Menstrual Cycle
Control of the Menstrual Cycle
The menstrual cycle is primarily controlled by the hypothalamus-pituitary axis in the brain.
Various hormonal secretions influence the cycle:
Gonadotrophic hormones: Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH) produced by the anterior pituitary gland
Related to hypothalamus-pituitary axis in the brain
Ovarian hormones: Estrogen, Progesterone, and Inhibin
Related to ovarian follicles within the ovary
4 Phases of the Menstrual Cycle
Folliculo recruitment and development
Ovulation
Formation of the corpus luteum
Regression of the corpus luteum:
If fertilization does not occur, the corpus luteum transforms into corpus albicans
Corpus Luteum
The corpus luteum is a yellowish endocrine structure in the ovary formed from the merging of follicular thecal cells and granulosa cells → these transform into luteal cells after oocyte discharge
Process known as luteinization
It regresses into corpus albicans if no fertilization occurs, and stops producing estrogen and progesterone
decrease in estrogen and progesterone levels allows the hypothalamus to resume its production of gonadotropin-releasing hormone (GnRH) → causing the release of LH and FSH by the anterior pituitary gland
Organs Involved in the Menstrual Cycle
Two primary organs are involved in the menstrual cycle:
Ovary
Ovarian cycle - 2 phases
Follicular phase
Luteal phase
Uterus
Endometrial cycle - 3 phases
Menstrual phase (menses)
Proliferative phase
Secretory phase
Follicular Phase
First half of the menstrual cycle (average 14 days of a 28-day cycle):
Marked by a decline in 3 hormone levels post-ovulation, (no fertilization occurs)
Progesterone (by granulosa cells)
Estrogen & Inhibin (by corpus luteum)
Ovarian cycle begins at the start of the follicular phase - if fertilization has not occurred from previous cycle -
Regression of corpus luteum
Decrease in estrogen and progesterone production
Removal of inhibition for the production of GnRH by the decrease in estrogen and progesterone levels
Resuming FSH production and increasing FSH levels in the late luteal phase
FSH is essential for the recruitment and development of ovarian follicles
Granulosa and Theca Cells
Granulosa folliculi → under influence of FSH
Theca folliculi → under the influence of LH
Granulosa and theca folliculi of the recruited follicles begin steroid hormone production:
Granulosa cells increase estrogen production
Androgens synthesized by theca cells diffuse into granulosa cells and are converted to estrogen by aromatase
LH stimulates the theca cells to synthesize and secrete progesterone and testosterone
Feedback Mechanisms
Elevated estrogen levels initially exert negative feedback on FSH and LH secretion by the anterior pituitary gland:
Decreased FSH levels prevent the development of another cohort of ovarian follicles in the same cycle
This also causes a slight drop in estrogen production
Decrease in FSH prevents recruitment and development of another cohort of ovarian follicles within the same cycle
Estrogen levels steadily rise due to granulosa cell proliferation
High estrogen stimulates additional estrogen production via positive feedback:
Estrogen production normally requires FSH
Estrogen usually exerts negative feedback on the release of FSH
Effects of estrogen on the hypothalamus and pituitary switch from negative to positive feedback, causing a surge in LH levels and a small increase in FSH before ovulation
Late Follicular Phase
During the late follicular phase:
With a surge of estrogen, the endometrium undergoes rapid growth/maturation - known as proliferative phase of the endometrial cycle
Granulosa cells secrete inhibin, progesterone, and estrogen → effectively regulating FSH and LH levels
Adequate levels of LH, FSH, and estrogen are necessary for progesterone production by granulosa cells
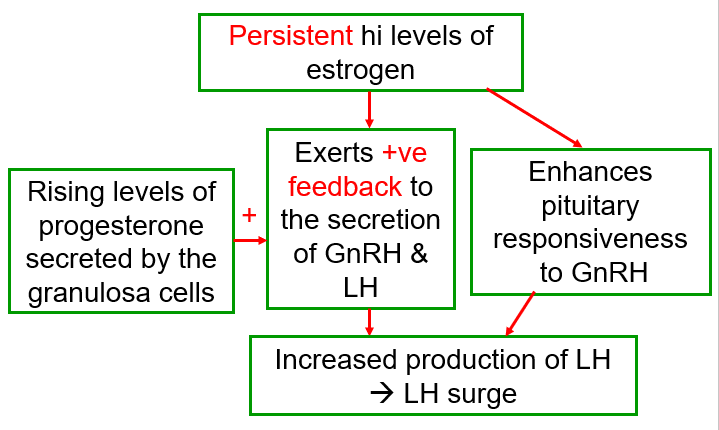
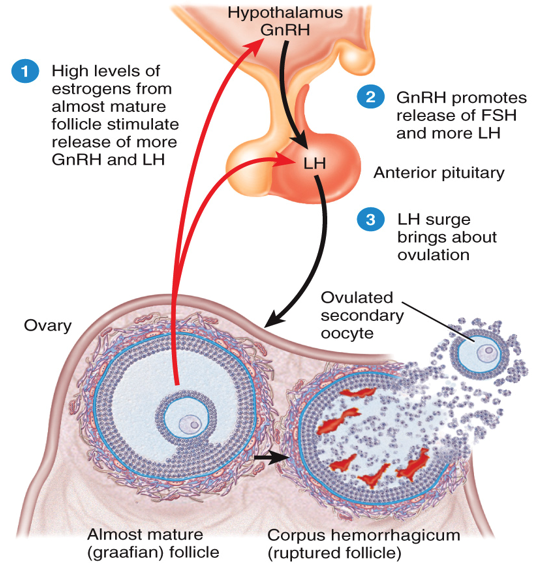
GnRH Production and LH Surge
High estrogen for a minimum of 2 days → positive feedback for the production of GnRH and LH
GnRH induces more FSH and LH production by the anterior pituitary
High estrogen levels condition the hypothalamus.
Rising progesterone levels increase LH production due to positive feedback mechanisms
Known as LH surge
High estrogen at late follicular phase stimulates growth of endometrium (3-4mm in thickness) - preparing the uterus for possible pregnancy
Estrogen also induces mucous glands of the cervix to produce watery mucous to facilitate sperm entry
LH surge causes primary oocyte to complete first meiotic division after ovulation
Ovulation Process
The LH surge results in:
Mature follicle secretes collagenase
Collagenase dissolves collagen enclosing the follicle
Break-down products of collagen induce inflammatory response
Inflammatory response attracts leukocytes that secrete prostaglandins
Rupture and Release of Oocyte
Prostaglandins cause outer theca layer of follicle to contract → rupturing the follicular wall
Antral fluid together with secondary oocyte spurts
Oocyte is then expelled into peritoneal cavity
Oocyte is then swept into Fallopian tube
Oocyte is either fertilized and turned into a zygote or dies
Post-Ovulation Hormonal Changes
Inhibin secretion increases under the influence in FSH and estrogen just prior to ovulation
Inhibin decreases GnRH release post-ovulation → reduced levels of LH and FSH:
Subsequently, the level of LH & FSH starts decreasing after ovulation
The second half of the menstrual cycle follows:
Aka the luteal phase
After ovum release, the follicle transforms into corpus luteum
Follicular cells remain as granulosa cells
Theca cells transform into luteal cells and begin secreting progesterone
Corpus Luteum Functions
Produces estrogen and inhibin
Progesterone and estrogen together stimulate further endometrial growth
The increasing levels of estrogen, inhibin, and progesterone suppress the hypothalamic-pituitary system
Resulting a drop in LH and FSH secretion after ovulation
Effects of Hormonal Drops
Drop in LH impacts the corpus luteum’s ability to produce estrogen and progesterone causing:
Induces endometrial degeneration
Leads to menstrual bleeding (menses)
The start of the menstrual phase of the endometrial cycle
Drop in estrogen and progesterone levels, diminishes the negative feedback on the hypothalamic-pituitary axis:
Gonadotropins (LH and FSH) secretion rise again
The start of a next menstrual cycle if no fertilization occurs
If fertilization occurs, the corpus luteum continues to produce progesterone