDL | > 60 | < 40 |
TG | < 150 | > 200 |
LDL = TC - HDL - (TG/5) if TG > 400 mg/dL
Risk Category | Therapeutic Lifestyle changes to LDLC |
High risk CHD or CHD equivalents 10 year risk > 20% | > 100 mg/dL |
Moderate High risk: 2 risk factors 10 year risk 10-20% | > 130 mg/dL consider drug therapy to lower |
Moderate Risk: 2 risk factors 10 year risk < 10 % | > 130 mg/dL |
Low risk: 0-1 risk factor | > 160 mg/dL |
Statins MOA - inhibit HMG-CoA reductase stopping the rate limiting step in cholesterol biosynthesis
deceased cellular cholesterol concentrations
increase downstream expression of LDL receptor promoting the uptake of LDL leaving LDL in plasma
Simvastatin (Zocor), Atorvastatin (lipitor), Pravastatin (Pravachol)
Sequestrants MOA - inhibit the reabsorption of bile acids from the gut to force hepatocytes to upregulate LDL receptor expression and increase clearance of LDL-cholesterol from the periphery to make bile acids
interfere with the absorption of fat-soluble vitamins and thiazide diuretics
cholestyramine (questran,prevalite), colesevelam (welchol), colestipol (colestid)
Cholesterol absorption inhibitors MOA - inhibit the absorption of cholesterol and plant sterols from duodenum by blocking NPC1L1 transport protein in the brush border of GI
does not affect the absorption of fat-soluble vitamins, triglycerides or bile acids
Ezetimibe (zetia)
Fibrates MOA - complex agonist at the peroxisome-activated receptor-a (PPARa) nuclear receptors to increase hepatic synthesis of apoA1 and apo2 for more HDL and decrease apoC3.
increases FA oxidation with a downstream decreased TG synthesis
Gemfibrozil (Lopid), fenofibrate (antara,fenoglide), bezafibrate (bezalip)
PCKS-9 inhibitors MOA - inhibits the binding of PCSK to the LDL receptors on hepatocyte surfaces increasing the number of them to clear LDL
Alirocumab (praluent) and Inclisiran (Leqvio)
Bempedoic Acid MOA - prodrug activated in the liver that inhibits acetyl-COA carboxylase to reduce subsequent production of cholesterol.
Nexletol (single tablet) and Nexlizet (bempedoic acid+ezetimibe)
Antisense oligonucleotides ASO MOA - inhibits the synthesis of apolipoprotein B by binding to cognate mRNA resulting in a substrate that degrades mRNA
reduces production of apoB and apoB-containing lipoproteins
Mipomersen and Volanesorsen
Microsomal Triglyceride Transport Protein MTP MOA - inhibits the activity of MTP reducing the production of apoB-containing lipoproteins by stopping the transfer of cholesteryl esters and triglycerides to apoB to make VLDL and chylomicrons
Lomitapide (Juxtapid)