AKI
recognize if AKI based change in SCr or UoP
nephrotoxic
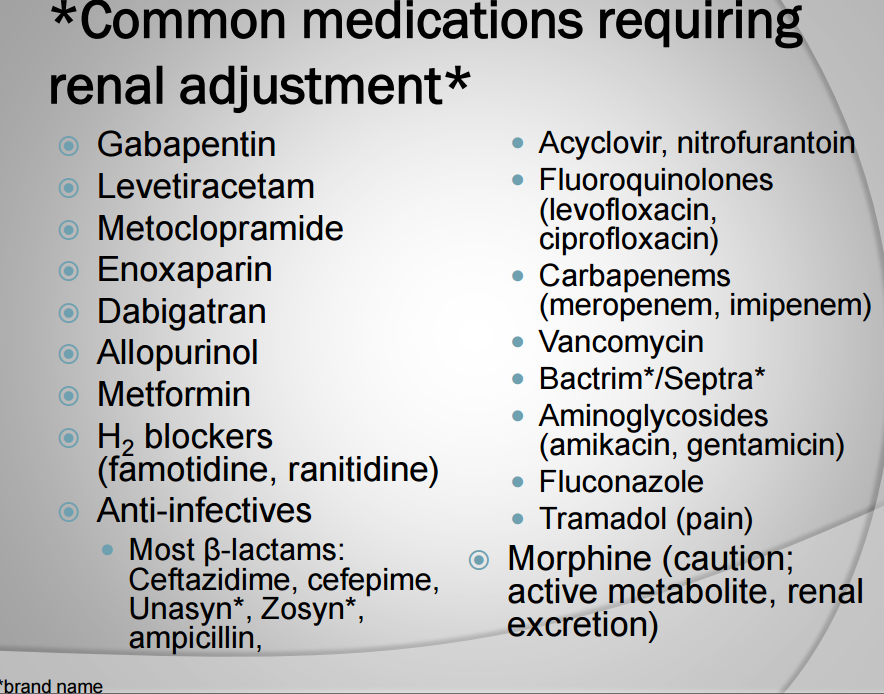
renally adjust
Detection Of AKI only one meet
increase in SCr by at least 0.3 within 48 hours
Increase in Scr 1.5x from baseline within 7 days
Decrease in Urine Output (UoP) to < 0.5 mL/kg/hr for at least 6 hours
normal 2L/day and typically changes faster than SCr, thus better to use for dose adjustment.
Nonoliguria - UoP > 500 mL/day → intrinsic failure or incomplete block
Oliguria - UoP 50-500 mL/day → prerenal
Anuria - UoP < 50 mL/day → complete block or catastrophy
Clinical Presentation of AKI
rapid decrease in GFR and increase in SCr and BUN
dehydration and hypotension and edema/sudden weight gain
severe abdominal/flank pain from infection, nephrolithiasis, glomerular or interstitial nephritis
bladder distension from obstruction
cola-colored urine sign of blood and acute glomerulonephritis
Assessment based on trends -
PMH of CKD, DM, HTN since high risk medications needed over long-term usually hold then give back
Onset of acute AKI, Acute or Chronic CKD
eGFR Cockcroft-Gault often overestimates in worse and underestimates in resolving due to lagging behind 1-2 days
Urinary analysis to determine type of AKI and infection
CBC to see infection
Electrolytes too see if any are toxic or near those levels
BUN:SCr increased to 20:1 sign or prerenal AKI
Fractional excretion of sodium (FENa) assess tubular integrity
low value means pre-renal AKI <1 % and renal > 2%
other conditions associated CHF, cirrhosis, nephrosis, contrast-induced nephropathy, rhabdomyolysis
Imaging of abdominal, CT, ultrasound, biopsy can reveal shrunken kidneys and obstructions when source unclear after labs
Types Of AKI
normal afferent arteriole dilates (widens) or efferent arteriole constricts (narrows) along with RAAS system to compensate for mild-moderate decreases or increases to renal perfusion
Pre-Renal - decreased blood flow to kidney caused by
less intravascular or circulating volume blood
less perfusion due to medications or renal artery stenosis
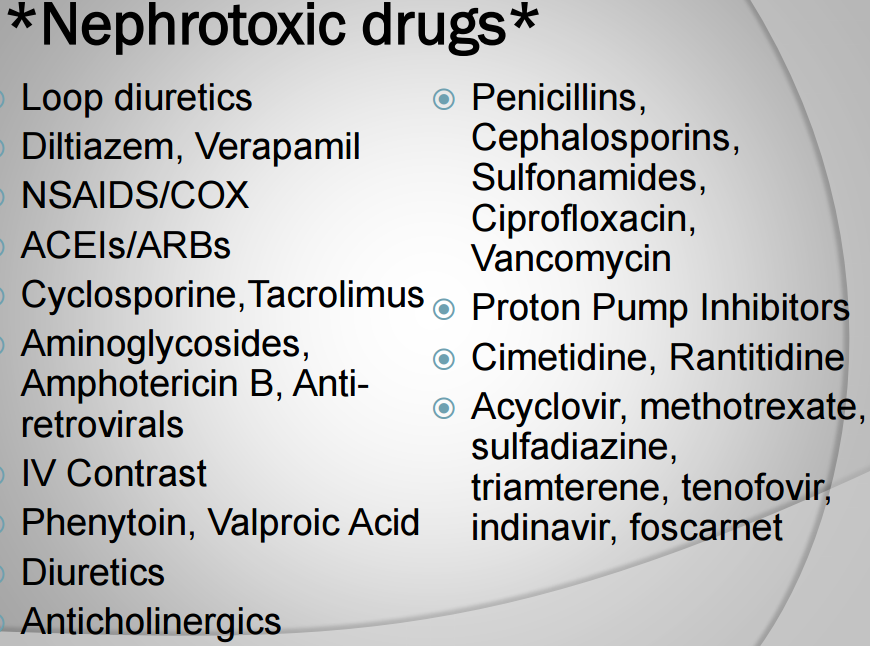
loop diuretics, NSAIDs/COX2, ACEi/ARBs, cyclosporine or tacrolimus
Intrinsic - injury to kidney anatomy of renal tubules, glomerulus, vascular structures, interstitium
tubular - from prerenal damage like prolonged HTN or nephrotoxic causing acute tubular necrosis (ATN)
Interstitial - inflammatory infiltrates and edema in interstitium from nephrotoxic medications and takes weeks to months to heal after stopping medication
Vasculatures - occlusion of renal vessels from HTN or thrombus
Glomerular - nephrotic syndrome and glomerulopathies
Post-renal - caused by obstruction from constriction or crystallization
common in BPH, nephrolithiasis, malignancy from medications like acyclovir, methotrexate, sulfadiazine, triamterene, tenofovir, indinavir, foscarnet, anticholinergics
Contrast Induced nephropathy CIN - visualize atomic structures in CT and angiography, but directly toxic and can lead to ATN
often nonoliguric and typically returns within 14 days to serious AKI
preventable by anticipation and measures
alternate CT with and without contrast in small volumes
avoid nephrotoxic agents and n-acetylcysteine
hydrate before and after administration to dilute contrast
LR/NS as 1 -1.5 mL/kg/hr started 3-12 hours before procedure then 6-24 hrs afterwards
Drug induced - increased SCr and BUN while decreasing GFR
shown by timing of drug or dose adjustment and recovery upon stopping
diuretics causing too much volume depletion lessening perfusion and being nephrotoxic
tacrolimus elevates levels to increase SCR causing renal dysfunction
Nephrotoxic Drugs
usually keep the life saving ones like antibiotics, antivirals, immunosuppressants
General Management
prevention by avoid nephrotoxic agents in high risk, monitor patient closely, renally adjust doses and short duration
treat underlying problem and d/c offending agents
hydration and dialysis
Supportive Care Treatment
Generally treat identifiable causes which can reverse pre-renal/post-renal AKI and prevent further damage
mange fluids, electrolytes, d/c offending agents, treat non-renal complications while recovering
hyperkalemia (Na 135-145 mEq/L),
hyperphosphatemia (Phos 2.5-5 mg/dL),
hypermagnesemia (Mg 1.5-2.0 mEq/L),
acid-base abnormalities
hydrate PO or NS/LR given as 250 mL- 1L boluses then re-evaluate
if overloaded or pulmonary edema use furosemide or (torsemide, bumetanide, ethacrynic acid), but monitor electrolytes again and renal dysfunction caution
blood products if low Hgb, Hct, anemic, active bleeding
Monitor SCr, BUN, fluid input and output, electrolytes, vitals, weight, medications
Correct: electrolytes, acid-base disorders, fluid status, etc
Even if dopamine increases kidney perfusion not for AKI
Dose Adjustment
Contrast Induced Nephropathy
IV contrast used to improve visualization of atomic structures within the body during coronary angiography and CT
Leading cause of AKI, but often nonoliguria and typically returns within 14 days and can progress to serious AKI needing dialysis
Risk factors with conditions that decrease renal perfusion (DM, CKD, sepsis, hypotension, dehydration, frequent administration, concurrent nephrotoxic agents)
Prevent by
alternate CT with and without contrast in small volumes,
hydration 1-1.5 mL/kg/hr before and after administration to dilute
avoid nephrotoxic agents in sepsis, ESLD, HIV, CHF, Transplant
use lower doses and renally adjust
monitor patient closely and treat underlying problems
dialysis
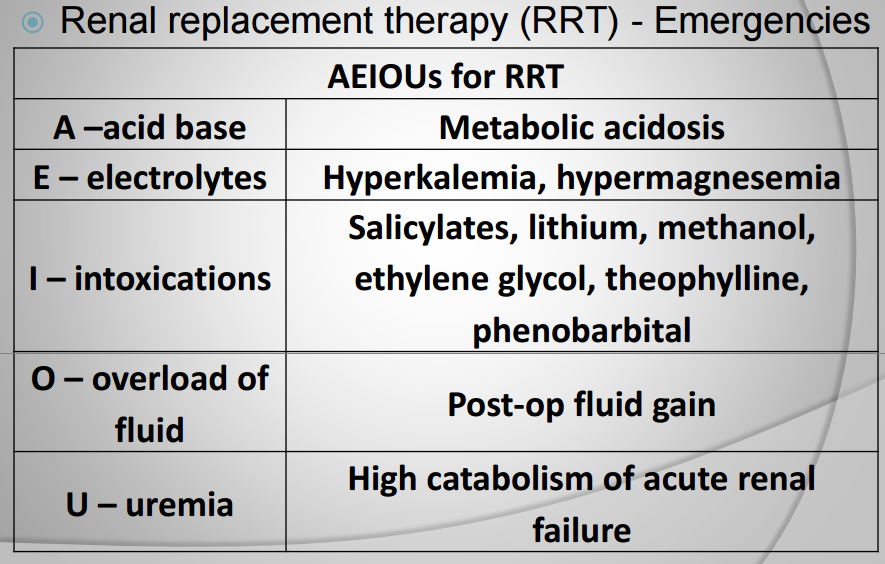
Renal Replacement Therapy (RRT)
short (AKI or AEIOus) or long term (CKD) replacement of patients own kidneys due to bad kidney function for inpatient, outpatient, clinics, and at home
Once started survival rate goes down due to CV related or infection IV dialysis
Initiate and plan for stage 4 CKD based on patient and nephrologist input
Dialysis
determines rate and efficacy of removal by modifying rate, speed, target
can go between large and small pores to change flux and filter molecules
dialysate creates osmotic gradients to clean the blood by changing concentration i.e hyperkalemic dialysate low [K] to diffuse out patient
HD | CRRT | Hybrid | |
drug dosing | less | more | both |
location | clinic | home | both |
duration | 4 hours | 10 hours | 24 hours |
frequency | 1 time | 3 days/week | daily |
Hemodialysis
commonly done 3 days/week for 3-4 hours with heparin in circuit to anticoagulate blood
Needs vascular access so arteriovenous (AV) fistula (abnormal connection) connects artery and vein to increase blood flow for a dialysis machine
lasts longer, less infection and thrombosis risk preferred for Long term
takes 3 - 4 months to mature before use
AV graft and CVC in emergency (tunneled or not tunneled) have higher risks
Peritoneal Dialysis
Blood is filtered out by the peritoneal cavity by a indwelling catheter across a semipermeable membrane lining abdominal wall and covering organs
dwelling - hookup, infusion, and fresh diffusion of dextrose
exchanging - waste diffusion is drained
same result as hemodialysis
less efficient and safe due to constant therapy
more stable due to slower filtration rate
Continuous Renal Replacement therapy (CRRT)
reserved for critically ill hemodynamically unstable patients who cannot tolerate HD, but has same mechanism as HD over 24 hours