Urinary Tract Infections (UTIs)
Urinary Tract Infections
Definition and Prevalence
Urinary Tract Infection (UTI): Presence of microorganisms in the urine not accounted for by contamination.
Prevalence varies by age and gender.
Symptomatic UTI: Occurs in 30% of women between 20-40 years old.
Up to 50% of females will have a UTI at some point in their lifetime.
Types of UTIs Based on Location
Upper UTI
Types of Infections:
Pyelonephritis
Intrarenal abscess
Presentation:
CVA tenderness
Flank pain
Fever
Nausea/Vomiting (N/V)
Malaise
Lower UTI
Types of Infections:
Cystitis
Urethritis
Prostatitis
Epididymitis
Presentation:
Dysuria (painful urination)
Urgency
Frequency
Nocturia (frequent urination at night)
Suprapubic heaviness
Gross hematuria (visible blood in urine)
Uncomplicated vs. Complicated UTIs
Uncomplicated (Simple) UTI
Involves only one type of bacteria.
85% are caused by E. coli.
Limited to the lower urinary tract.
Complicated UTI
Structural or functional abnormality interferes with urine flow or host defenses.
Factors include:
Congenital abnormalities
Obstruction
Indwelling catheters
Neurologic deficits affecting urinary function
UTIs in males
Require longer treatment regimens.
Often polymicrobial (involving multiple bacteria).
Patients are more prone to additional UTIs.
Laboratory Tests and Routes of Infection
Laboratory Tests
Urine Analysis (U/A) Possible Findings:
Pyuria (pus in urine)
Nitrite
Leukocyte Esterase
Blood
Routes of Infection
Ascending:
Bacteria from the urethra travel up to the bladder, causing cystitis.
More common in females (shorter urethra).
Most common route of infection for UTIs.
Other Routes:
Hematogenous:
Seeding of the urinary tract with pathogens from the bloodstream.
Lymphatic
Host Defense Mechanisms and Risk Factors
Host Defense Mechanisms
Urine characteristics: low pH, high osmolality, and urea.
Prostatic secretions: can inhibit bacterial growth.
Increased urge to urinate when bacteria enter the bladder.
Risk Factors
Female
Sexual Intercourse, lack of voiding after sexual intercourse
Use of diaphragm and/or spermicide
Diabetes Mellitus
Pregnancy
Male
Uncircumcised
Prostatic hyperplasia
Both Sexes
Urologic instrumentation
Neurogenic bladder
Urinary tract obstruction
Incomplete voiding
UTI Treatment
Treatment Goals
Eradicate causative organism.
Prevent complications and recurrence of infection.
Treatment Considerations
Patient compliance.
Drug properties: Adequate concentration in urine.
Treatment Duration
Uncomplicated: 1-7 days (3 days is optimal).
Complicated: 2-4 weeks (up to 6 weeks if prostatic involvement).
Empiric vs. Directed Treatment
Uncomplicated UTIs: treated empirically (without Culture & Sensitivity (C&S)).
Complicated UTIs: Gram stain, Culture & Sensitivity (C&S) with empiric treatment until results return.
Treatment of Uncomplicated UTI
Acute Uncomplicated Cystitis
Frequent presentation in the outpatient setting.
Especially common in women of childbearing age.
Causative Organisms
E. coli > 85% of uncomplicated lower UTIs.
Other causes:
Staph Saprophyticus
Klebsiella Pneumoniae
Proteus Mirabilis
Enterococcus spp.
Empiric treatment with coverage for the most common organisms.
Follow up for resolution of signs/symptoms.
Treatment Duration
Single-dose treatment – not recommended.
3-7 days.
3 days is optimal with good cure rate & avoidance of Adverse Effects (AE’s).
Antimicrobials for Uncomplicated UTIs
Nitrofurantoin (Macrobid®)
MOA: Inhibits various enzymes in bacteria and damages DNA
AE: hemolytic anemia (G6PD deficiency), GI, acute pneumonitis, neurological problems
Contraindications: anuria, oliguria, pregnancy ≥ 38 wks
Dosing: 100mg PO BID x 5 days.
Do not use in patients with Creatinine Clearance (CrCl) < 60ml/min.
Trimethoprim/Sulfamethoxazole (TMP/SMX) (Bactrim DS, Septra DS®)
Dosing:
2 Double Strength (DS) tablets as a single dose.
1 DS tablet BID x 3-7 days.
AVOID in sulfa allergic patients.
In some areas, there is up to a 20% resistance rate.
Fluoroquinolones
Ciprofloxacin (Cipro®) 250 mg BID x 3-7 days.
Levofloxacin (Levaquin®) 250 mg Qday x 3-7 days.
Fosfomycin (Monurol®)
3gm PO x 1
Mechanism of Action (MoA): inactivates pyruvyl transferase which then inhibits bacterial wall synthesis = bactericidal.
Adverse Effects (AEs): anorexia, diarrhea, epigastric discomfort, Headache (HA), Nausea (N), Vomiting (V), rash.
Beta-Lactams
MoA: Interfere with bacterial cell wall synthesis/repair. Bind penicillin binding proteins (PBP)
weakens cell membrane → cell lysis → bactericidal. Exhibit time dependent killing
AE: GI Upset, Hypersensitivity reactions, Nephritis, Neurotoxicity
Amoxicillin: 3 grams x 1 dose or 500 mg BID x 3 days.
Amoxicillin/Clavulanate (Augmentin®): 500 mg Q8h x 3 days.
Cephalosporins: good efficacy but no advantages in simple UTI over Augmentin®.
Big push to avoid fluoroquinolones for uncomplicated UTIs due to increasing resistance in Staph, Pseudomonas, and other strains of bacteria.
Antimicrobials for Complicated UTIs
Trimethoprim/Sulfamethoxazole (TMP/SMX) (Bactrim, Septra DS®)
Dosing: 1 DS tablet BID x 7-14 days.
Fluoroquinolones
Ciprofloxacin (Cipro®) 250-500 mg BID x 7-14 days.
Levofloxacin (Levaquin®) 250 mg Qday x 7-14 days.
Amoxicillin/Clavulanate
Dosing: 500 mg Q8h x 7-14 days.
Recurrent Lower UTIs
Nitrofurantoin
Dosing: 50 mg Qday x 6 months.
TMP/SMX
Dosing: ½-1 single strength tablet Qday x 6 months.
Acute Pyelonephritis
Signs/Symptoms
Fever/chills, malaise, flank pain, CVA tenderness, N/V, decreased appetite.
Treatment
Many of the same antimicrobials used for uncomplicated UTIs.
Gram stain.
Gram Stain: gram (+) cocci: S. fecalis (Ampicillin indicated).
Empiric therapy until Culture and Sensitivity (C&S) results.
Fluoroquinolones or Aminoglycoside +/- Beta-lactam.
Longer Duration of Treatment: Usually 14 days.
Inpatient vs. Outpatient Treatment
Inpatient: IV Antimicrobial & IV Fluids.
High fever, N/V & high risk of dehydration, immunocompromised.
Antimicrobials for Acute Pyelonephritis - Outpatient
First-Line Therapy
Fluoroquinolones
Ciprofloxacin (Cipro®) 500 mg BID x 7 days.
Levofloxacin (Levaquin®) 750mg Q day x 5 days.
Ceftriaxone IV, gentamicin IV - if Fluoroquinolone (FQ) resistance >10%.
Second-Line Therapy
TMP/SMX (Bactrim, Septra DS®)
Dosing: 1 DS tablet BID x 14 days.
Ceftriaxone 1gm IV.
Gentamicin 7mg/kg IV.
Amoxicillin/Clavulanate
Dosing: 500 mg Q8h x 14 days.
UTIs in Special Populations: Pregnancy
Pregnancy: UTIs are more common.
Associated with adverse fetal effects.
Asymptomatic bacteriuria may progress to pyelonephritis.
Treat to avoid complications.
Regular screening for bacteriuria during pregnancy.
Treatment Options in Pregnancy
First-Line Treatment (Tx): Beta-Lactams
Amoxicillin or Amoxicillin/Clavulanate (Augmentin®) - if increased resistance to Amoxicillin.
Cephalosporins - Cephalexin (Keflex).
Sulfonamides: AVOID in 3rd trimester (newborn hyperbilirubinemia).
AVOID Tetracyclines & Fluoroquinolones IN PREGNANCY.
Follow up urine culture: 1-2 weeks after completion of therapy.
UTIs in Special Populations: Catheterized Patients & Males
Catheterized Patients
UTIs are very common in catheterized patients.
Bacteria may be introduced into the bladder with insertion of the urinary catheter, or bacteria may ascend to the bladder.
Asymptomatic: remove catheter & hold antimicrobials.
Symptomatic: remove catheter & antimicrobials.
If discontinuation of the catheter is not possible, change the catheter (especially if > 2 weeks).
UTIs in Male Patients
Abnormality (structural or functional) should be expected.
Treat as complicated UTI.
Treatment duration: 7-14 days (longer if prostate involvement).
Recurrent UTIs
Two groups based on number per year:
< 3 UTIs per year: treat each infection with short-course therapy.
3 UTIs per year: consider long-term prophylactic therapy (6 months) with periodic urine cultures.
Symptomatic re-infections with sexual activity:
Single-dose prophylactic therapy: 1 Single Strength (SS) Sulfamethoxazole/Trimethoprim tablet or Nitrofurantoin (Macrobid®) after intercourse.
Voiding after intercourse may also help prevent UTIs.
Relapse after short-course therapy:
14-day treatment.
Prostatitis
Inflammation/infection of the prostate.
Acute or chronic infection.
Acute: sudden onset of urinary & constitutional signs/symptoms.
Diagnosis: Prostatic secretions & urine (bacteria & leukocytes).
Organisms: Most common: Gram (-) enteric organisms.
Predominant organism: E. coli.
Treatment:
Antimicrobials:
TMP/SMX (Bactrim®)
Fluoroquinolones: Ciprofloxacin, Levofloxacin
Duration:
Acute: 4 weeks
Chronic: 6-12 weeks
Epididymitis
Bacterial (most common cause): Likely organism depends on the patient’s age.
Prepubertal: Coliform bacteria (E. coli) - Treatment: Sulfamethoxazole/Trimethoprim (Bactrim®).
Young adult to middle age: C. trachomatis, N. gonorrhoeae - Treatment: Ceftriaxone (Rocephin®) 500 mg IM x 1 dose & Doxycycline 100mg PO BID x 10 days (or Ceftriaxone 500mg IM x 1 plus Levofloxacin 500mg Qday x 10 days in MSM).
Older males: Coliform bacteria (E. coli) - Treatment: Sulfamethoxazole/Trimethoprim (Bactrim®) or Levofloxacin.
Other causes:
Post-infectious (inflammatory reaction) - After systemic infection.
Chemical epididymitis - reflux of urine causes an inflammatory response.
Urethritis
C. trachomatis, N. gonorrhoeae
Treatment: Ceftriaxone & Azithromycin (or Doxycycline).
Urinary Analgesic
Phenazopyridine
Rx: Pyridium® 100 mg & 200 mg tablets.
Dosage: 200 mg PO TID with food.
OTC: 95 mg (AZO-Gesic, AZO-Standard, & Uristat); 97.2 mg (UTI Relief).
Mechanism of Action (MoA): acts directly on urinary tract mucosa to produce local analgesic effect.
Use:
Symptomatic relief of pain, burning, urgency, frequency arising from irritation of the lower urinary tract (from instrumentation, irritation, or infection).
Useful with initiation of antimicrobial (symptomatic relief until antimicrobial controls infection).
Adverse Effects:
Red-Orange discoloration of urine.
Abdominal cramping, Headache (HA).
Rare - hepatitis, acute renal failure, hemolytic anemia.
Other Treatments for UTI
Estrogen cream
Postmenopausal women.
Cranberry
Doesn’t help treat active UTI.
Might help prevent recurrent infections.
Prevents bacterial adhesion to the urethral wall.
UTI Summary
Diagnosis | Pathogens | Treatment | Other Info. | |
|---|---|---|---|---|
Acute Cystitis (U) | •E. Coli •S. Saprophyticus | •TMP/SMX DS •FQ •1-7 days (3 days is preferred) | ||
Pregnancy | •E. Coli •S. Saprophyticus | •Amox/Clav (Augmentin®) •Cephalosporin •TMP/SMX DS* •7 days | *Avoid sulfamethoxazole during 3rd trimester | |
Acute Pyelonephritis (U) | •E. coli | •TMP/SMX DS •FQ •14 days | ||
Acute Pyelonephritis (C) | •E. coli •P. mirabilis •K. pneumoniae •P. aeruginosa •E. fecalis | •FQ •Extended spec. PCN + AG •Severity of illness will determine duration of IV Antibx, PO to complete 14 days of therapy | ||
Prostatitis | •E. coli •K. pneumoniae •Proteus spp. •P. aeruginosa | •TMP/SMX DS •FQ •4- 6 weeks |
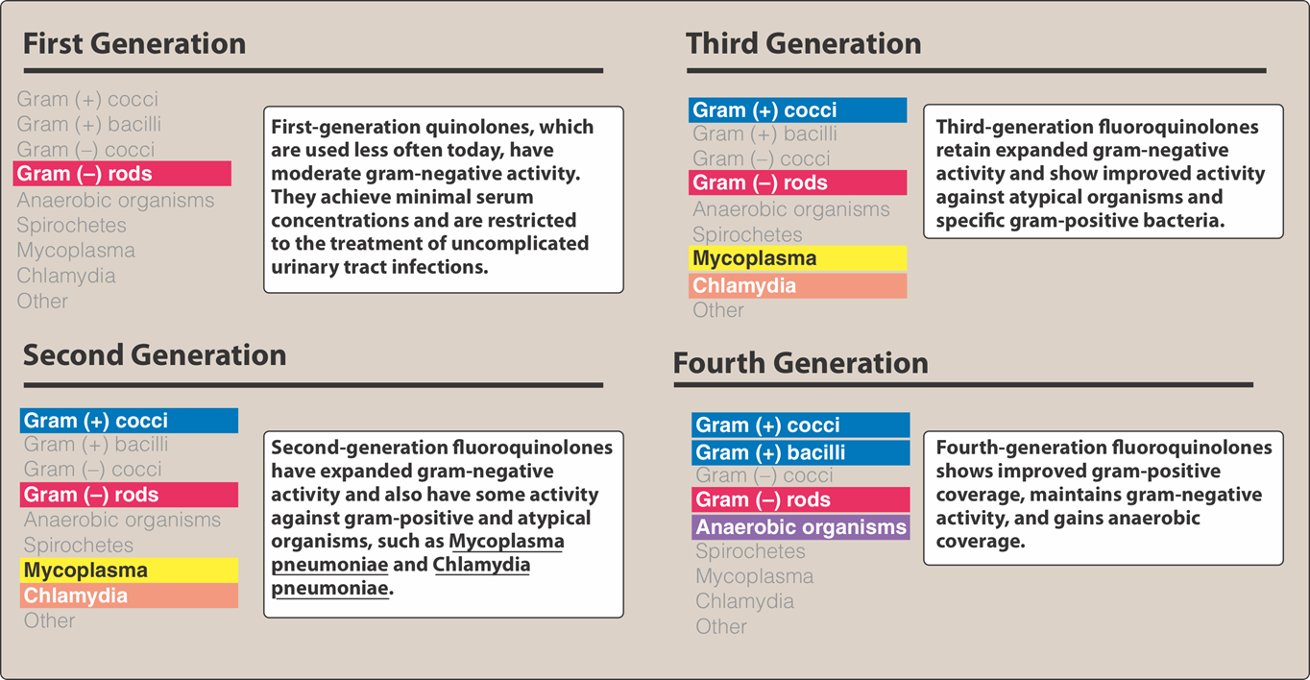
Fluoroquinolones: Interactions and Adverse Effects
Interactions
Ingestion with antacids (Aluminum (Al) or Magnesium (Mg)).
Dietary supplements with iron or zinc, Calcium (Ca) (supplements or food).
Adverse Effects
Gastrointestinal (GI): Nausea/Vomiting/Diarrhea (N/V/D).
Hypoglycemia.
Phototoxicity.
Connective tissue problems:
Avoid in pregnancy & lactation and in pediatrics (under 18 years of age) due to cartilage erosion.
Tendon rupture.
Black Box warning:
Patients >60 years old, concomitant corticosteroid therapy, & patients with kidney, heart, or lung transplant.
Central Nervous System (CNS) effects:
Convulsions, increased Intracranial Pressure (ICP), and toxic psychosis.
SMZ/TMP
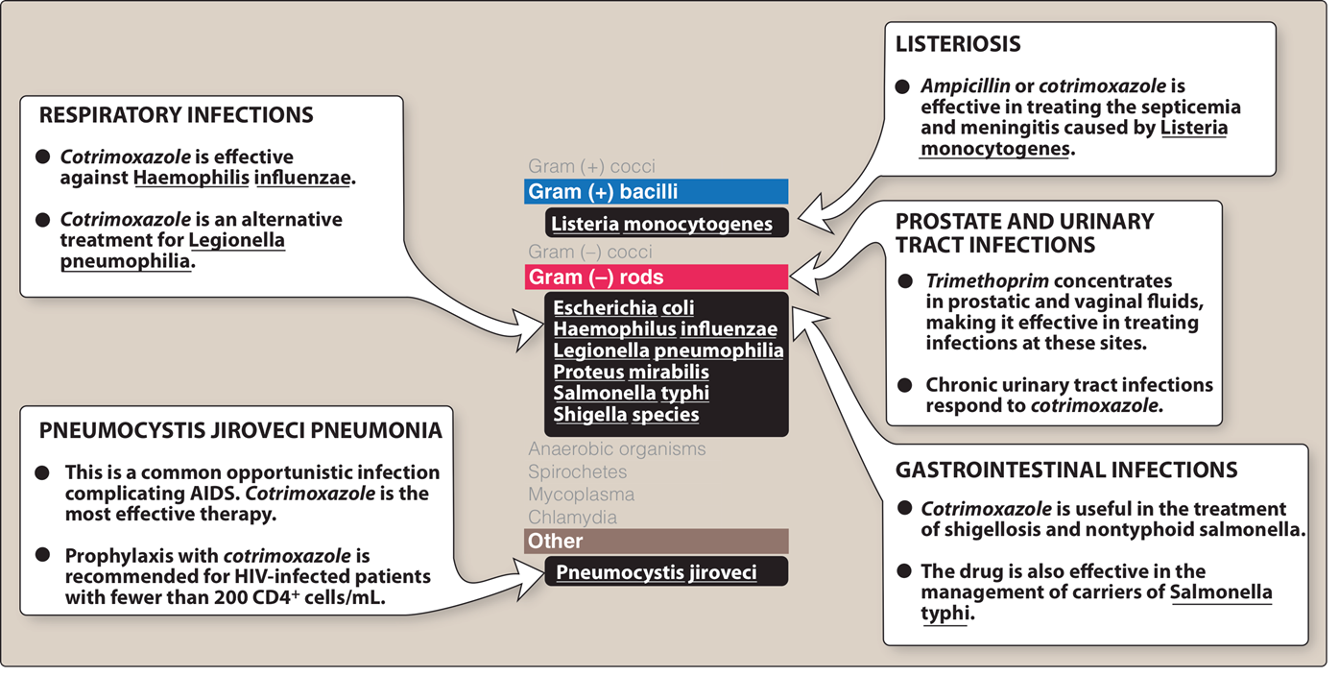
Sulfonamides
Mechanism of Action (MoA)
Inhibition of the synthesis of bacterial dihydrofolate acid (essential cofactor).
Antimicrobial Spectrum
Bacteriostatic.
Enterobacteria in the urinary tract.
Kinetics
Liver metabolism, urinary excretion.
Drugs
Sulfamethoxazole/Trimethoprim (Bactrim DS, Septra DS).
Adverse Effects
Crystalluria.
Hypersensitivity:
Rashes, angioedema, Stevens-Johnson Syndrome (SJS).
Hemopoietic disturbances.
Kernicterus:
Avoid in newborns & infants less than 2 months of age (displace bilirubin from binding sites on albumin → bilirubin in the Central Nervous System (CNS)).
Avoid in pregnant patients near term.
Nitrofurantoin (Macrobid®)
Mechanism of Action (MoA):
Inhibits various enzymes in bacteria and damages DNA.
Adverse Effects (AE):
Discoloration of urine, hemolytic anemia (Glucose-6-Phosphate Dehydrogenase (G6PD) deficiency), Gastrointestinal (GI) upset, acute pneumonitis, neurological problems.
Contraindications:
Anuria, oliguria, pregnancy ≥ 38 weeks.
Gentamycin
MoA: diffuse through porin channels (oxygen dependent transport system) → bind to the 30 S ribosomal subunit → interrupting protein synthesis
AE: nephrotoxicity, ototoxicity, and allergic reactions such as rash or anaphylaxis.
Azithromycin
MoA: Irreversibly bind to the 50S bacterial ribosomal subunit→ inhibiting translocation step of protein synthesis
AE: N/V/D, Cholostatic juandice