Haemorrhagic fevers
WHAT IS A VIRAL HAEMORRHAGIC FEVER?
Viral haemorrhagic fevers (VHFs) refer to a group of illnesses that are caused by several distinct families of viruses. Symptoms are similar.
In general, the term "viral haemorrhagic fever" is used to describe a severe multisystem syndrome (multiple organ systems in the body are affected, sometimes all).
Characteristically, the overall vascular system is damaged, so that the body's ability to regulate itself is impaired. These symptoms are often accompanied by haemorrhage (bleeding), although the bleeding is itself rarely life-threatening.
VIRUS FAMILIES THAT CAUSE VHF
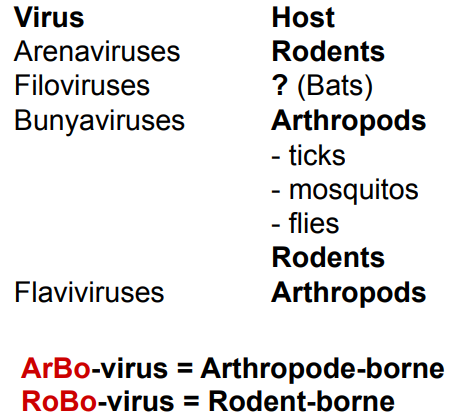
These are four main families, Arenaviruses, Filoviruses, Bunyaviruses and Flaviviruses. These viruses are enveloped (fatty lipid) ssRNA viruses. Animals or insect hosts are their natural reservoirs, but never humans (seen in the high mortality rate). They are geographically restricted (cannot be seen in most places, due to climate, reservoirs, etc). In rare cases, other viral and bacterial infections can cause haemorrhagic fever; e.g. scrub typhus.
VHF ARE ZOONOTIC DISEASES
Totally dependent on their natural hosts for replication and overall survival. Humans are often dead-end hosts. Human-to-human transmission exists for some VHF, such as Ebola, Marburg, Lassa and CCHFV. Rodents and arthropods are the main reservoirs and vectors. The reservoir(s) for Ebola and Marburg still unknown, but probably bats.
Lassa and CCHFV is different among different patients. They are not usually very infectious, but on occasions one person can infect a whole hospital.
ZOONOSES
ARENAVIRUSES
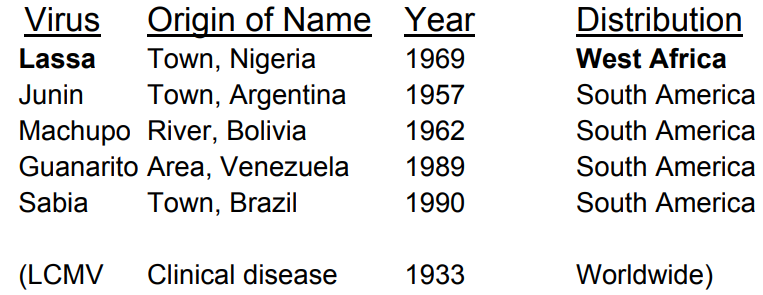
LCMV causes very mild symptoms in humans. It has been studied easily due to low severity, in order to understand Arenaviruses.
LASSA VIRUS
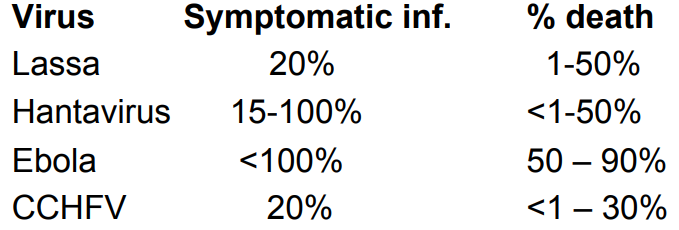
It's endemic in areas of West Africa, including Nigeria, Liberia, Sierra Leone, and Guinea. There are up to 500000 infections/year, with 5-50000 deaths. The transmission is rodent-to-human (the “multimammate rat”, Mastomys species-complex). There is also secondary human-to-human transmission with the potential for nosocomial outbreaks with high case-fatality.
FILOVIRUS

EBOLA
Until the present outbreak in West-Africa, there had been approximately 2300 cases (1500 deaths) in total since its identification in 1976. All outbreaks occur in tropical African ecosystems (between latitude 5˚ North and 5˚ South). In West Africa 2014-2015 there were close to 30.000 cases and >11.000 deaths.
There are six types of Ebola virus:
Zaire (EBOV)
Sudan (SUDV)
Tai Forest (TAFV)
Bundibugyo (BDBV)
Reston (RESTV)
Bombali (BOMV – from bat)
All except Reston and Bombali viruses have been shown to cause disease in humans. Reston virus causes disease in non-human primates, but not in humans.
MARBURG
There are two types of Marburg virus:
Marburg (MARV)
Ravn (RAVV)
Both have been shown to cause fatal disease in humans.
BUNYAVIRUSES
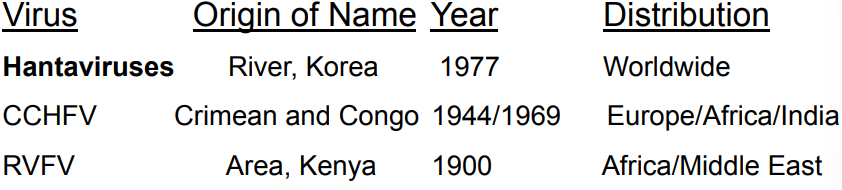
CCHFV: Crimean-Congo HFV.
RVFV: Rift Valley fever virus.
FLAVIVIRUS (DENGUE)
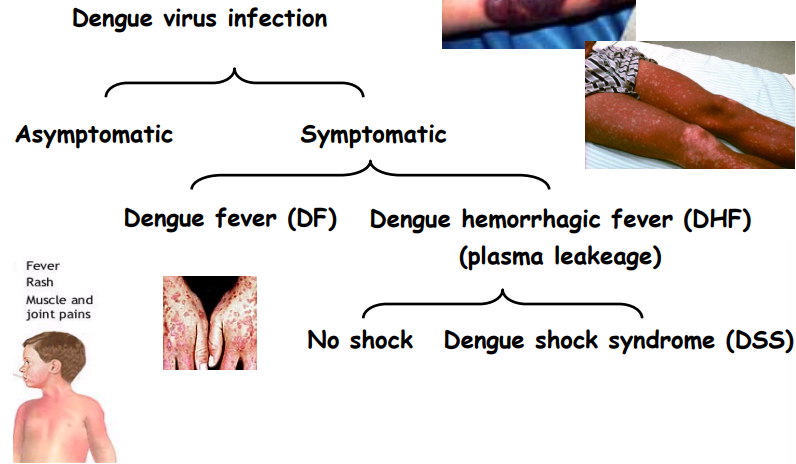
There more than 2.5 billion humans in risk areas. There are a lot of infections that are completely asymptomatic. DF lasts for 7-10 days, where you feel bad but you recover. DSS is mainly in young children, who die.
SYMPTOMS OF VHF
They vary by the type of VHF, but early signs often include: fever, fatigue, dizziness, muscle aches, loss of strength and exhaustion (”Influenza-like symptoms”).
Patients with severe cases of VHF can show signs of bleeding under the skin, in internal organs, or from mouth, eyes, or ears. However, patients rarely die because of blood loss. Severely ill patient cases may also show shock, nervous system malfunction, coma, delirium, and seizures. Some types of VHF are associated with renal (kidney) failure.
Not all infected individuals get sick.
TREATMENT OF VHF
Patients receive supportive therapy, but generally speaking, there is no other treatment or established cure for VHFs. Ribavirin, an anti-viral drug, has been effective in treating some individuals with Lassa fever or HFRS. Treatment with convalescent-phase plasma has been used with success in some patients with Argentine haemorrhagic fever.
VACCINES FOR VHF
With the exception of yellow fever and Argentine haemorrhagic fever, for which vaccines have been developed, no vaccines exist that can protect against these diseases.
WHAT CAUSES DISEASE DURING VHF?
Is it the virus alone?
Is the virus per se not involved at all?
Is the disease caused by our immune defence against the virus?
Do the virus interfere with the activation and function of the immune responses, thereby causing disease?
A mixture?
Not all infected individuals become ill though. Ebola is the most deadly of them all.
EBOLA (TRANSMISSION)
You can get it through contact with blood, secretions or tissues from patients or infected animals (gorillas and chimpanzees). Also through injections with contaminated syringes (high mortality), mucosal exposure (eyes), at least in animal models, and airborne (extremely rare).
Receptors for the virus are C-type lectins (several types) and others. Almost all organs are infected, so it's expected that the virus can enter all organs.
EBOLA (CLINICAL PRESENTATION)
The incubation period is 4-10 days.
You can get high fever, muscle pain, gastrointestinal symptoms, swelling of the lymph nodes, kidneys and brain. Necrosis can occur in different organs (liver, lymph organs, kidney, testis/ovaries). The patient will also have impaired coagulation, haemorrhage, and 50% develop rash, but profuse bleeding is rare.
Severe nausea, prostration, increased respiration rate, anuria, and drop in body temp. indicates oncoming shock = death.
<50% show signs of bleeding.
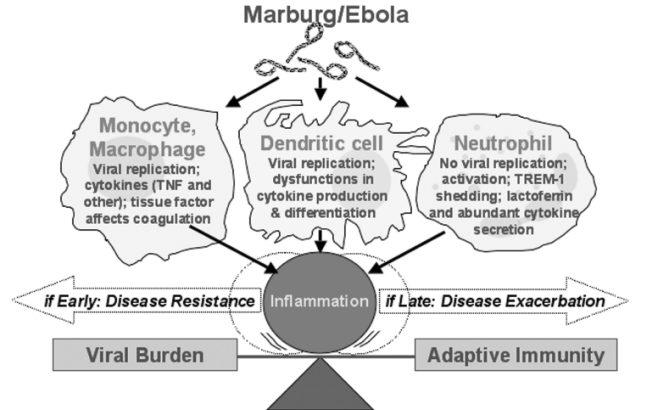
EBOLA (PATHOGENESIS)
Vascular dysfunction (due to immune system generally) and loss of endothelial barrier function are considered the major contributors to the fatal outcome of Ebola virus infection, like for other VHF.
However, this is not caused by the virus infection per se. It is believed that the vascular dysfunction is caused by activation of the immune system in the endothelia.
TNF and NO elevated in fatal cases, might be involved.
Viral glycoprotein secretion which interferes with the immune system.
EBOLA (FATAL VS NON-FATAL CASES)
Up to 100x more virus in blood in fatal cases.
Very high levels of virus very early p.i. in fatal cases.
Specific IgM-responses 2 days p.i. and IgG at days 5-8 p.i. in survivors.
No specific IgG-responses in fatal cases.
High levels of serum-NO in fatal cases.
Decrease in T-cell numbers in fatal cases.
Early inflammatory responses in survivors.
EBOLA (CONCLUSION)
Normal cross-talk between innate and adaptive immunity is subverted by Ebola, resulting in delayed adaptive immunity, uninhibited viral replication and disease, due to high level of cytokine-production.
HANTAVIRUS
Human infection
HFRS (fever with renal syndrome) or HCPS (cardiopulmonary syndrome)
Transient
Rodent infection
Asymptomatic
Chronic
Close to a small river called Hantaan in Korea, 3000 United Nations soldiers experienced an acute febrile illness with acute renal failure and shock during the Korean War. Mortality was around 7%. HFRS was discovered by ”western medicine”.
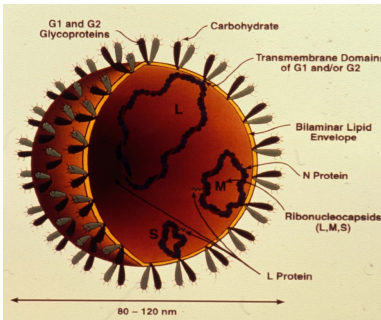
It's an enveloped tripartite (-)ssRNA virus that encodes four proteins:
Nucleocapsid protein (N)
Envelope protein G1 and G2
L-protein (RNA-dependent RNA polymerase)
It has complementary 3' and 5' terminal sequences (panhandle structures) that form circular viral RNA.
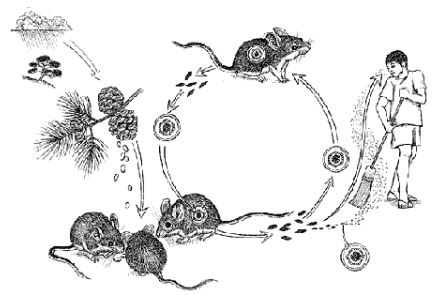
ANIMAL FACILITIES AND HANTAVIRUS
This is not a good idea. Hantavirus is the microbe that has accidentally killed most laboratory workers in animal labs globally. Infection of rats (natural reservoir) is asymptomatic and life-long. One infected rat can quickly contaminate a whole animal lab. Today, all animals are screened for hantaviruses.
HAEMORRHAGIC FEVER WITH RENAL SYNDROME (HFRS)
It has been known in China for more than 1000 years but was first described in Sweden 1934. In Euro-Asia there are around 200000 cases annually. Mortality differs from <0.1% to 10% depending on the virus. Clinical severity ranges from asymptomatic infection to fulminant haemorrhagic shock.
There are often five different phases of the disease:
Febrile
Hypotensive
Oliguric
Polyureic
Convalescent
However, there is considerable variation between patients.
HANTAVIRUS CARDIO-PULMONARY SYNDROME (HCPS)
The first case was in 1993, Four-Corner region, USA. In the Americas there are less than 1000 recognized cases annually. Mortality is around 50%. The symptoms are cardiac and respiratory, with normally less renal and bleeding manifestations compared to HFRS.
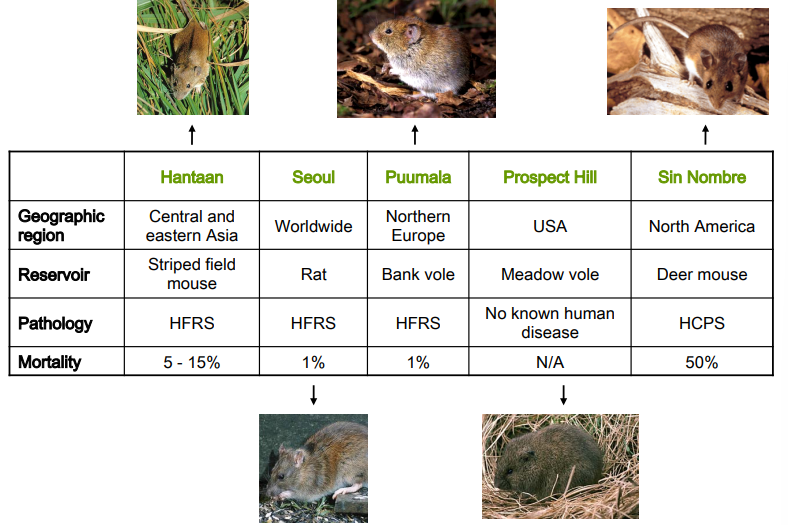
CHARACTERISTICS OF SOME HANTAVIRUSES
There are over 25 different viruses. Not all infect humans and not all cause disease.
PUUMALA HANTAVIRUS
It causes a form of HFRS (Nephropathia epidemica). There are epidemics in Northern Europe. The largest outbreak ever in Sweden was in 2007/08, with a total of 2153 diagnosed cases.