thoracic wall & lungs
overview of thorax
musculoskeletal wall of the thorax is flexible & consists of vertebrae, ribs, & the sternum. It offers protection to organs.
The thorax contains the lungs & the heart.
The diaphragm & thoracic wall work to move air into & out of the lungs during breathing.
The mediastinum (middle) contains the heart & provides a conduit for structures passing into & out of the thorax
overview of thorax
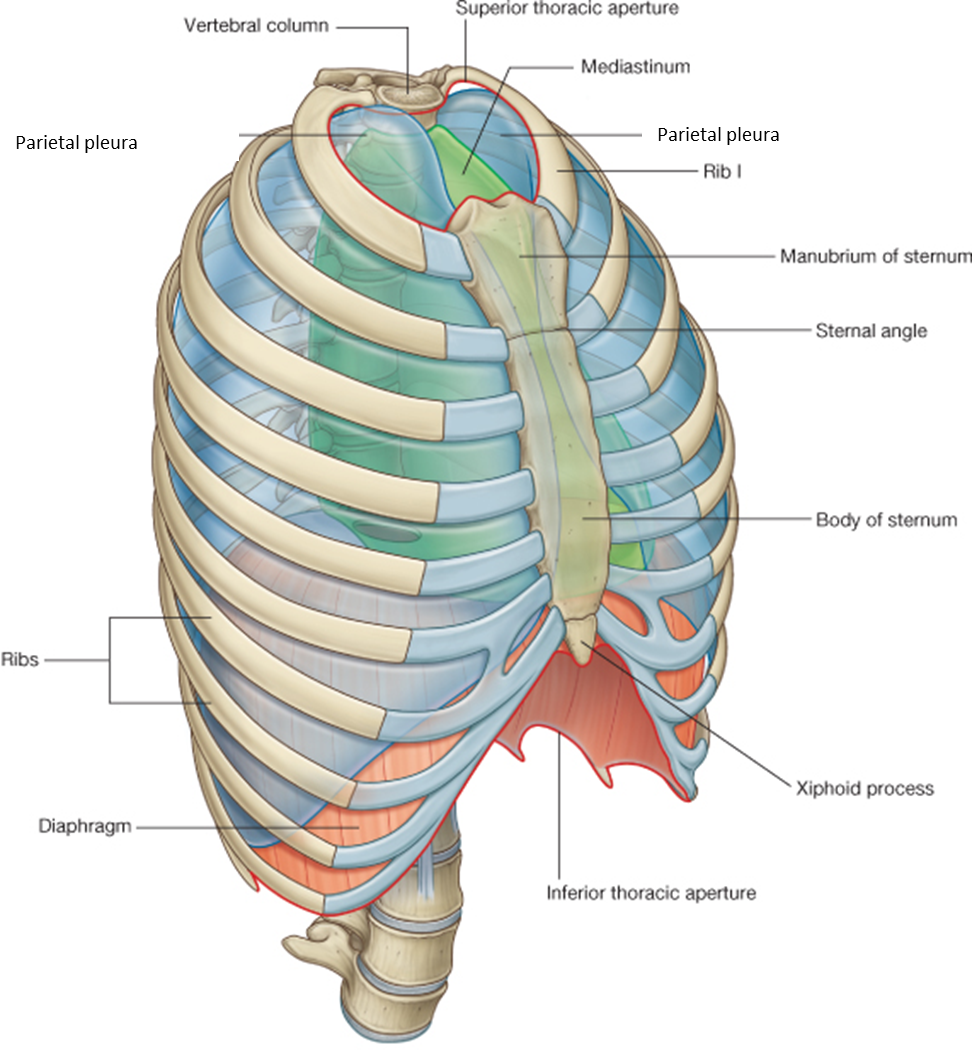
Divided into three compartments: left & right pulmonary cavity, and the mediastinum.
There is a superior & inferior aperture, aperature means opening.
thorax (chest cavity) has two openings:
Superior Thoracic Aperture (Thoracic Inlet)
the upper opening of the thorax, allowing structures to pass btwn the neck & chest.
always open
It is bordered by:
First thoracic vertebra (T1) (posteriorly)
First pair of ribs & costal cartilages (laterally)
Manubrium of the sternum (anteriorly)
Important structures passing through include the trachea, esophagus, major blood vessels (like the subclavian arteries & veins), & nerves (like the vagus & phrenic nerves) thorax
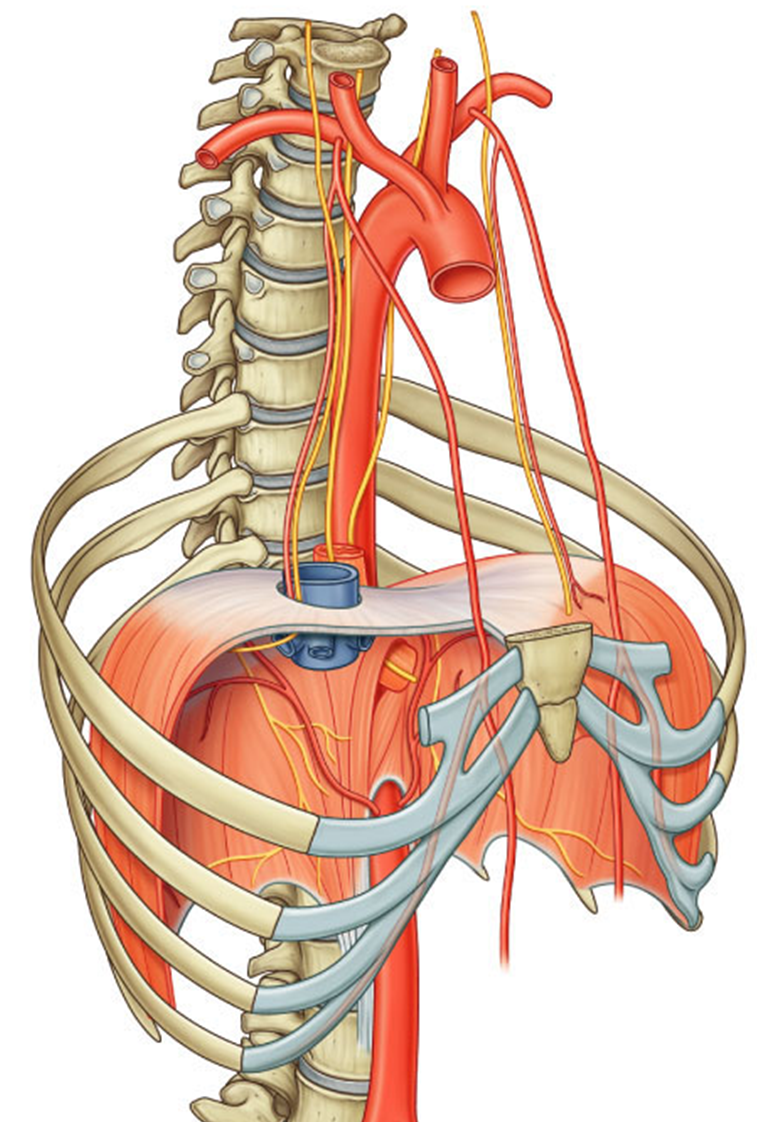
Inferior Thoracic Aperture (Thoracic Outlet) – This is the lower opening of the thorax, which is larger & closed off by the diaphragm, separating the thoracic cavity from the abdominal cavity. It is bordered by:
12th thoracic vertebra (T12) (posteriorly)
11th & 12th ribs (posterolaterally)
Costal margin (cartilages of ribs 7-10) (anterolaterally)
Xiphisternal joint (anteriorly)
Structures passing through the diaphragm include the aorta, esophagus, & inferior vena cava.
Though "aperture" means "opening," the superior aperture remains open, while the inferior aperture is largely closed off by the diaphragm except for small passageways for structures to pass through.
The diaphragm encloses the thoracic cavity inferiorly.
The superior aperture is open to permit passage of structures to the neck.
parietal pleura expands above first rib into neck
thoracic wall
mediastinum
tracheobronchial tree
lungs
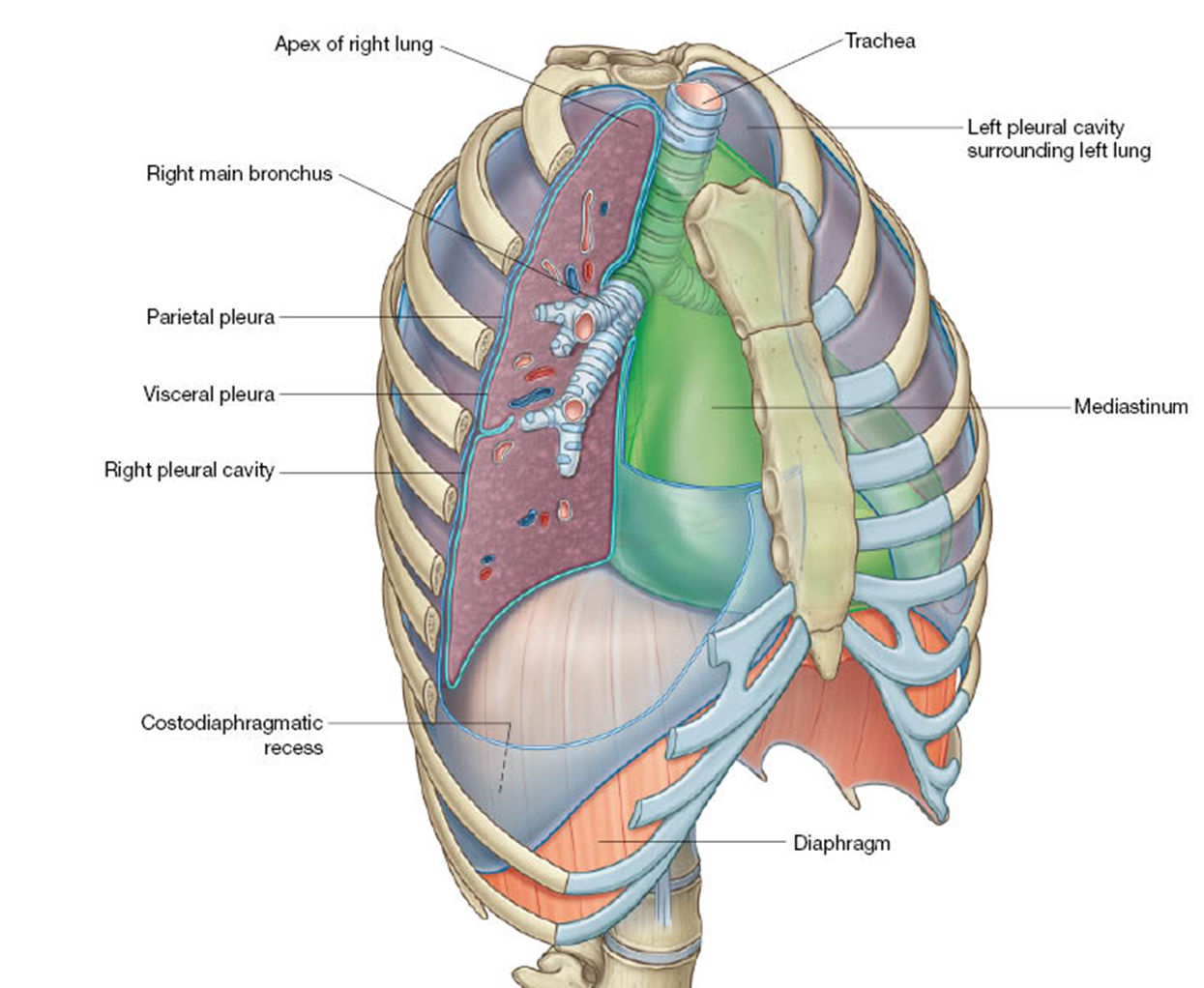
parietal & visceral pleura what is the difference?
pleural cavity (potential space)
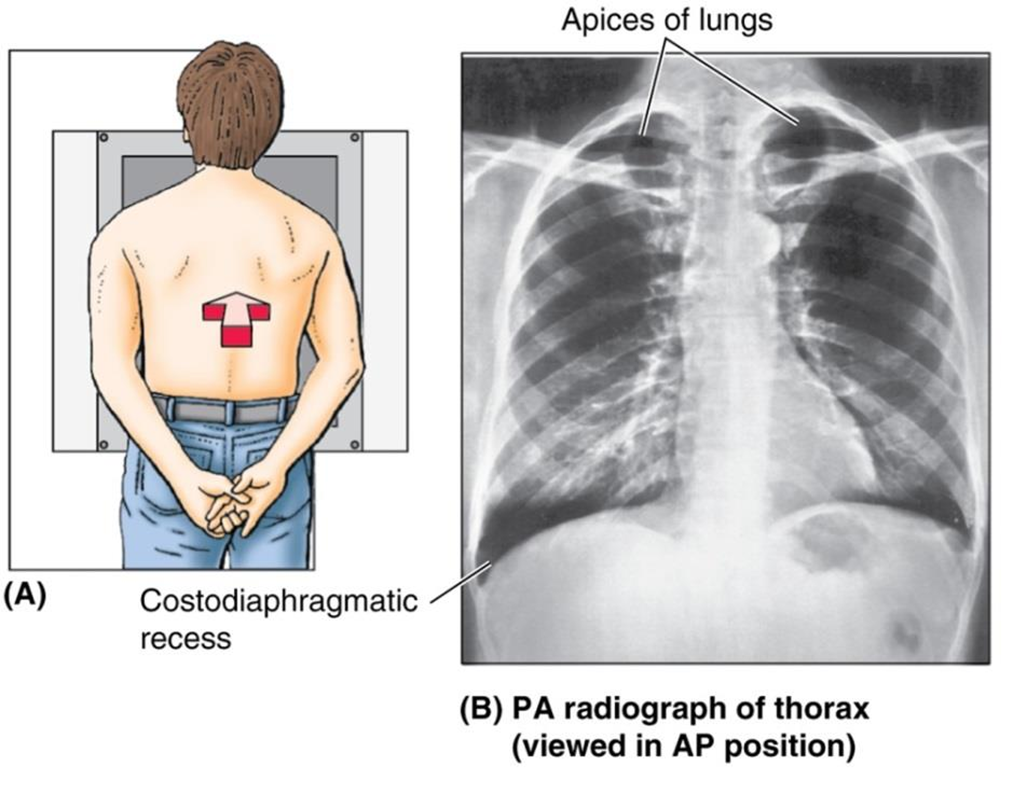
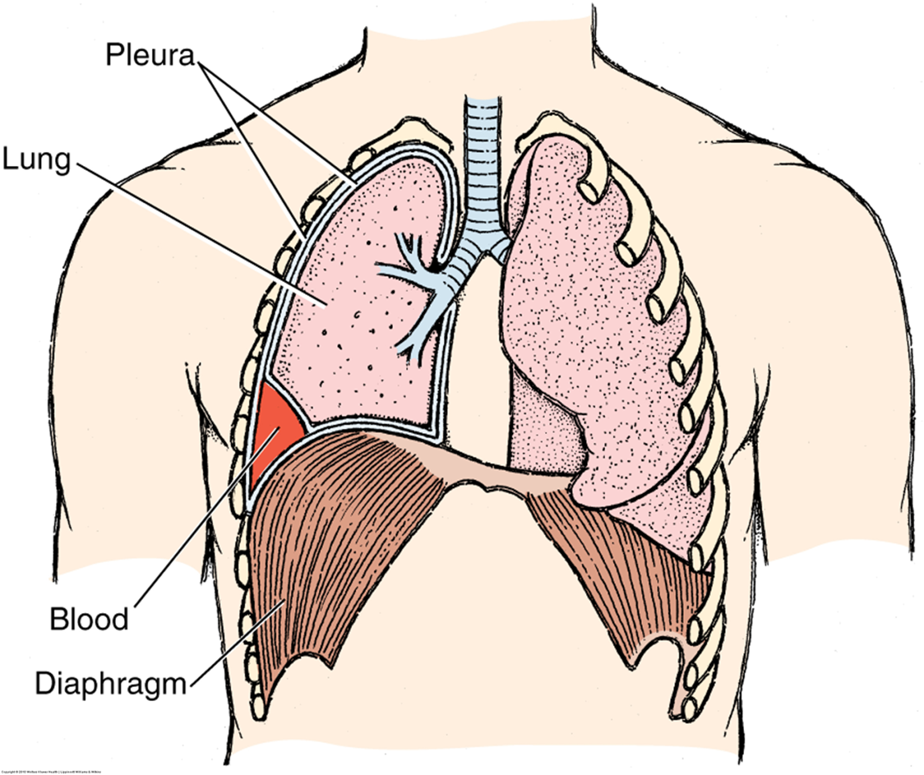
costodiaphragmatic recess
the lung fills the pleural recess during deep inspiration
clinical note: pathologic fluid may accumulate in the costodiaphragmatic recess
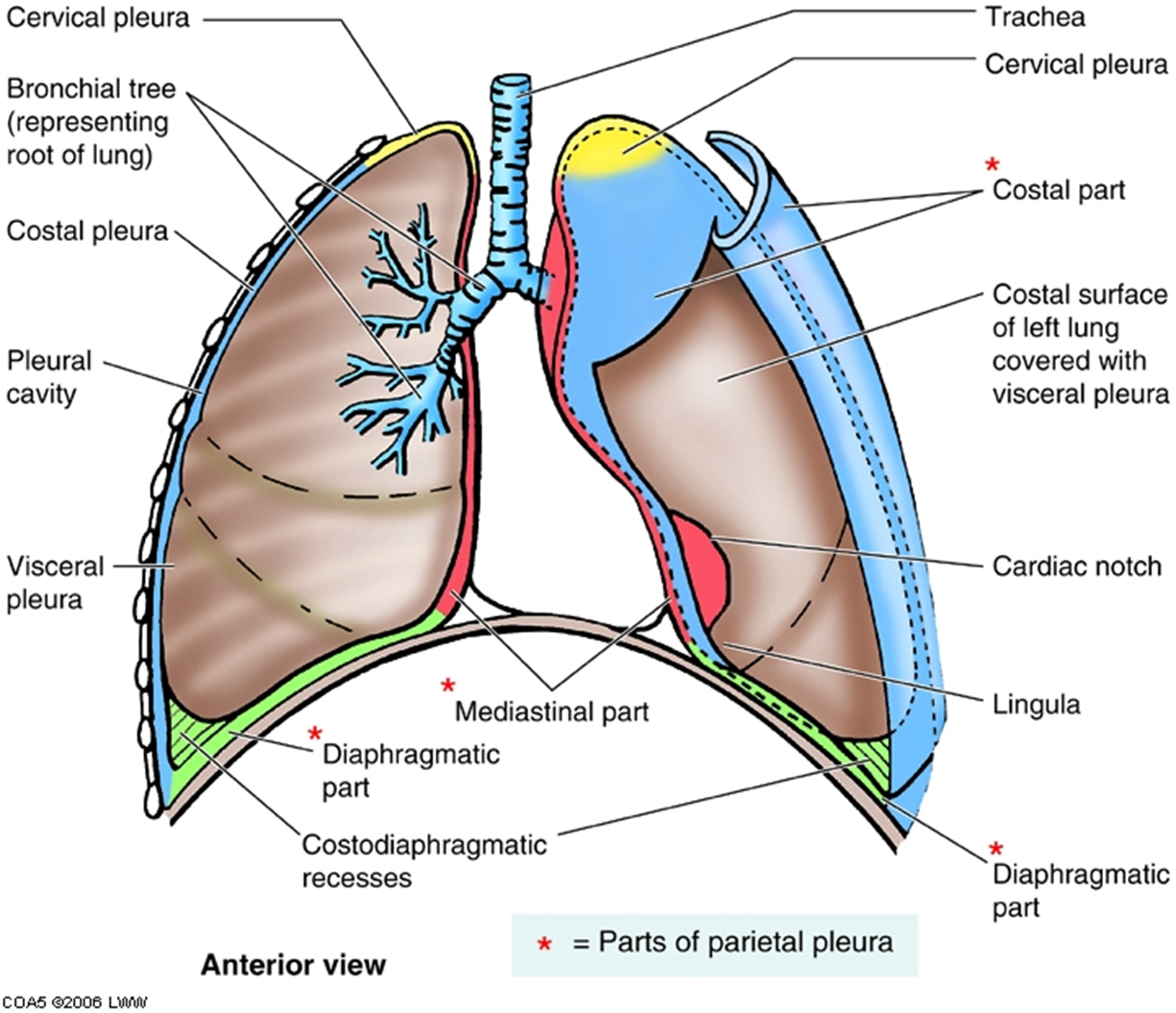
diff betwn parietal & visceral pleura
Parietal Pleura: The outer layer of pleura that lines the thoracic cavity.
It is innervated by somatic afferent fibers, hence capable of detecting pain.
This portion is in contact with the wall of the thorax and can be subdivided into regions such as cervical, costal, mediastinal, and diaphragmatic pleura.
Visceral Pleura: The inner layer of pleura that covers the lungs directly.
It is believed to be insensitive to pain as it lacks somatic afferent fibers, and it detects only stretch.
At the root of the lung, the visceral pleura is continuous w the parietal pleura.
vertical lines of thoracic wall
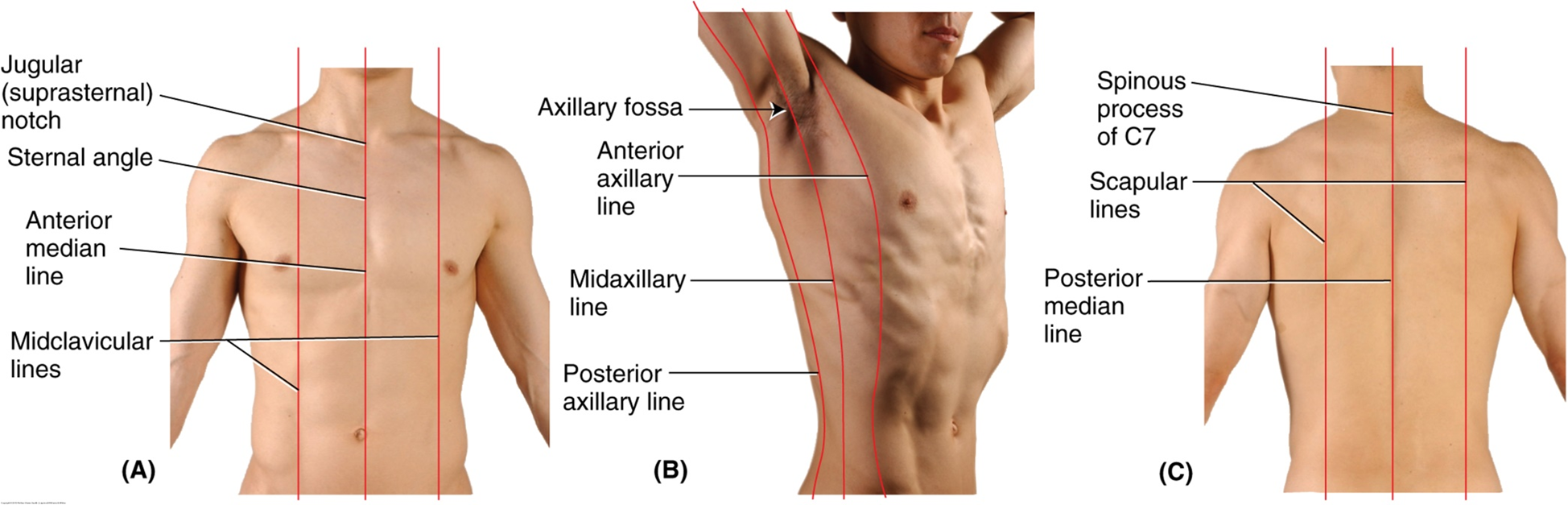
maybe he will explain why these are important, he just listed them, he didn’t really say anything about them
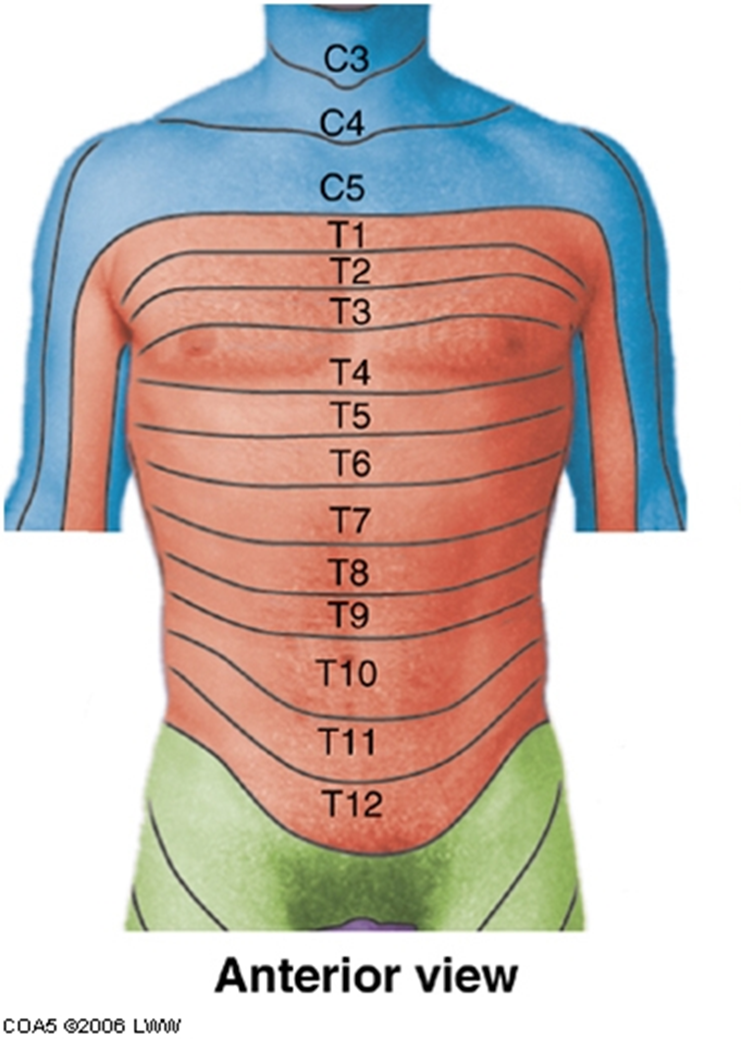
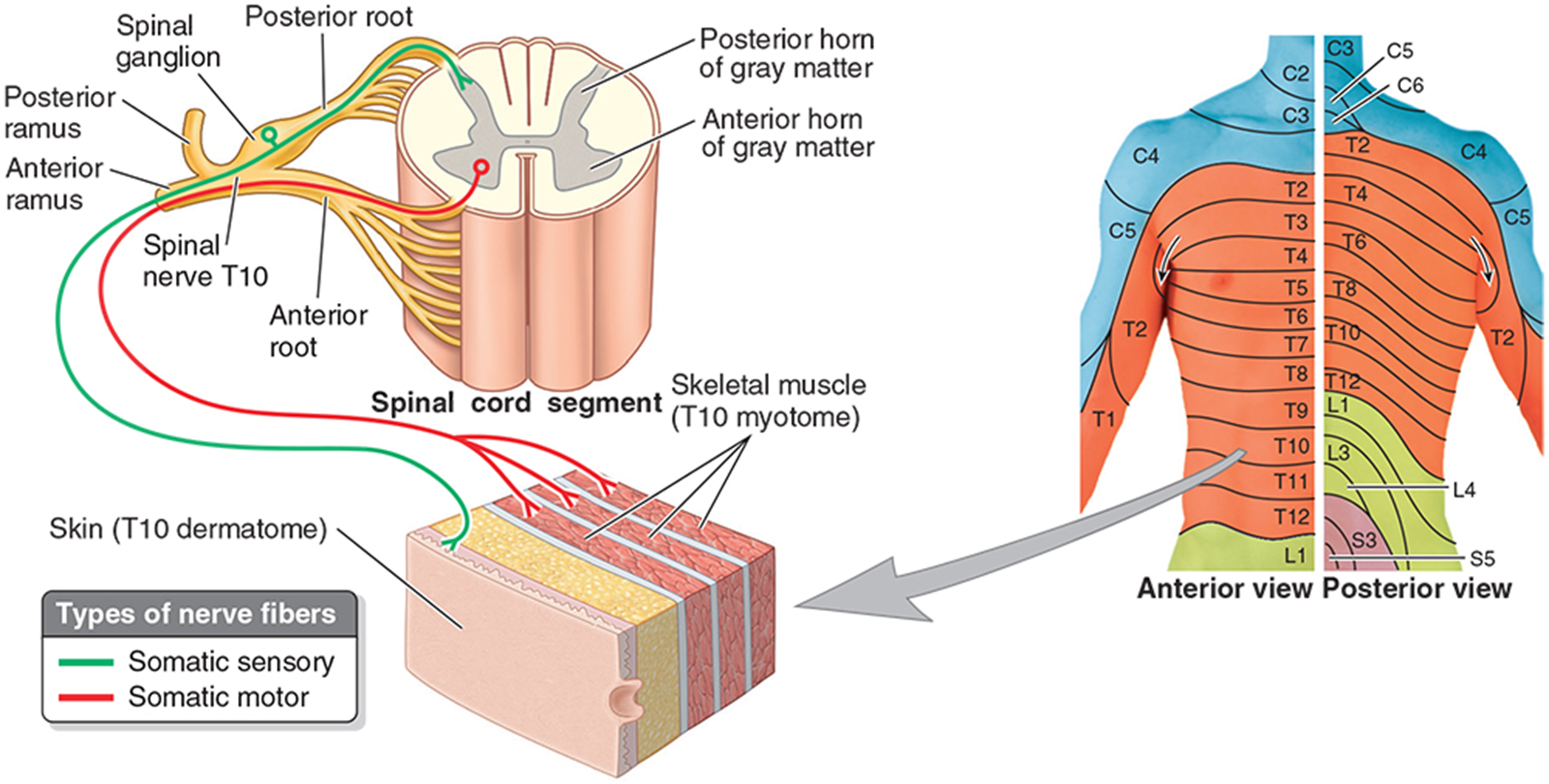
dermatomes
C3-C5 neck and shoulder
T4 nipple line
T6 xiphoid process
T10 umbilicus
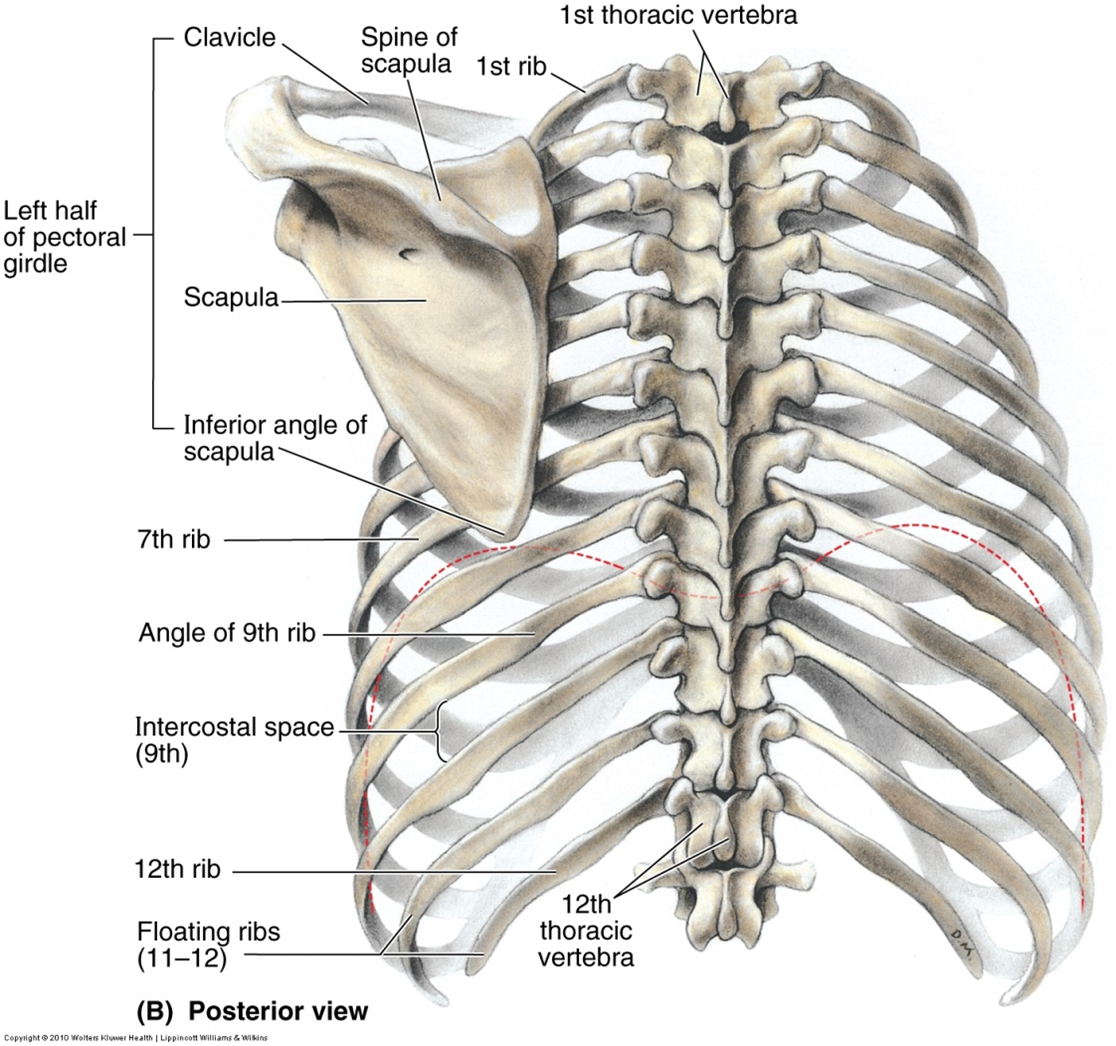
Thoracic skeleton
Sternum - manubrium, body largest portion, xiphoid process
12 thoracic vertebrae & intervertebral discs
12 pairs of ribs w costal cartilages
Rib classification:
True ribs (1-7) attach directly to sternum via costal cartilages.
False ribs (8-10) attach the costal margin.
Floating ribs (11 & 12) no anterior attachment. more susceptible to injury
costal margins
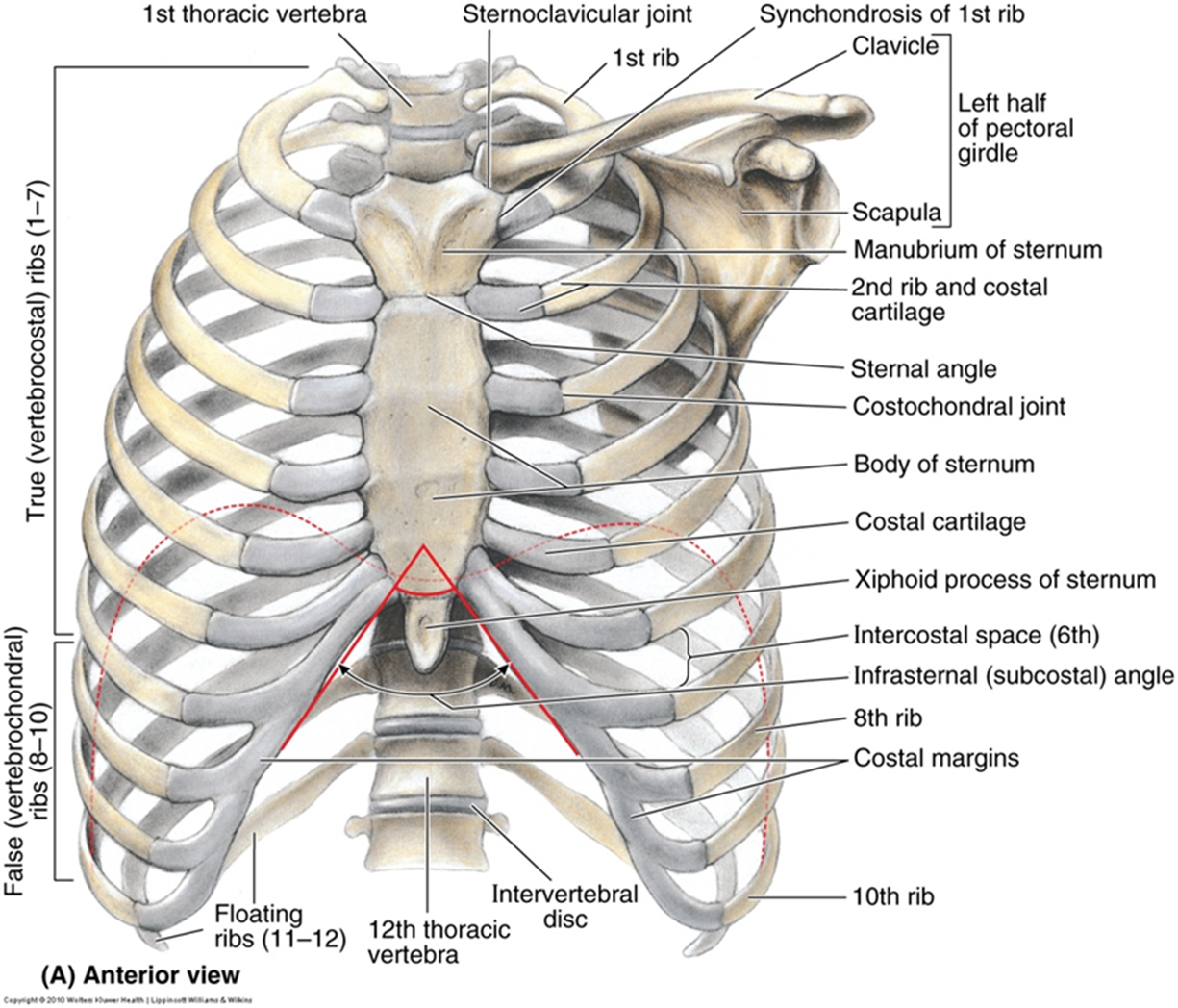
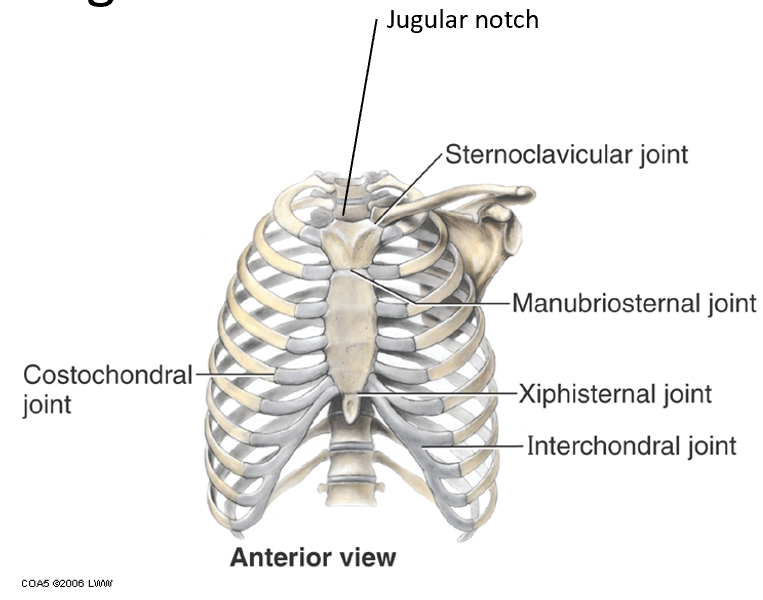
Landmarks of thoracic cage
•Jugular (suprasternal) notch depression @ top of manubrium @ top of sternum
•Manubriosternal joint – sternal angle (of Louis) is at level of second rib costal cartilage & T4-T5 IV disc.
•Xiphisternal joint – T9 vertebral level
Marks the superior limit of the liver, the central tendon of the diaphragm, & the inferior border of the heart
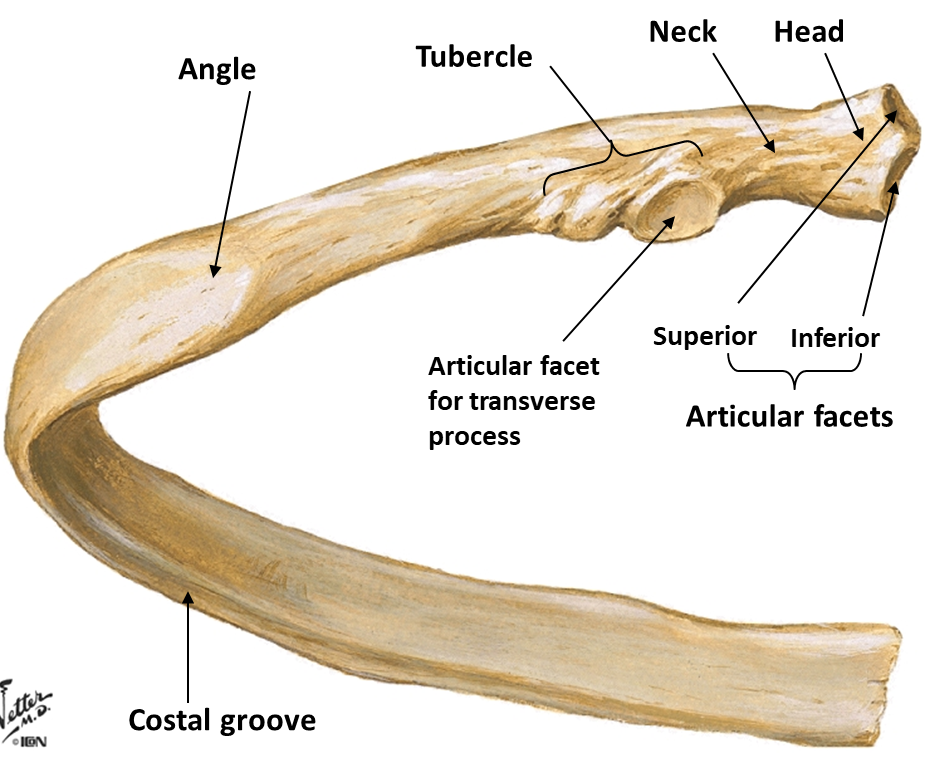
typical rib
Ribs 3-9 are typical and have the following features:
Head
Neck
Tubercle
Superior& inferior articular process
Body or shaft
Angle
Costal groove
Costal cartilage
clinical note: rib fractures typically occur near the costal angle (area of greatest curvature)
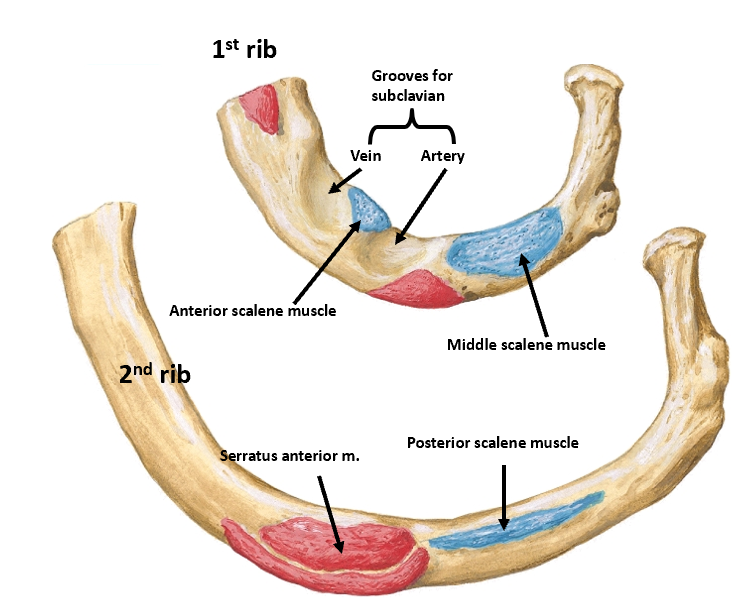
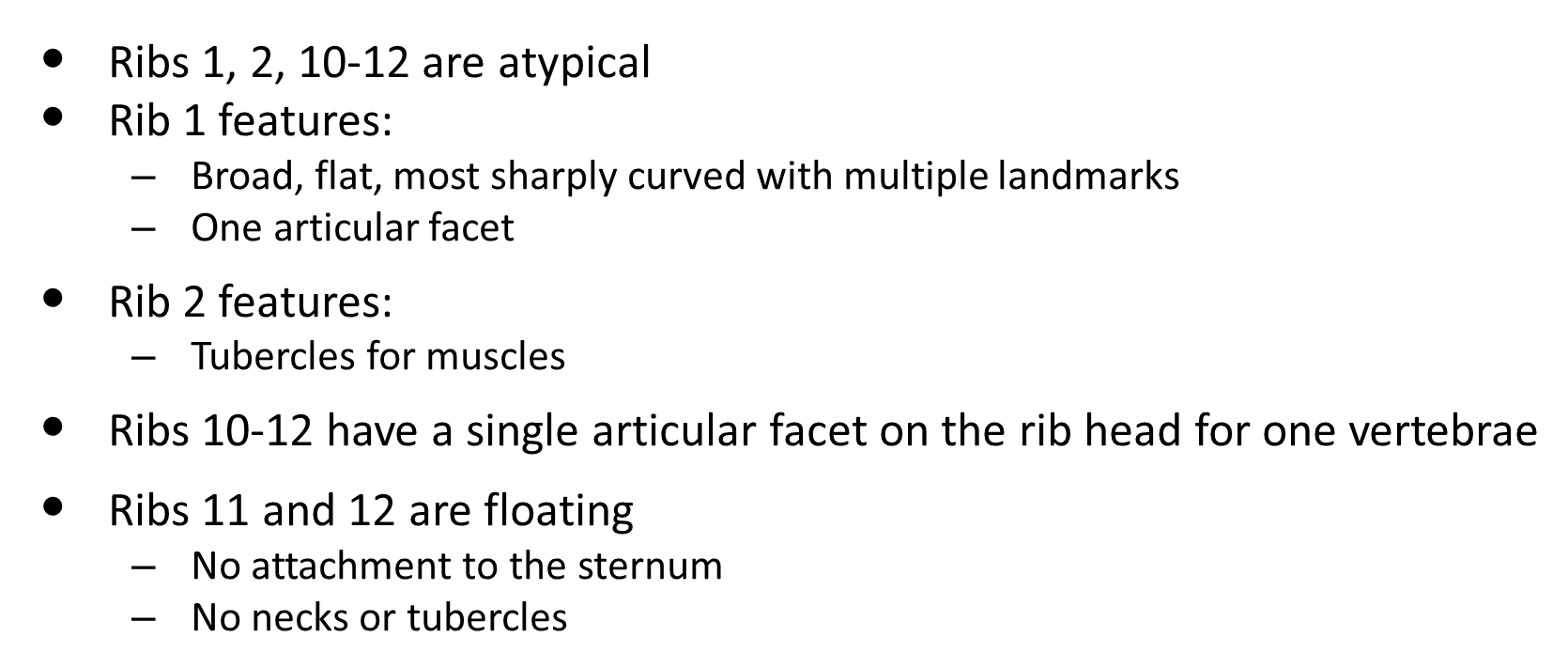
atypical ribs
•Ribs 1, 2, 10-12 are atypical
•Rib 1 features:
–Broad, flat, most sharply curved w multiple landmarks
–One articular facet
- anterior scalene attaches here, grooves for subclavian vein
•Rib 2 features: Tubercles for muscles
•Ribs 10-12 have a single articular facet on the rib head for one vertebrae
•Ribs 11 and 12 are floating
–No attachment to the sternum
–No necks or tubercles

/
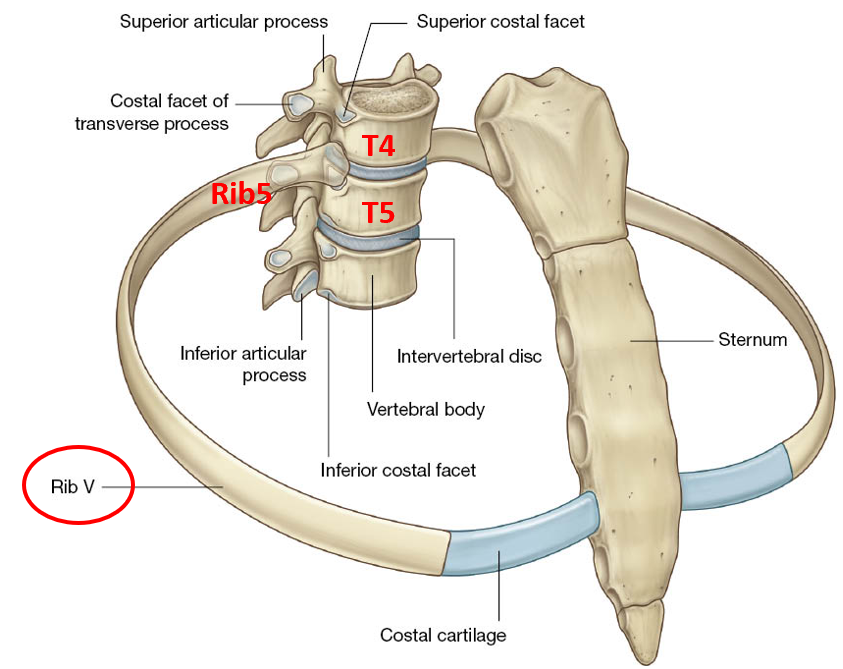
joints btwn vertebrae, ribs, sternum
a typical rib articulates w vertebra of same level & vertebrae above
Intercostal muscles
support intercostal spaces during respiration preventing billowing out during expiration & being drawn in during inspiration.
They act isometrically (without movement) during quiet respirations.
They also assist rib movements w forced respiration.
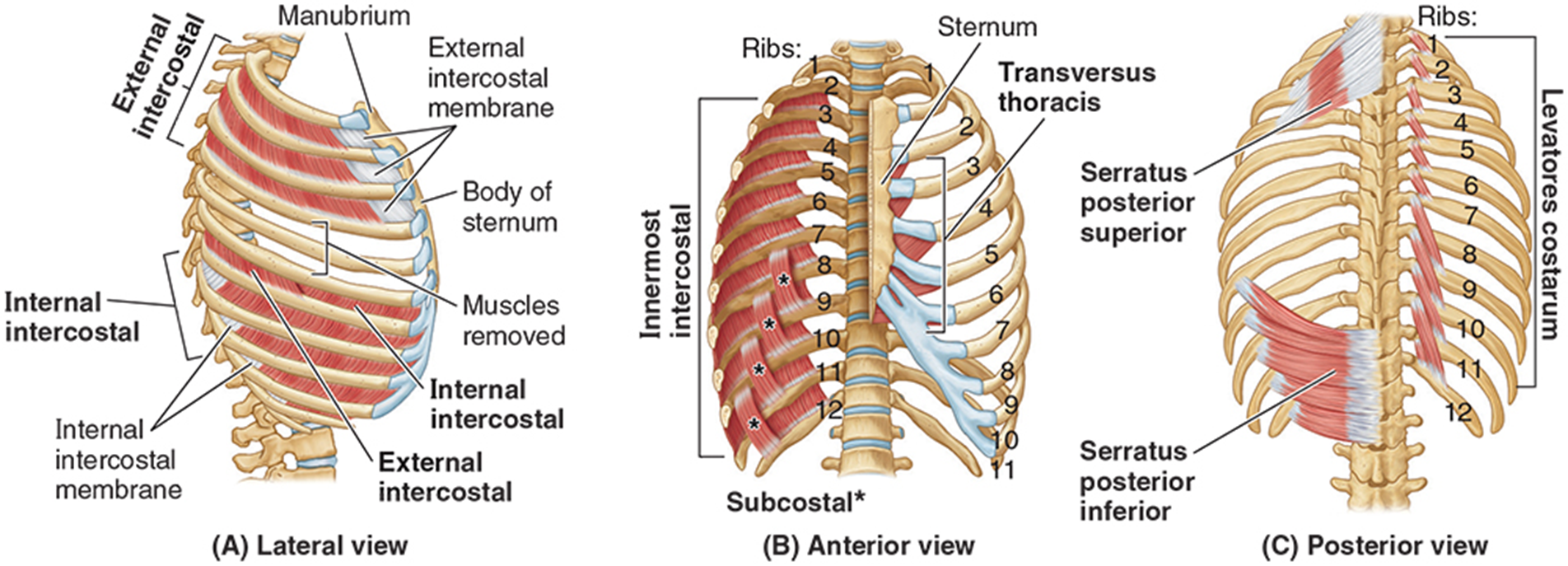
external intercostal point downward like putting hands in pockets, end in region where rib becomes costal cartilage
internal intercostal show fibers in opposite direction
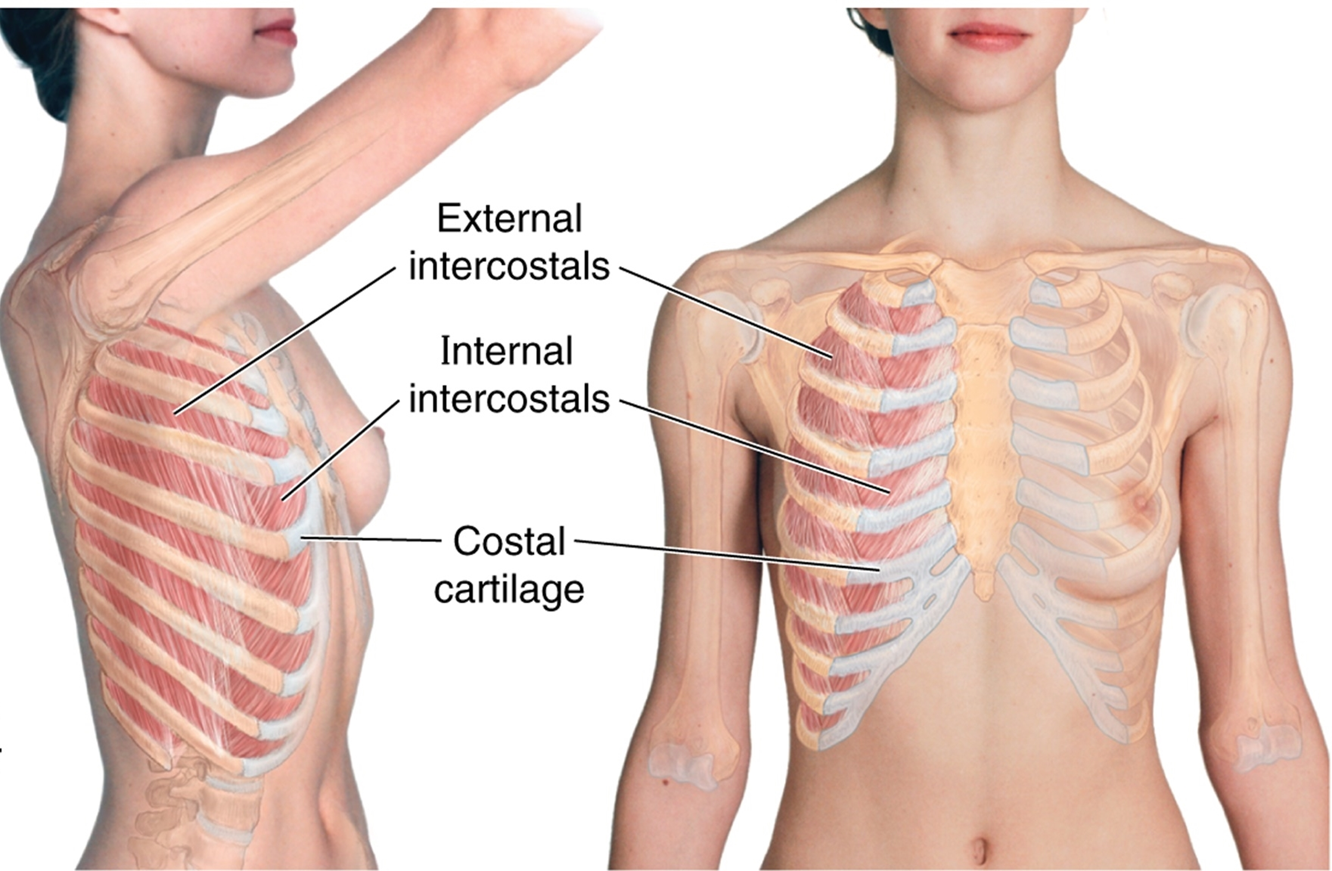
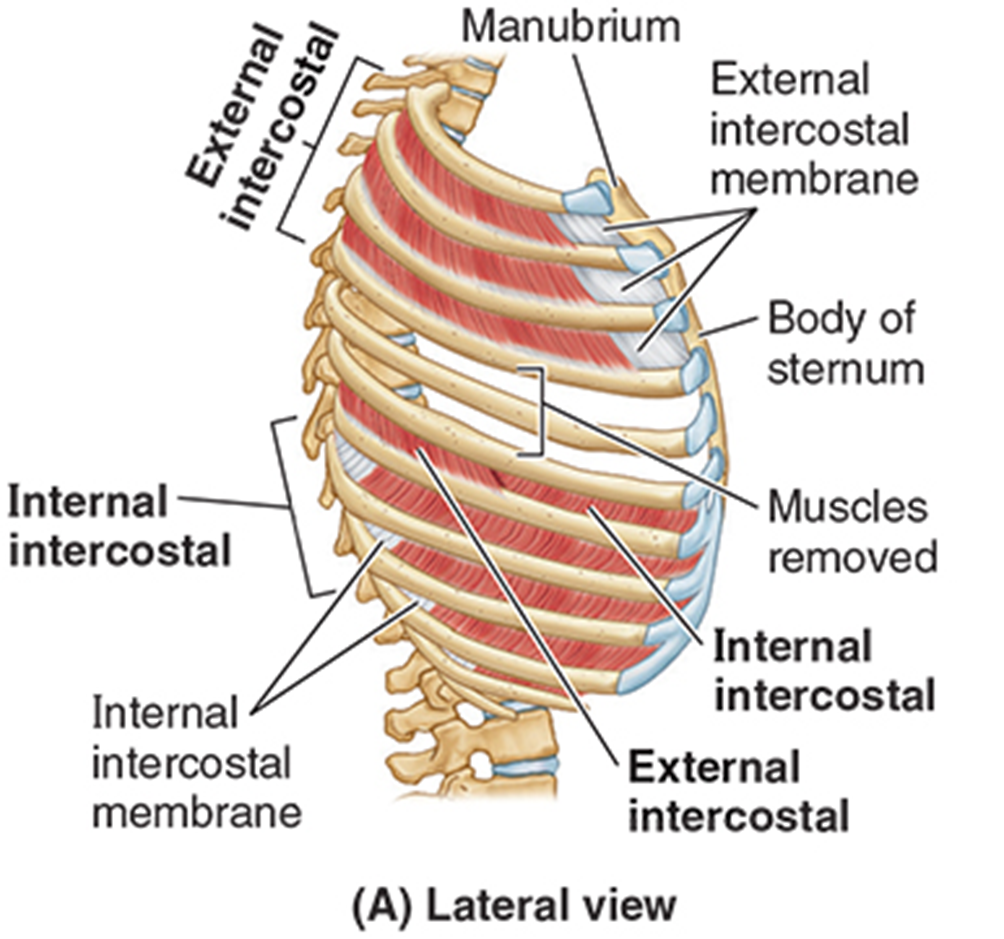
external intercostal muscles
Muscle fibers span from tubercles of ribs posteriorly to costochondral junction anteriorly & then continue as a membranous layer to the sternum.
Most active during inspiration to elevate ribs.
internal intercostal muscles
Muscle fibers run at a right angle to external intercostal muscles, from sternum to angle of the ribs, & continue posteriorly as a membrane layer.
deep to external intercostal muscles
Most active during expiration to depress ribs
innermost intercostal muscles
most evident in lateral region of internal thorax
help w exhalation
subcostal muscles
span 2-3 intercostal spaces posteriorly
both have same fiber direction of internal intercostal muscles
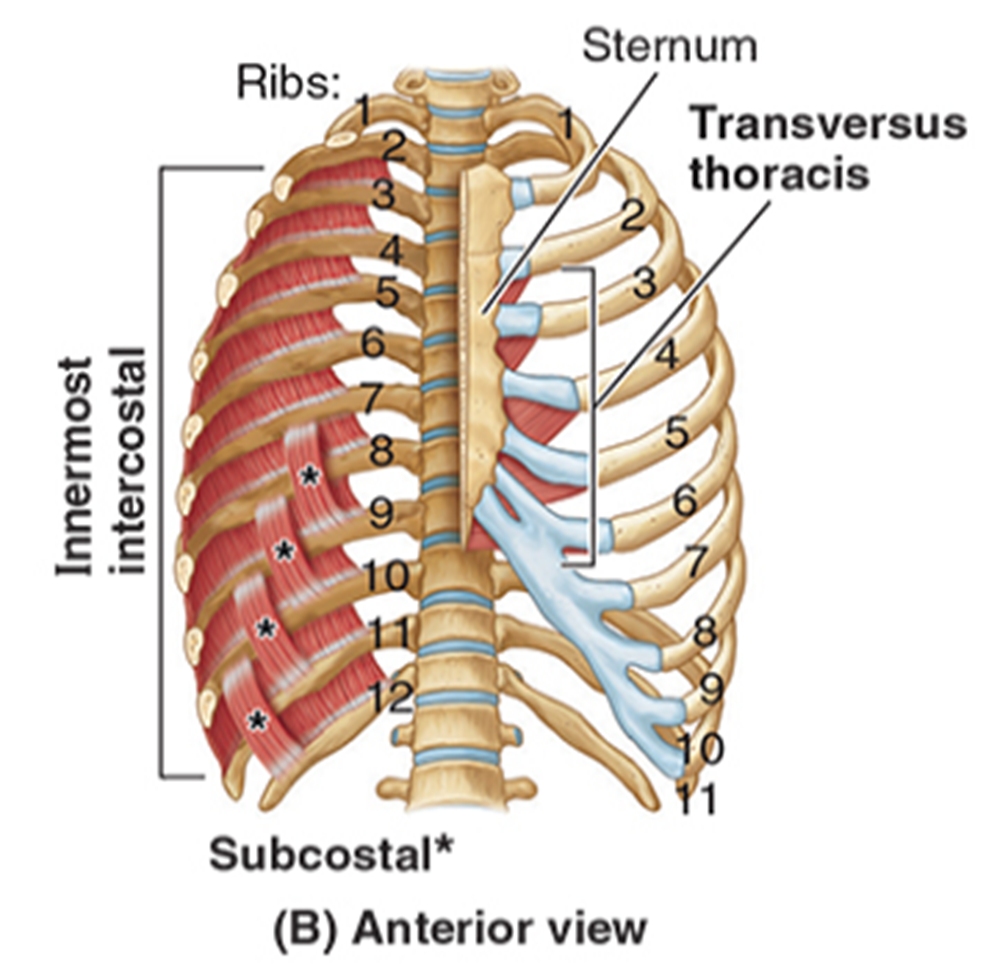
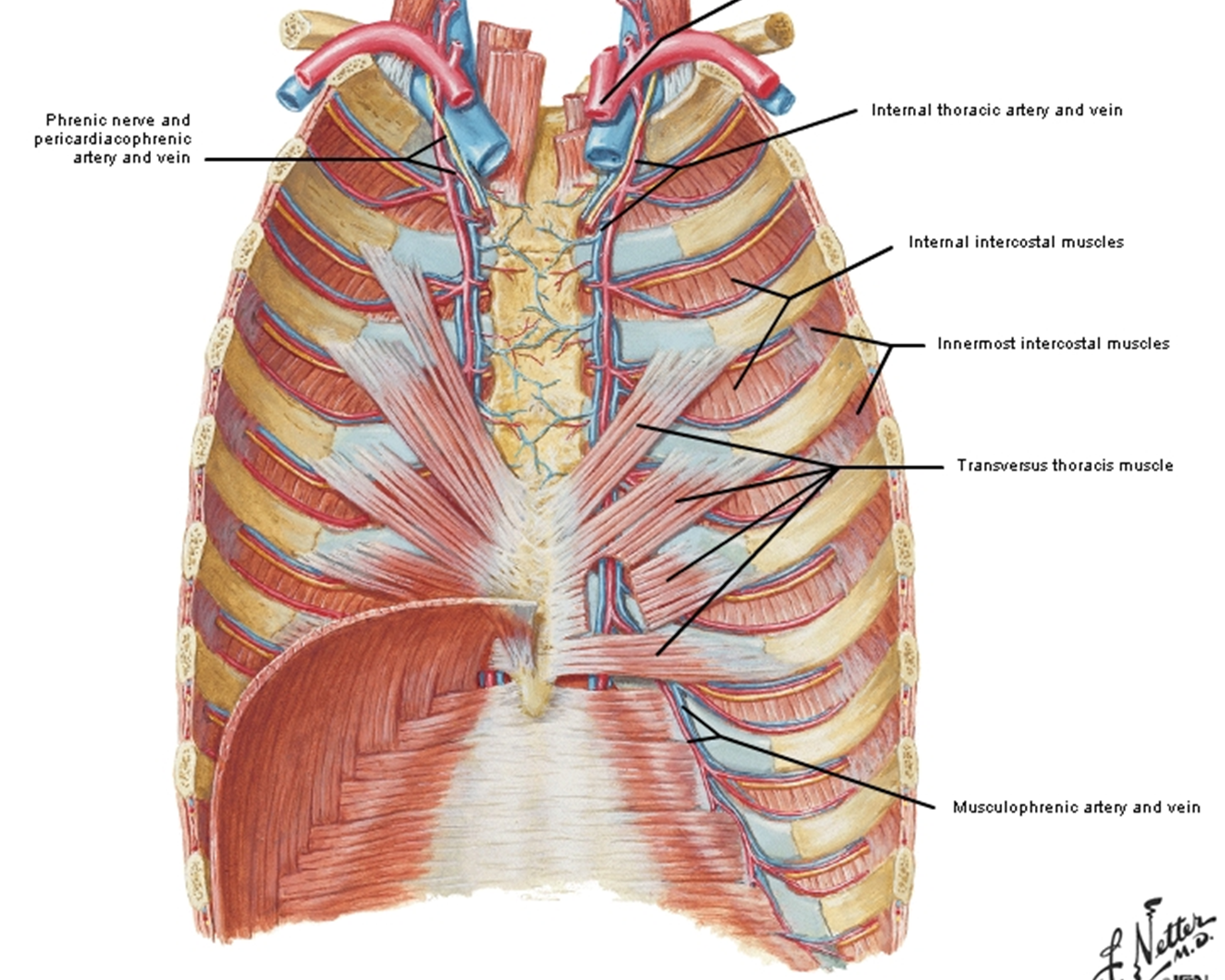
transversus thoracis muscles
Span more than one intercostal space from sternum to costal cartilage.
Continuous inferiorly w transversus abdominis muscle.
spans typically from ribs 3-6
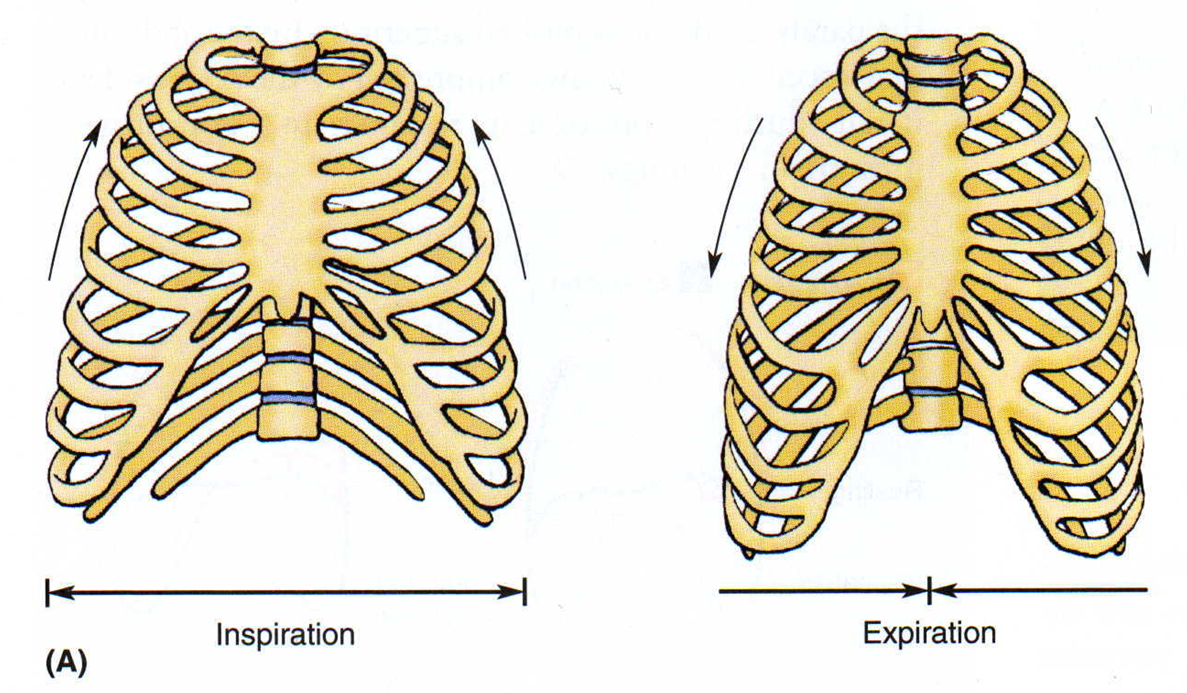
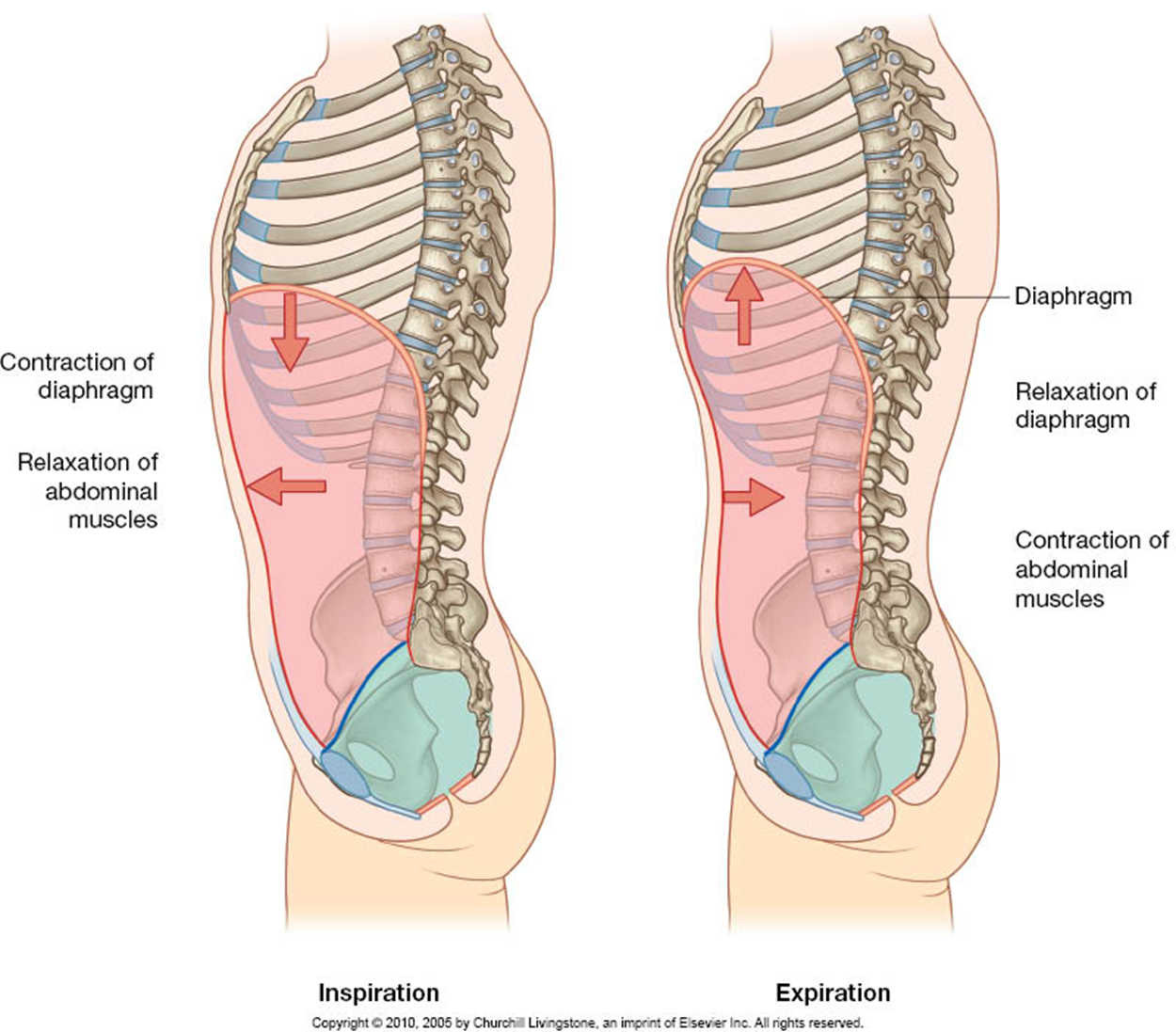
thoracic wall movement
During inspiration, the rib cage expands vertically, laterally, & in the anteroposterior dimension. active
During expiration the diaphragm relaxes, and the rib cage contracts. passive
lungs follow same pattern
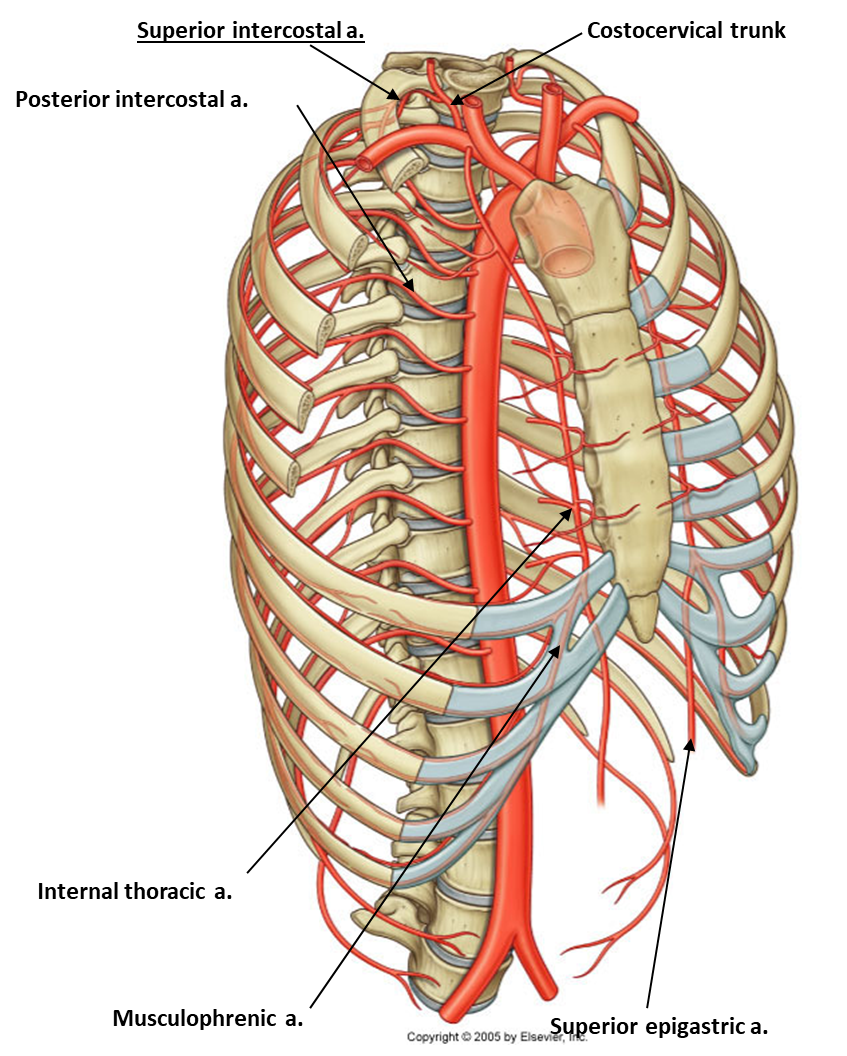
arterial supply
Posterior intercostal arteries
Mostly originate from the thoracic aorta
Anterior intercostal arteries
Originate from internal thoracic arteries for the upper spaces and;
Musculophrenic arteries for the lower spaces.
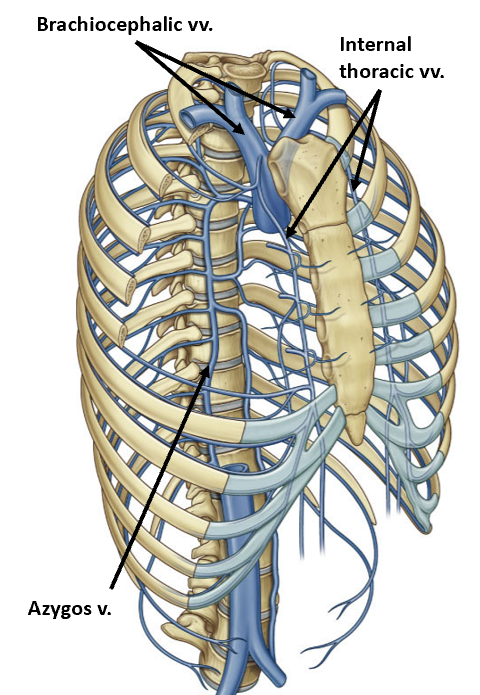
venous drainage
parallels arterial supply for most part
major exception: azygous venous system
Ultimately, blood drains back to the venous system via two routes.
Internal thoracic veins, which drain to brachiocephalic veins.
The azygos without a pair system of veins drain into the superior vena cava.
venous blood enters R siide of heart
intercostal nerves
11 intercostal nerves (anterior rami of T1 – T11) providing motor and sensory functions.
Subcostal nerve (anterior ramus of T12).
Collateral branches are found near the superior border of ribs.
Intercostal nerves contain sympathetic fibers to smooth muscle in the body wall blood vessels, hair follicles, and sweat glands.
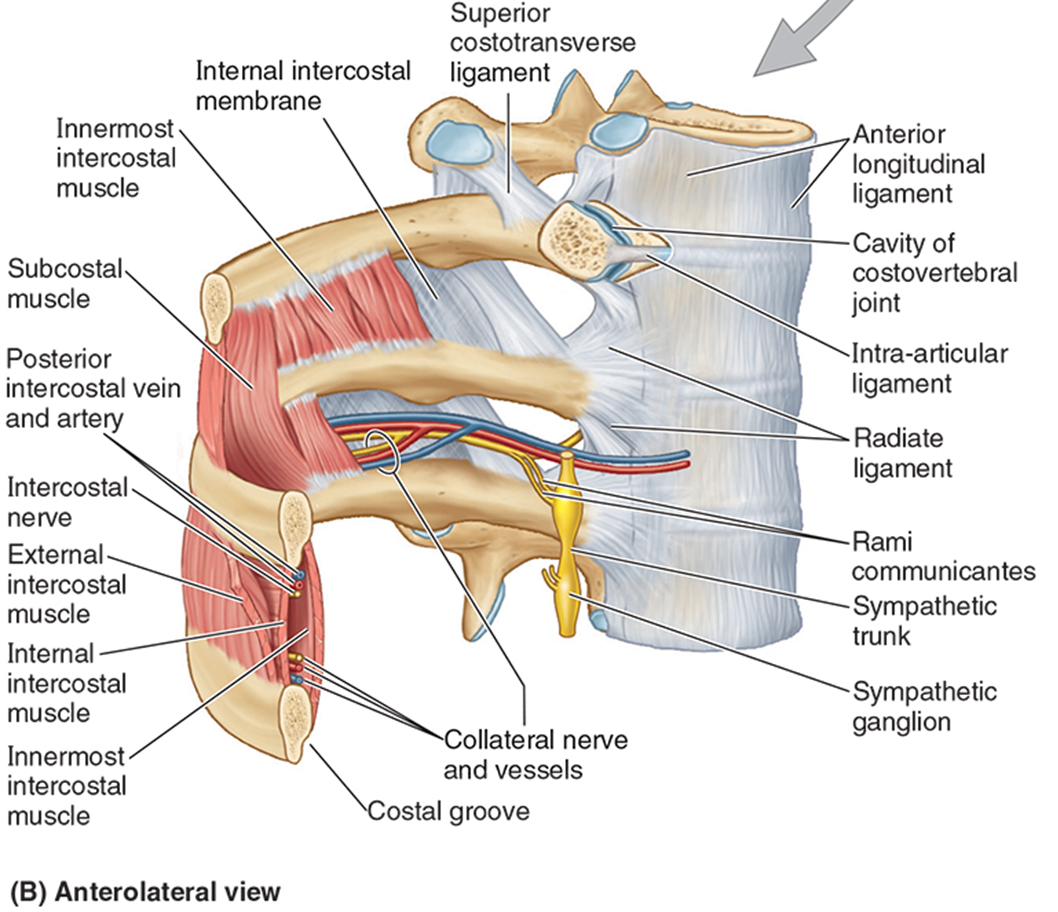
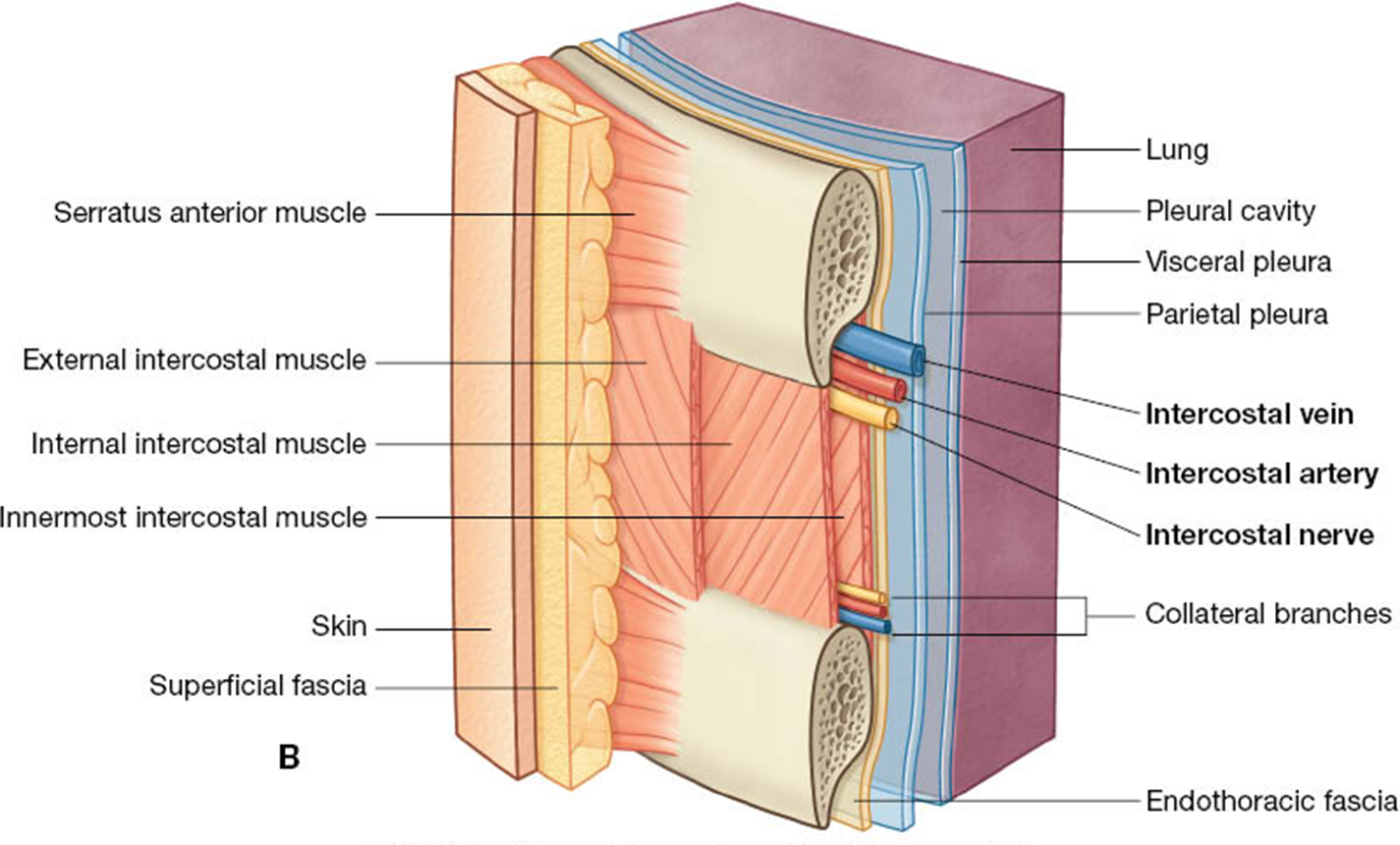
Intercostal vessels and nerves pass btwn the innermost and internal intercostal muscle layers.
intercostal muscle, nerve, & vessel relationships
the intercostal vessels & nerves pass btwn the innermost & internal intercostal muscles.
All intercostal muscles are innervated by intercostal nerves.
Collateral branches run superior to the ribs.
segmental dermatomes & myotomes of thorax
intercostal nerves segmentally innervate muscles of thorax & abdomen, & overlying skin
Intercostal vein artery and nerve (VAN)
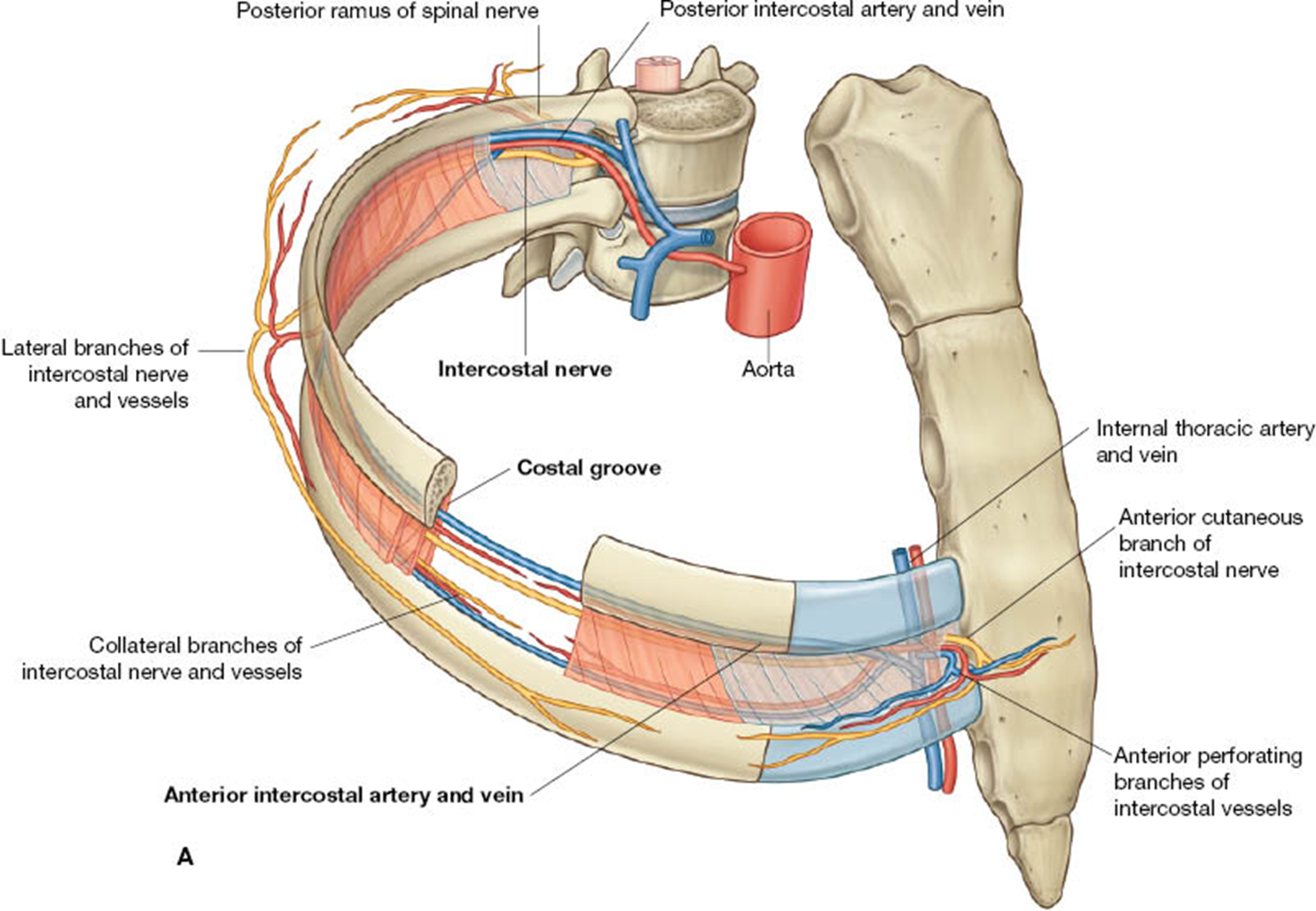
intercostal region
Intercostal vein, artery, nerve (VAN)
Skin, fascia, muscle layers, endothoracic fascia, parietal pleura
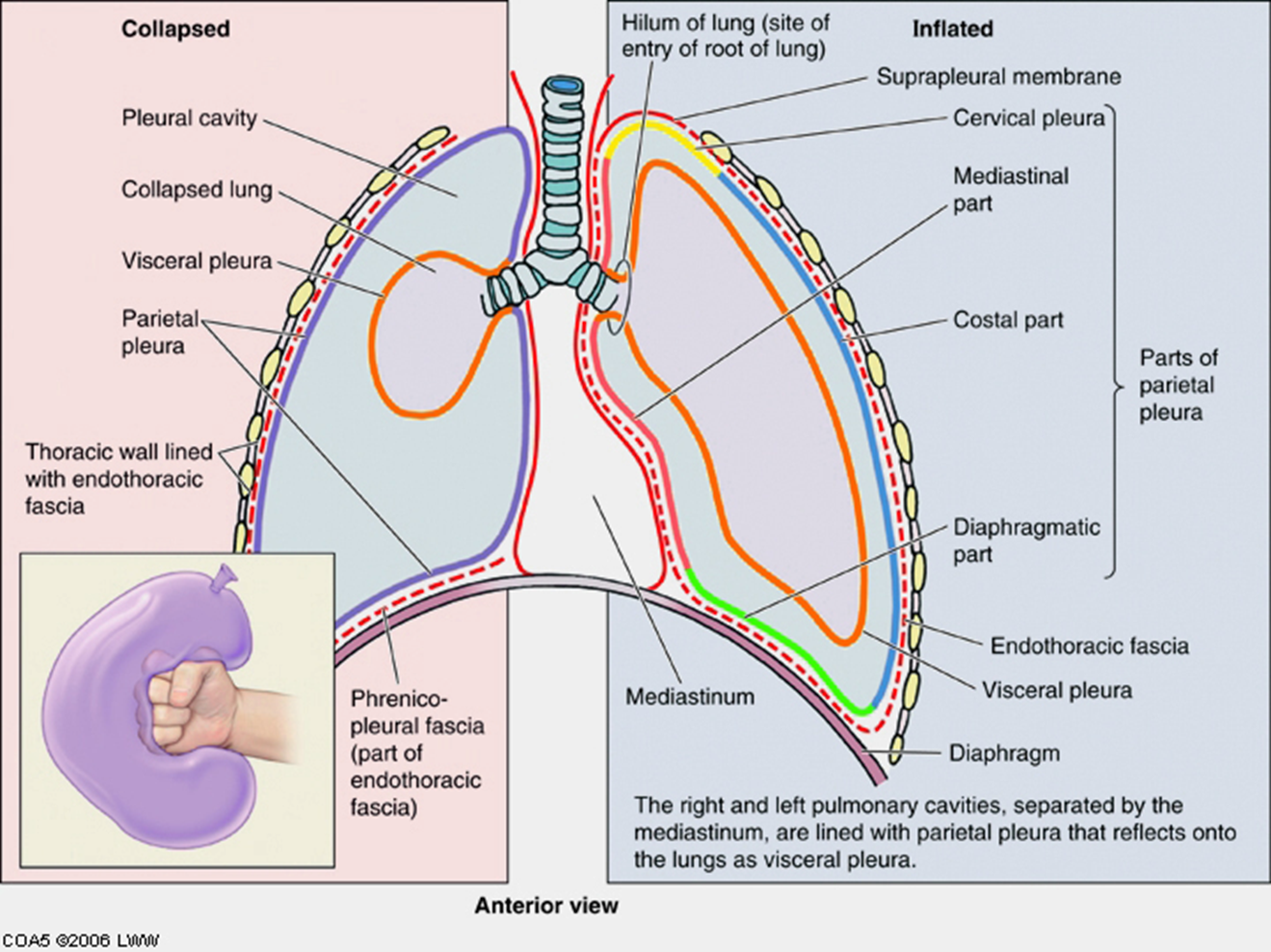
Pleura
pleural linings are best described by imagining your fist into a balloon
The part touching your fist is the visceral pleura.
The part outside is the parietal pleura.
The potential space between is the pleural cavity.
At your wrist (root of the lung), the visceral & parietal layers are continuous.
Note that your fist is outside of the balloon, just as the lung is outside of the pleural cavity.
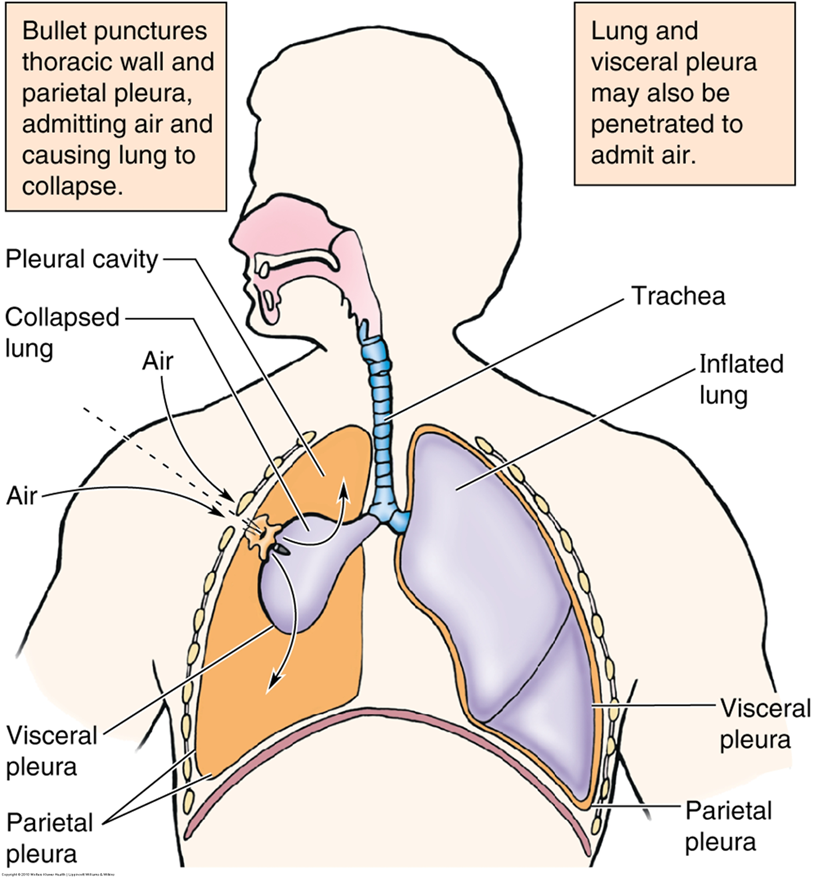
clinical note: pneumothorax & atelectasis
pneumothorax is the entry of air into the pleural cavity from either penetrating trauma or rupture of pulmonary lesion. This will cause a collapse of the lung (atelectasis).
After administering local anesthetic, a chest tube is inserted to promote drainage of air and inflation of lung.
clinical note: hemothorax
hemothorax is shown w blood in costodiaphragmatic recess
chest tube often inserted to drain fluid
parts of perietal pleura
Cervical pleura
Costal
Mediastinal
Diaphragmatic
Pleural recesses
clinical note & pleurisy
Parietal pleura is innervated by somatic afferent fibers and may produce local pain or referred pain.
The costal pleura is innervated by branches from the intercostal nerves. Pain would be felt in relation to the dermatomes of thoracic and abdominal walls.
The diaphragmatic pleura and the mediastinal pleura are innervated by the phrenic nerve. Pain would refer to the C3, C4, and C5 dermatomes – lateral neck and supraclavicular region.
Visceral pleura is believed to be insensitive to pain. Afferents detect stretch.
Pleuritis (pleurisy) inflammation of the pleura will cause a sharp stabbing pain of the chest wall upon inspiration. A friction rub can be auscultated. Adhesions between parietal and visceral pleura may form.
plerua recess & reflections
Visceral and parietal pleura are separated in regions that are not occupied by lungs during quiet respiration, resulting in recesses or potential spaces. These recesses allow for lung expansion during forced inspiration.
Clinically, the most important is the costodiaphragmatic recess. This recess enlarges during expiration.
Pathological collections of fluid may pool here when patient is upright.
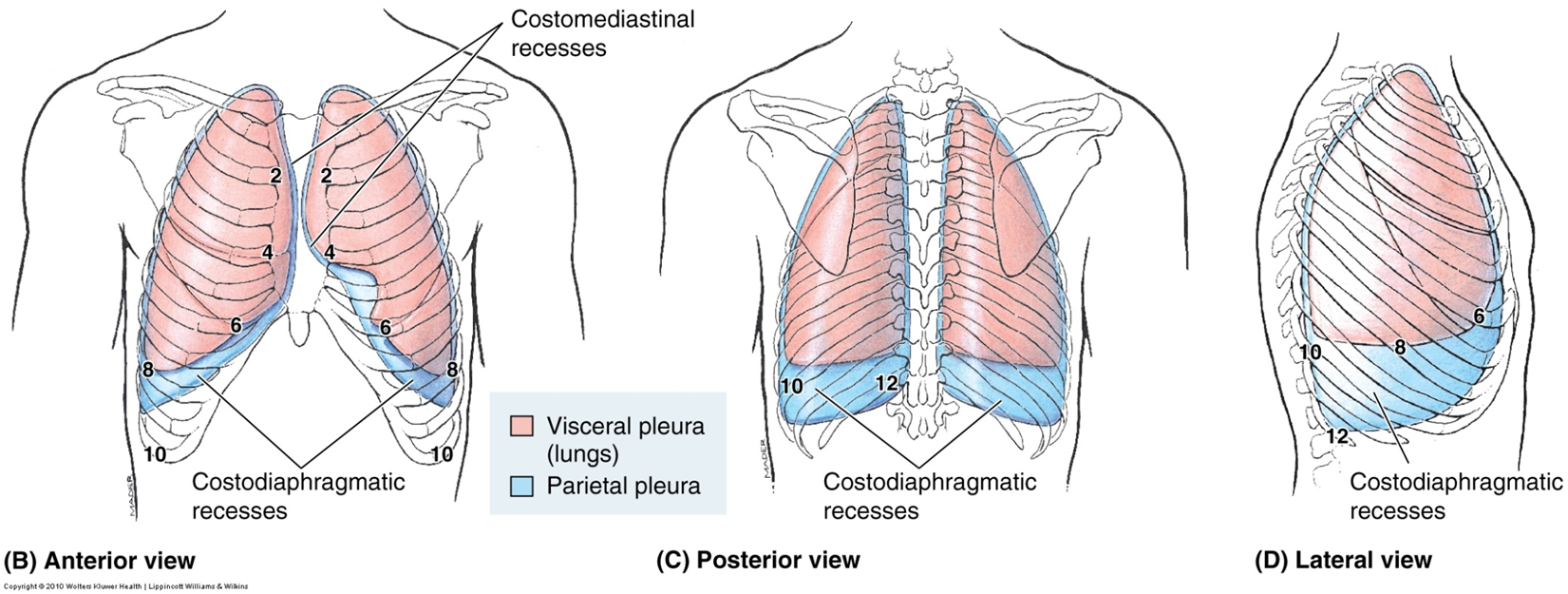
inferior extent of lung/visceral pleura and parietal pleura during normal respiration
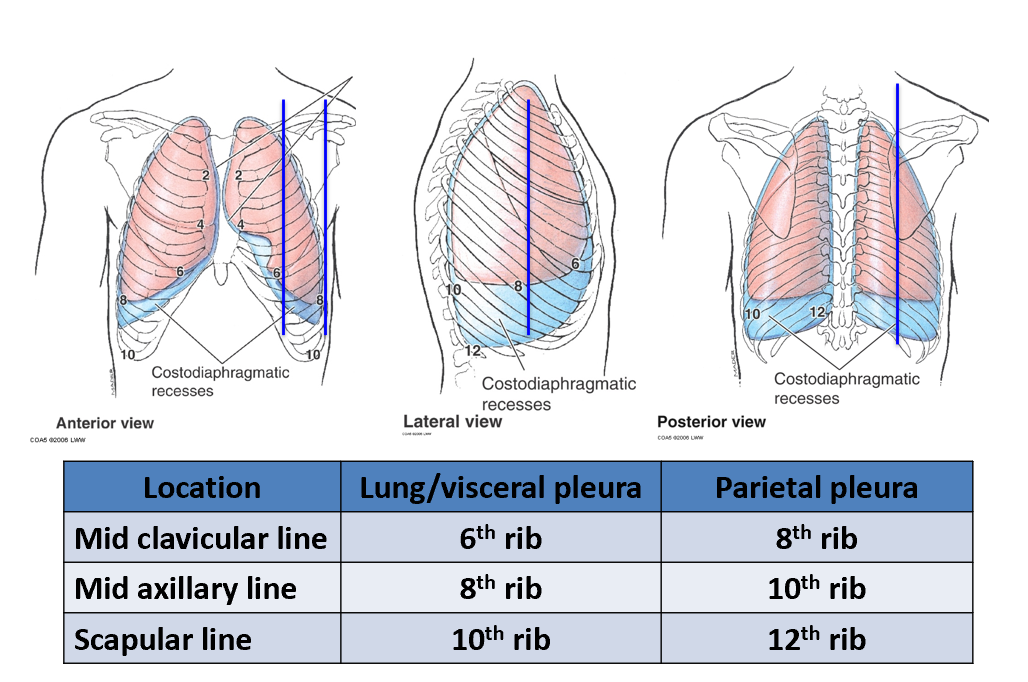
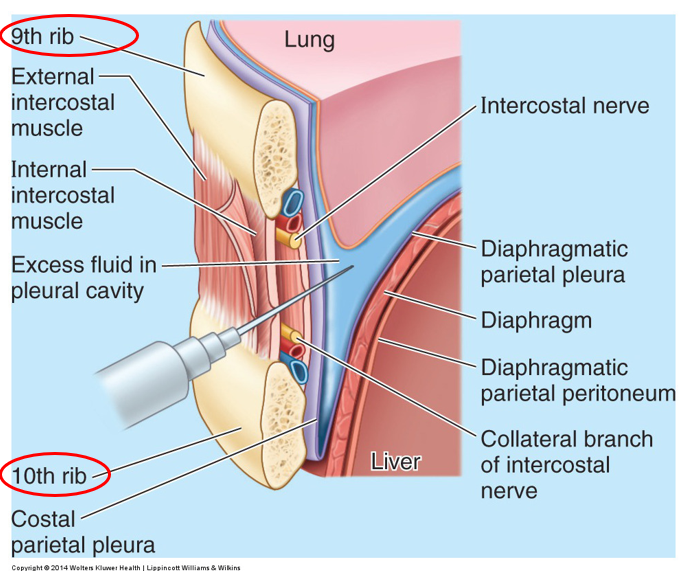
clinical note: thoracentesis for pleural effusion
Fluid collection from costodiaphragmatic recess from the 9th ICS midaxillary line in a patient sitting upright. Note proximity to the liver.
lung basics
2 lungs.
Organs of respiration on either side of the mediastinum.
Surrounded by pleural cavities.
Air enters and leaves via main bronchi.
Apex projects above 1st rib.
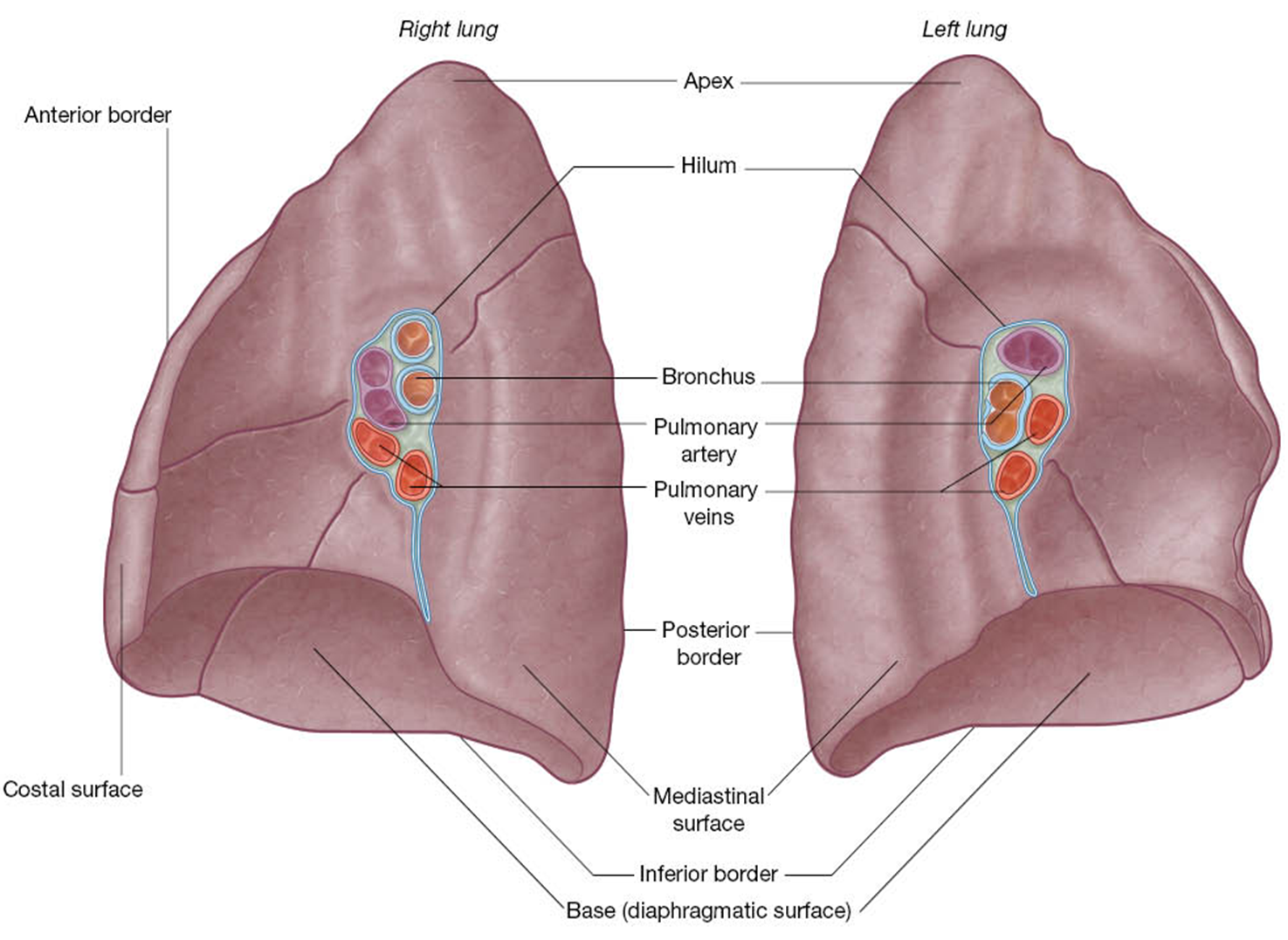
Base sits on diaphragm.
Costal and mediastinal surfaces.
Borders: anterior, posterior, and inferior.
Root of the lung enters at the hilum
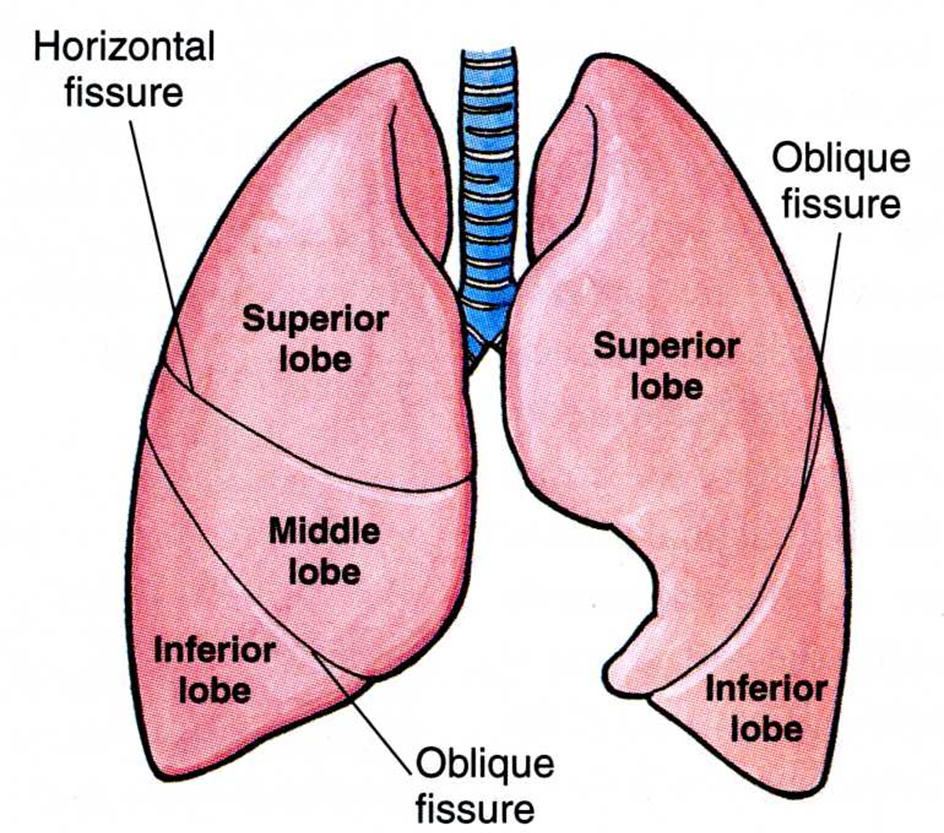
lobes & fissures of lungs
The right lung has 3 lobes. They are separated by a horizontal and oblique fissure.
The left lung has 2 lobes that are separated by an oblique fissure.
The lingula is an extension of the superior lobe of left lung.
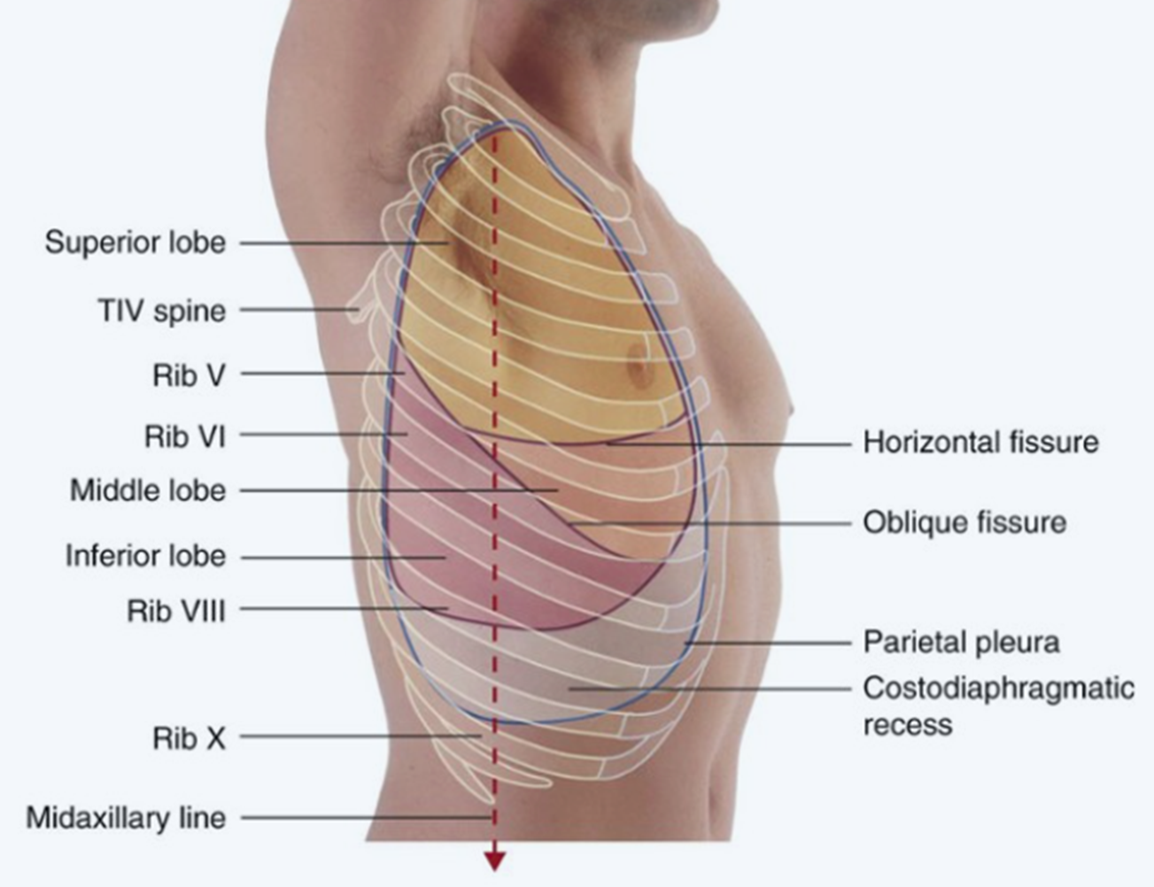
fissures & surface landmarks
Oblique fissure begins at level of the spine of T2/T4, passes 5th ICS at midaxillary line (MAL), then follows contour of rib 6 anteriorly.
The horizontal fissure extends from the oblique fissure, crosses rib 5 MAL then follows the contour of rib 4 anteriorly.
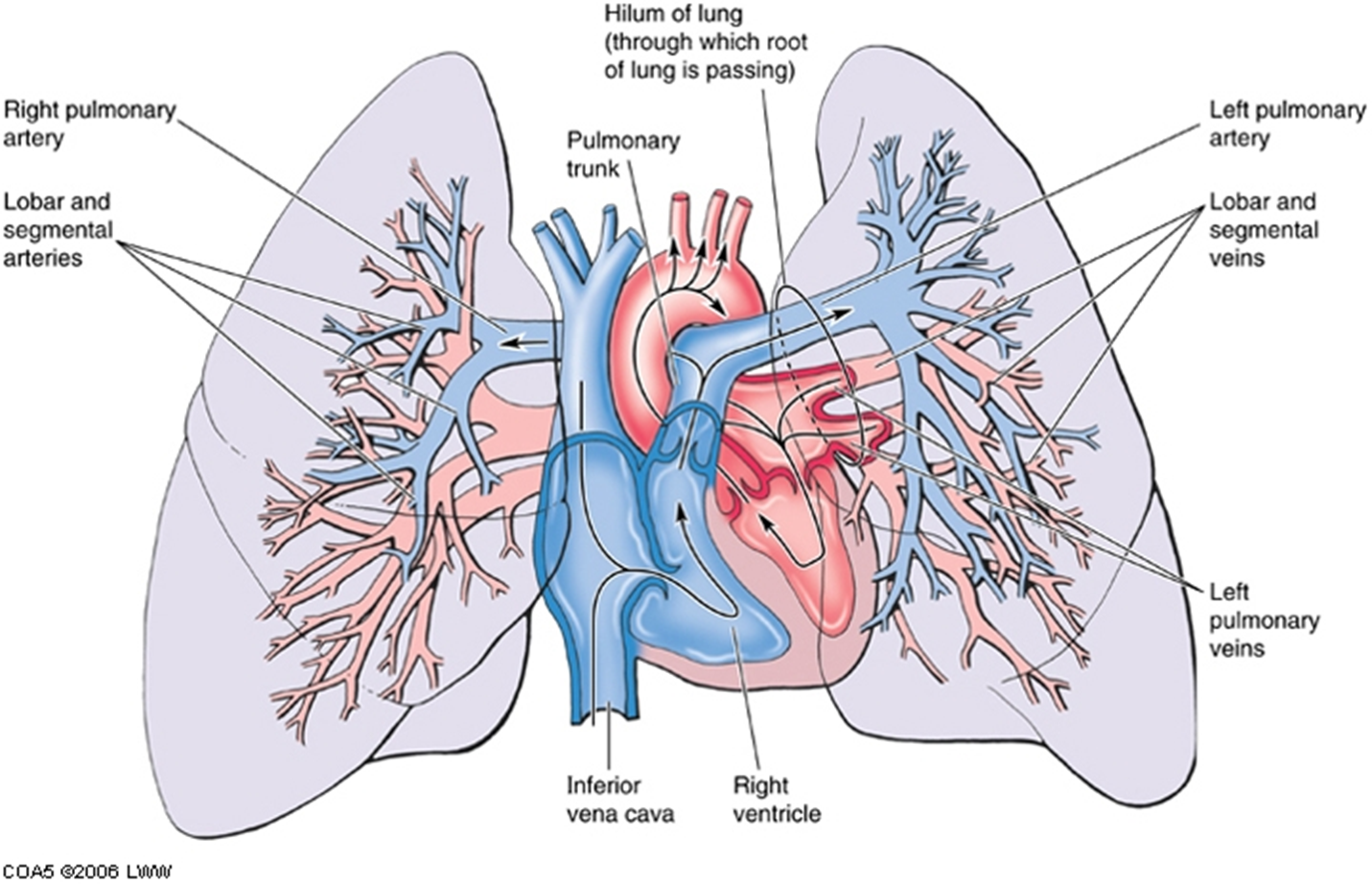
pulmonary arteries & veins
Each lung has one pulmonary artery supplying it, and two pulmonary veins draining it.
A segmental artery is usually anterior to the bronchus.
Each lung also has bronchial arteries and veins.
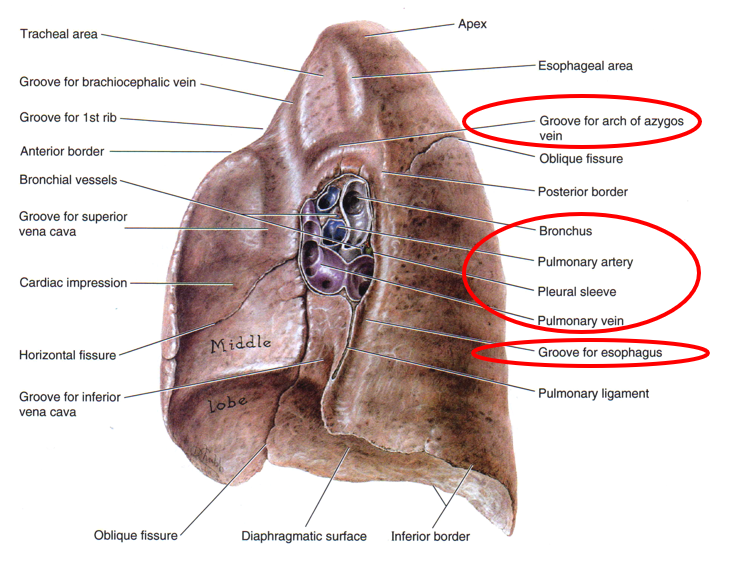
R lung mediastinal surface
The root of the lung is made up of the bronchi & pulmonary vessels. These structures enter and exit at the hilum of the lung.
The pulmonary ligament, double layer of pleura, permits movement during respiration.
The grooves and impressions shown on the cadaver lung illustration are artifacts of embalming. They demonstrate important relationships.
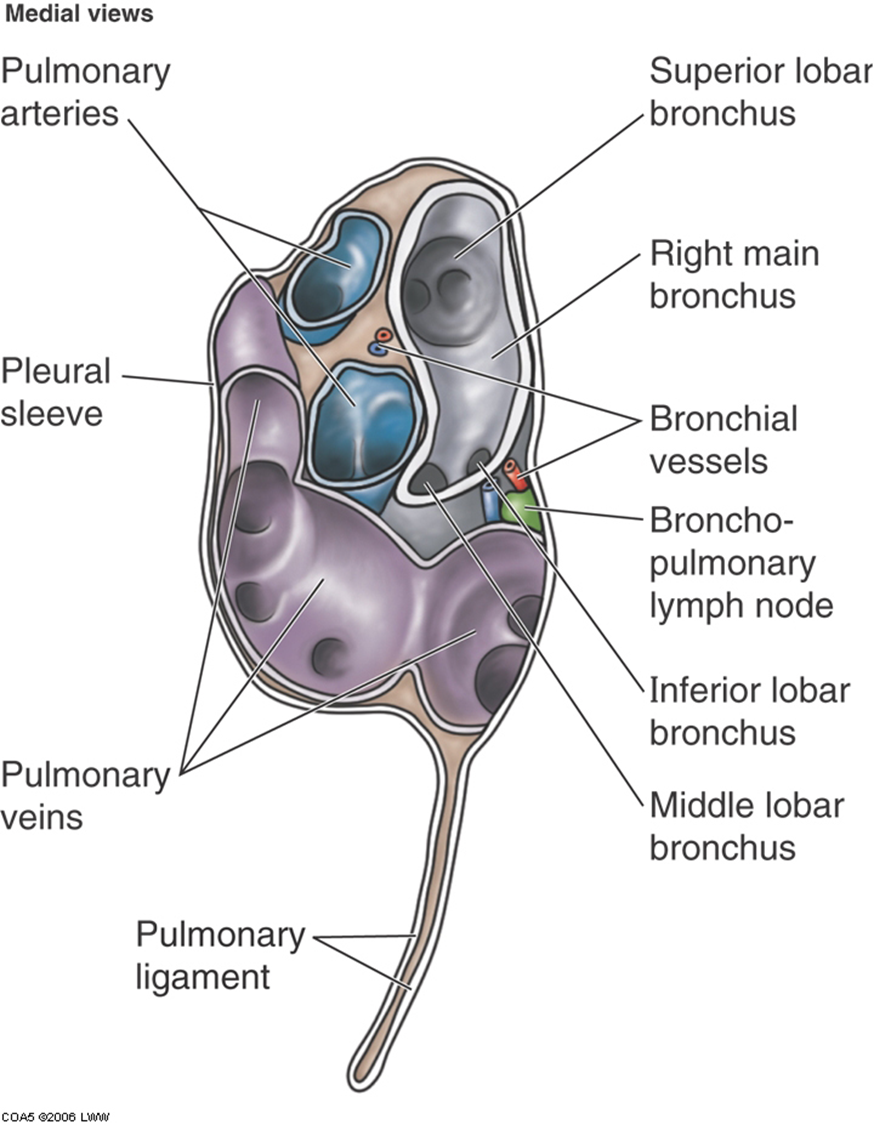
At the hilum of the right lung, the bronchus to the superior lobe has branched from the main bronchus and thus it is superior to the pulmonary artery.
The combined bronchus to the middle and inferior together is inferior to the pulmonary artery.
The pulmonary veins are most inferior.
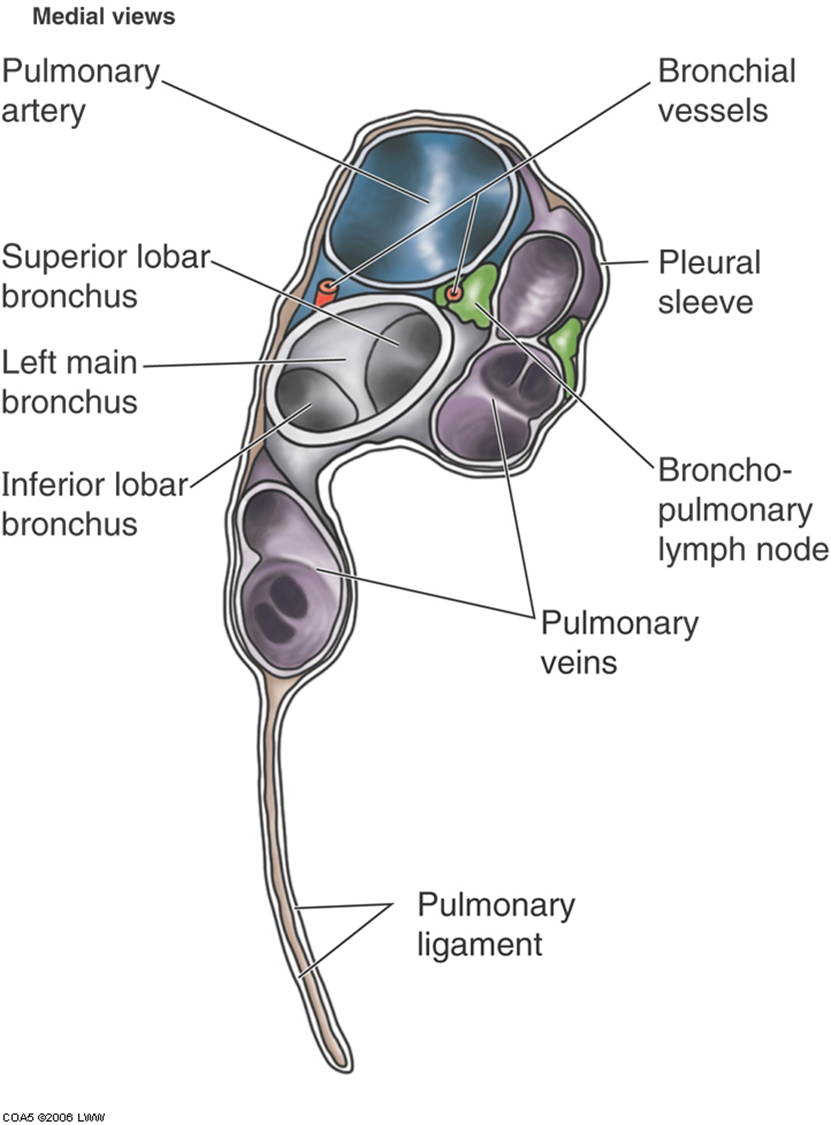
L lung mediastinal surface
On the left lung, the main bronchus is inferior to the pulmonary artery.
The veins are anterior and inferior to the other structures.
Bronchial vessels can also be seen.
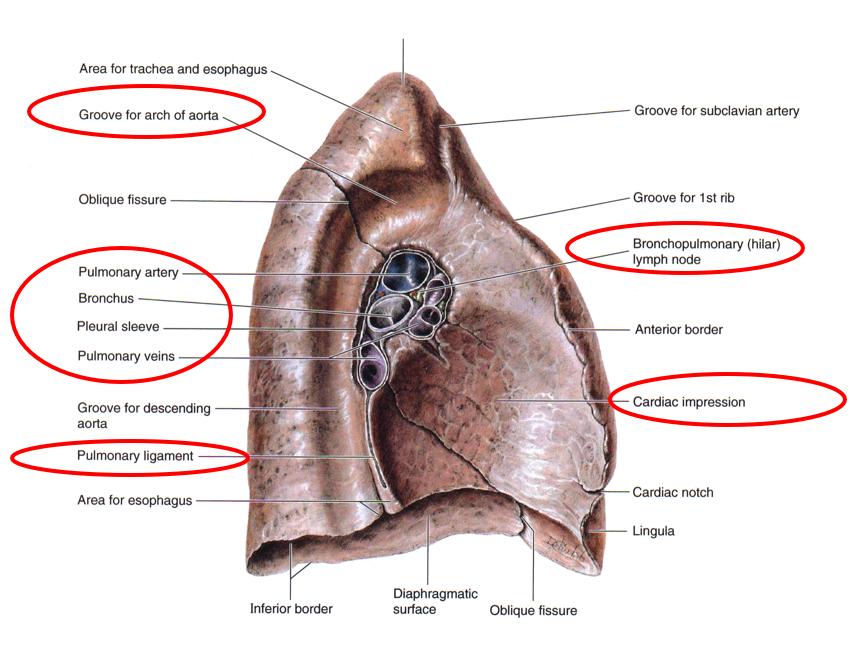
Notice the arrangement of the vessels and bronchi at the root of the lungs.
Note the lung borders and surfaces.
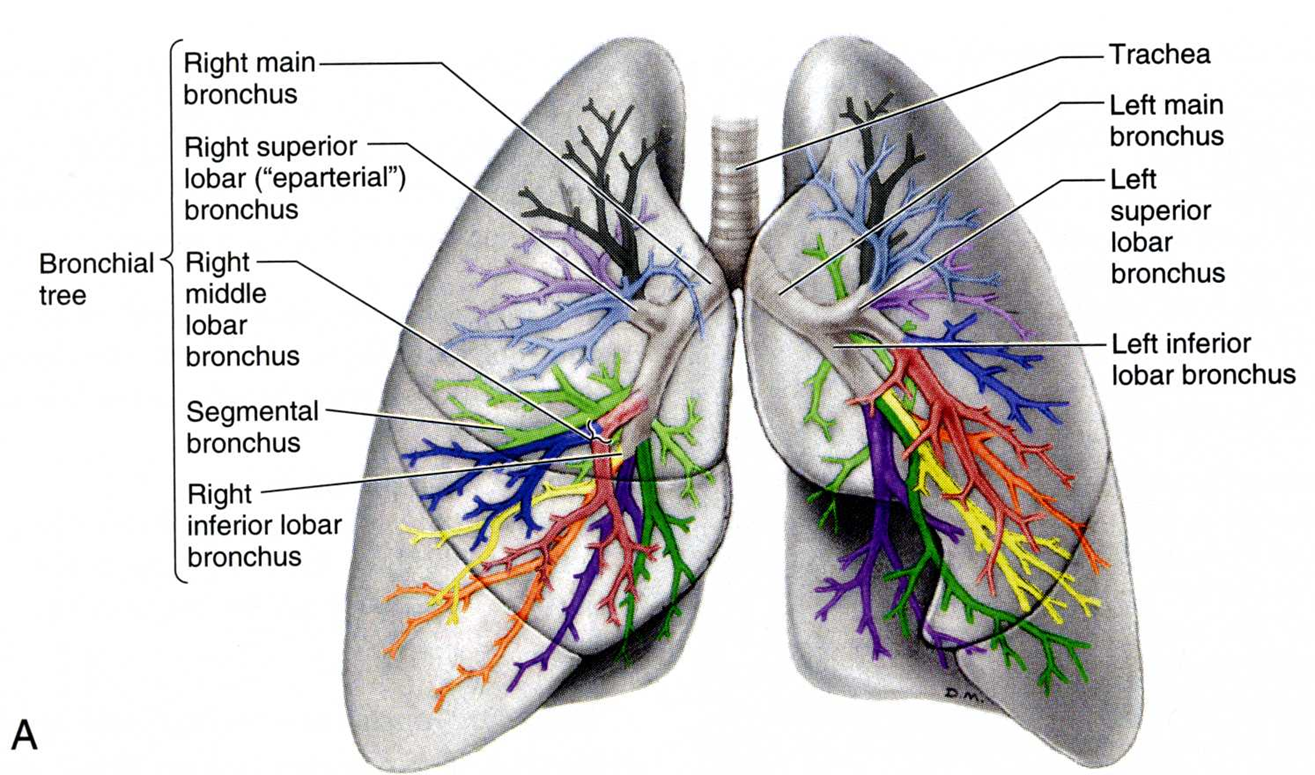
tracehobronchial tree
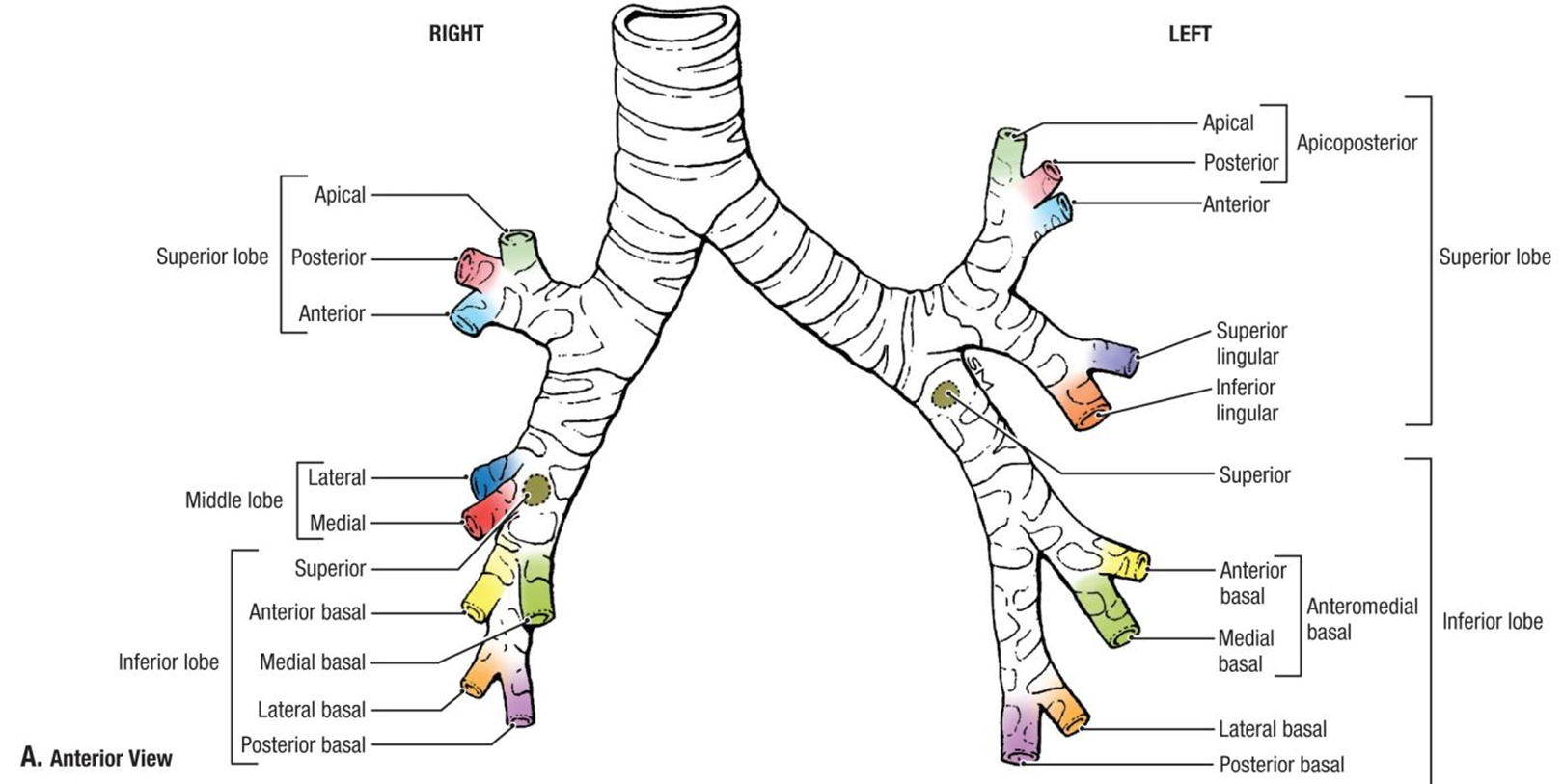
Each main bronchus divides into lobar (secondary) bronchi. Each lobar bronchus divides into segmental (tertiary) bronchi. 10 segments on the right, & 8-10 on the left.
bronchopulmonary segments
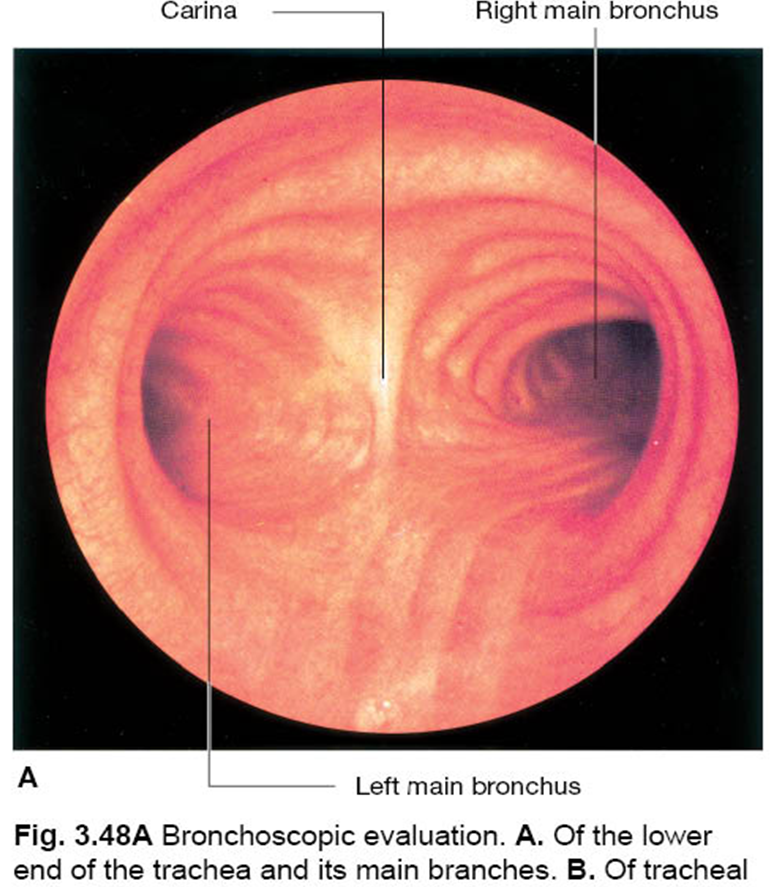
clinical note: bronchoscopy & aspirated foreign body
An aspirated foreign body is more likely to enter the right main bronchus bc it is more vertical, wider, and shorter than the left main bronchus.
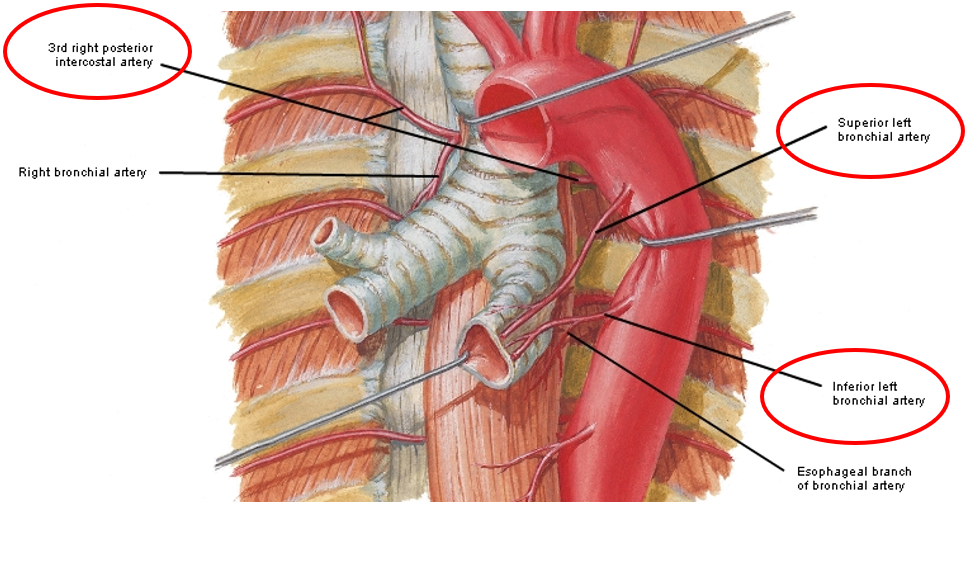
bronchial arteries
Bronchial arteries supply the bronchi, bronchioles, & visceral pleura w oxygenated blood.
pulmonary are busy w gas exchange, so bronchial arteries supply oxygenated blood to pulmonary tissues
Typically, there are 2 arising from the aorta going to the left lung, & 1 arising from the 3d right intercostal artery to the right lung. Tertiary branches inter the lung segments.
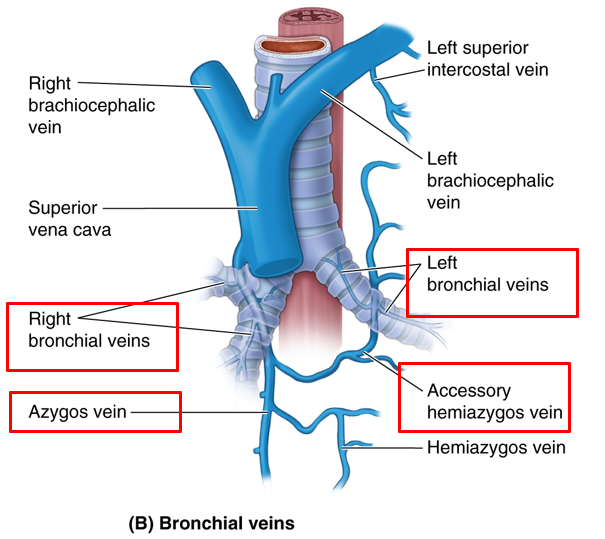
bronchial veins
Bronchial veins drain only a portion of the blood supplied by the bronchial arteries (proximal part near the root of lung).
The remainder is drained by the pulmonary veins.
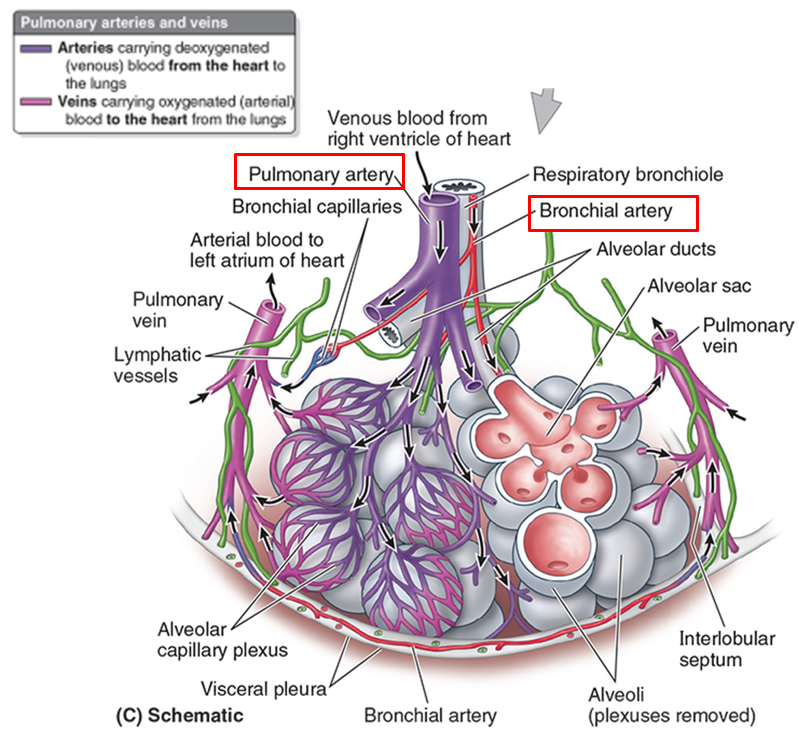
big picture: bronchial vs pulmonary vessels
Pulmonary arteries and veins are large - gas exchange – cardiopulmonary circulation.
Bronchial arteries and veins are small - supply & drain the tissues of the bronchial tree.
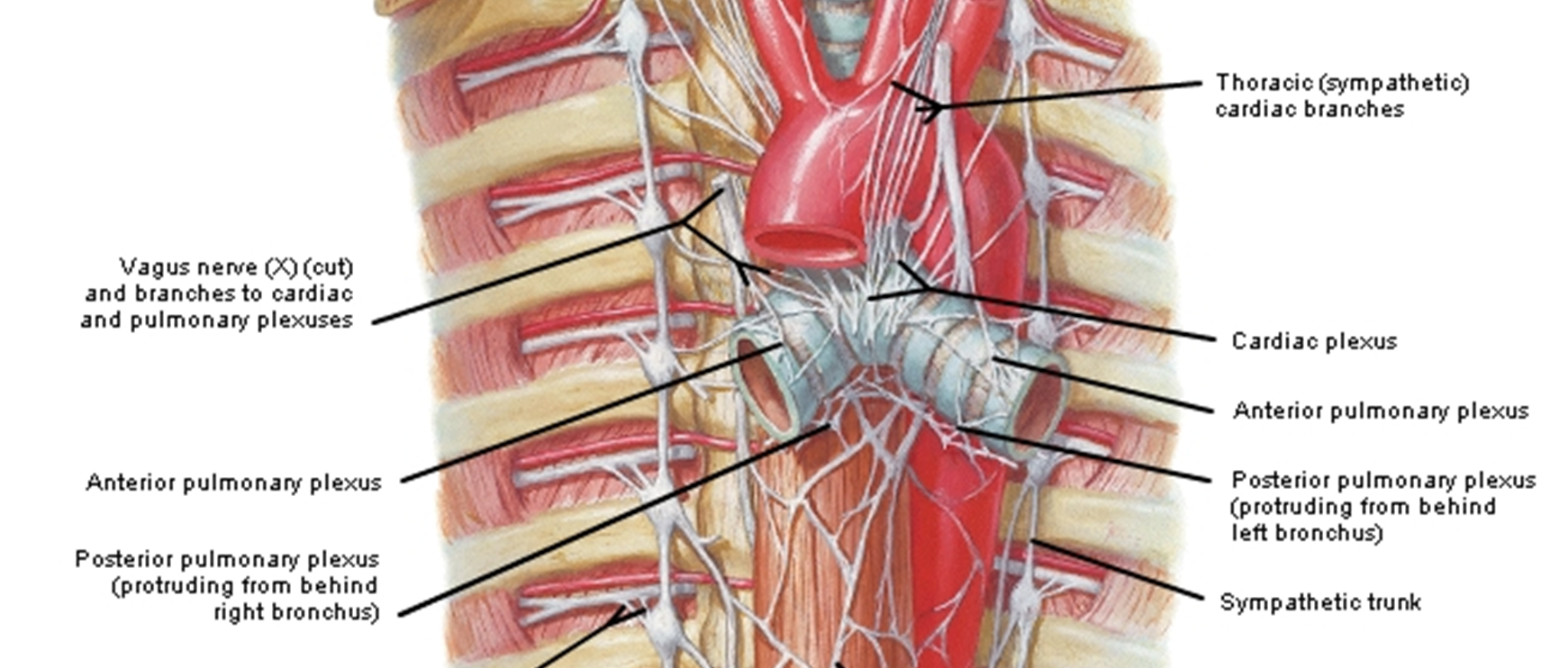
nerves of lungs
Nerves to the lungs arise from the pulmonary plexuses.
Parasympathetic (rest & digest) presynaptic fibers in the plexus are from the Vagus nerves.
They constrict bronchiolar smooth muscle, stimulate glandular secretion, and are inhibitory to blood vessels.
Visceral afferent fibers to Vagus nerve from lungs for stretch, respiration reflexes, & cough reflex.
Sympathetic (fight or flight) fibers in the plexus are postganglionic from upper 5 thoracic ganglia. They vasoconstrict, inhibit glands, relax bronchial smooth muscle.
Nociceptive (pain) afferents from bronchi travel with the sympathetic fibers.
diaphragm
It is the most important respiratory muscle.
It has a right and left dome. The muscular fibers converge to a central tendon.
When the diaphragm contracts, the height of the domes decreases, and the volume of the thorax increases.
Innervated by phrenic nerve (C3-C5)
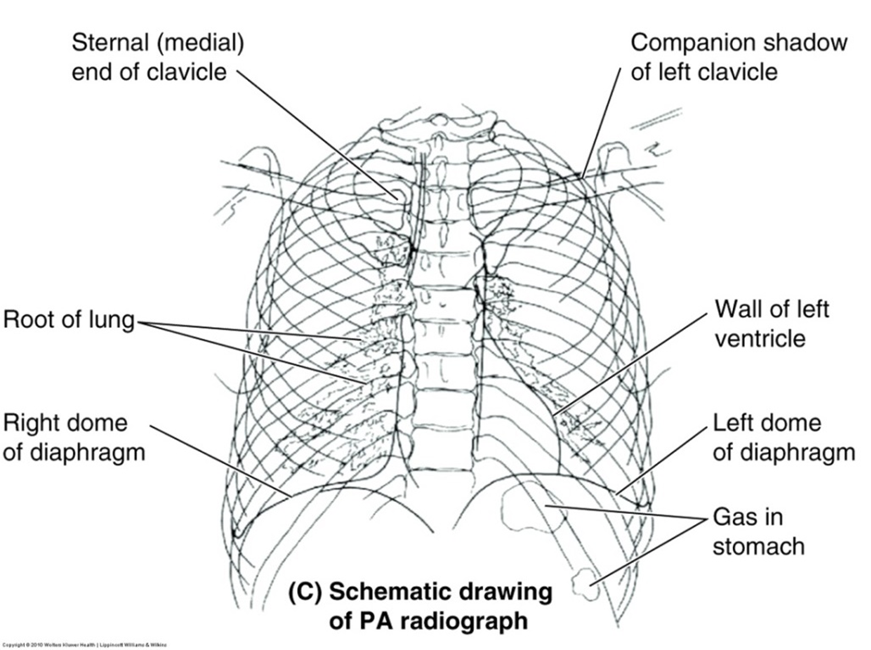
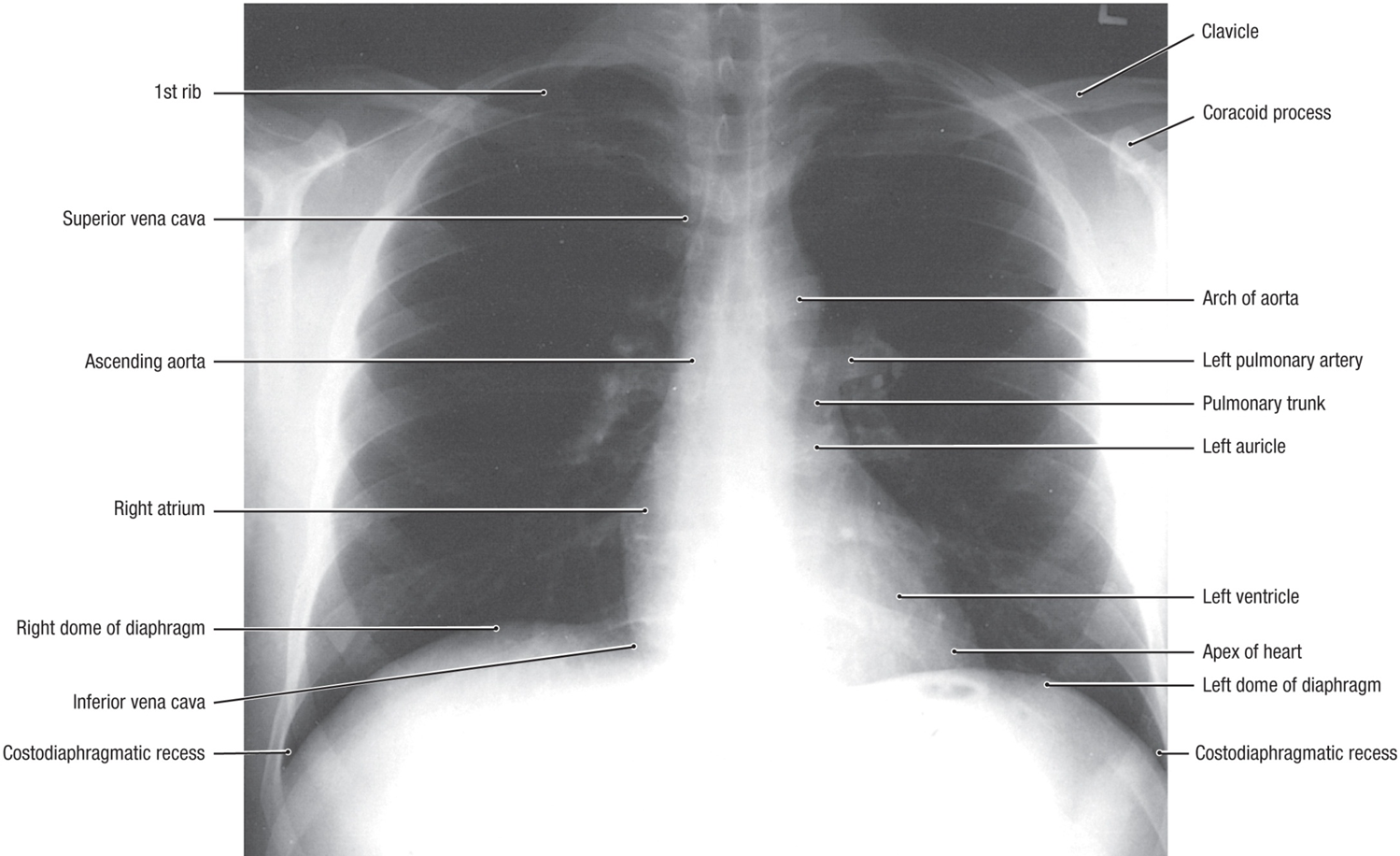
chest x-ray