S1W7 ACP Right Heart Cath AM
Right Heart Catheterization Overview:
Purpose: Right heart catheterization (RHC) provides essential hemodynamic data for diagnosing cardiovascular conditions.
Key Tools: Involves cardiac catheterization and angiography.
Educational Objectives :
Understand the history and development of RHC.
Learn to perform and interpret right heart studies.
Identify the indications for using RHC as a diagnostic tool.
History of RHC :
First performed on a horse by Claude Bernard (1844).
First human RHC by Werner Forssmann (1929).
Technique involved self-catheterization via left antecubital vein.
Indications for RHC :
Measurement of cardiac output.
Assessment of intracardiac pressures and shunts.
Evaluation of pulmonary hypertension (PH).
Diagnosis of valvular disease.
Historical role in cardiogenic shock evaluation.
Contraindications for RHC :
Absolute Contraindications:
Mechanical tricuspid/pulmonic valve
Right heart masses (thrombus/tumor)
Right-sided endocarditis
Relative Contraindications:
Coagulopathy - blood clotting disorder
Pacemaker presence
Skin site infections
Bioprosthetic tricuspid or pulmonic valve
LBBB
Arrhythmias
Procedure of RHC :
Preparation:
Calibrate oximeter
check hemoglobin (Hb)
setup ECG and saturation probe.
set up saline / pressure bag
Align transducer with reference point for pt - mid chest inline with approx RA
Open transducer to air and zero - close transducer once zeroed
WHO checklist
Provide operator with correct equipment : sheath, guidewire, cath
Access: Predominantly via femoral vein; alternative access through brachial, internal jugular, or subclavian veins.
Key Measurements :
Hemodynamic :
Record phasic and mean pressures.
Advanced catheter placement into right atrium (RA), right ventricle (RV), pulmonary artery (PA), and pulmonary capillary wedge pressure (PCWP).
Adjust scale as you go , nice trace settle , measure end of expiration
Wedge pressure O2 sats >95%, PCWP clear V waveform
Pullback from PCWP through to RA - record each pressure wave form change
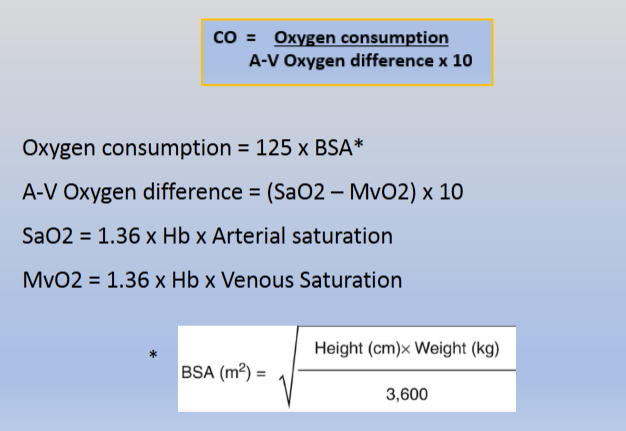
Calculation Methods:
Cardiac Output :
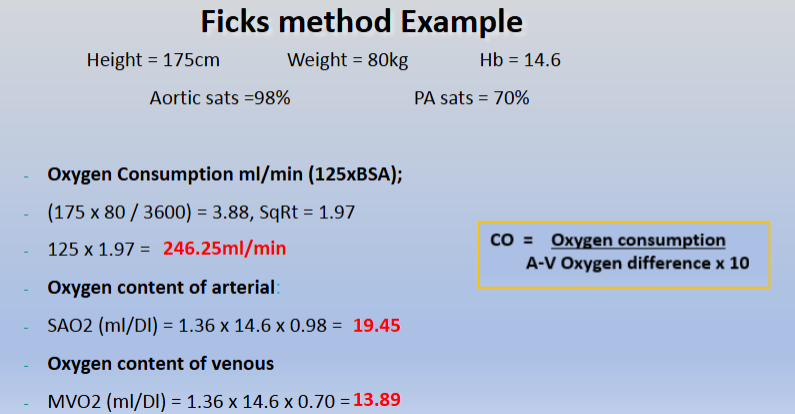
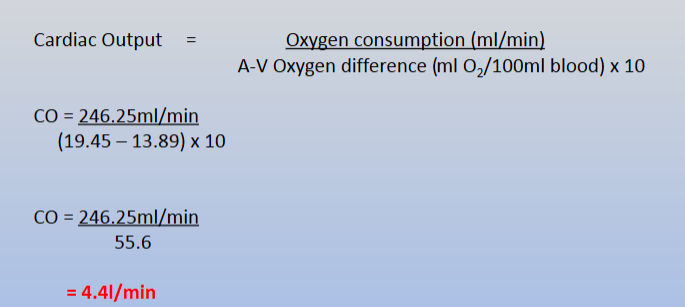
Fick’s Method: Measures oxygen consumption and differences in oxygen content.
Normal CO: 4.0-6.0 L/min.
1. Oxygen Consumption
2. Oxygen content of arterial blood
3. Oxygen content of mixed venous blood

EXAMPLE:
Direct versus Indirect Fick’s method:
The direct Fick method is preferred, but requires direct measurement of O2 uptake, a technique that is not widely available.
The indirect Fick method, which uses estimated values of O2 uptake, is acceptable but lacks reliability
Thermodilution Method: Involves change in temperature measurement post-fluid bolus injection.
Uses Swans Ganz catheter
Preferred method for calculating CO
In patients with intracardiac shunts, thermodilution may be inaccurate because of early recirculation of the injectate.
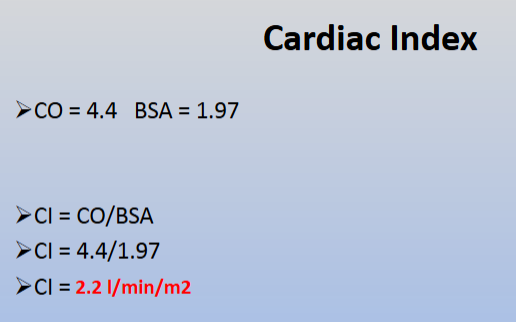
Cardiac Index: CI) adjusts output to patients BSA :
Normal CI: 2.4-4.0 L/min/m2
A cardiac index below 2.0 L/min/m2 might indicate cardiogenic shock in an acute setting
Analysing Pulmonary Vascular Resistance (PVR) :
The resistance against blood flow from the pulmonary artery to the left atrium
PVR Formula: Used for diagnosing pulmonary arterial hypertension (PAH).
Normal value: 0.25–1.6 WU. Values >3 WU indicate PAH.
A PVR >3 WU is required for the diagnosis of Pulmonary arterial hypertension
Is highly sensitive to changes in both flow and filling pressure, and may not reflect changes in the pulmonary circulation at rest

EXAMPLE:
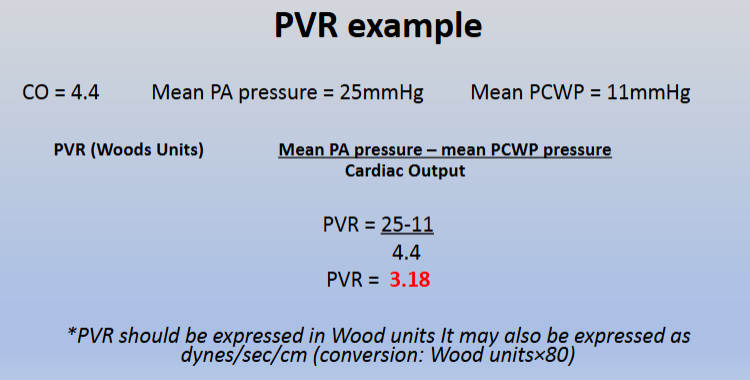
Breakdown:
Calculating shunts:
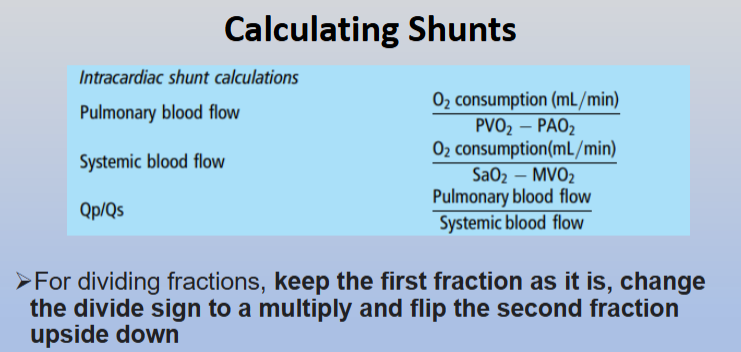
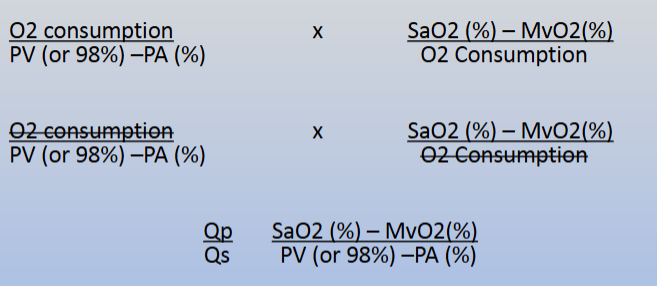
Shunt formula:
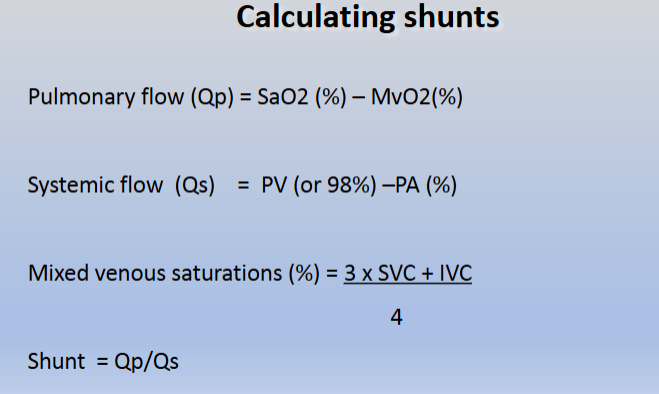
Qp:Qs 1 = normal
Qp:Qs >1-1.5 = mild
Qp:Qs >1.5-2 = moderate
Qp:Qs >2 = severe
Usually shunt is L>R due to pressures
Can be R>L which would give a value of <1
Common Complications of RHC:
Potential Risks:
Ventricular arrhythmias
Advanced AV block
Right ventricular perforation
Pulmonary rupture or infarction
Pneumothorax
References
European Society of Cardiology guidelines and related literature on pulmonary hypertension and RHC practices.