Introduction to the Profession
What is a CDA?
Not a protected title (yet): This means that while there are recognized programs for Communicative Disorders Assistants (CDAs), the title itself is not legally regulated in the same way as Speech-Language Pathologists (SLPs) or Audiologists.
Anyone can technically call themselves a CDA, which underscores the importance of adhering to professional standards and working under supervision.
The "CDA" title should be used by graduates of a recognized program (CDAAC: https://cdaac.ca/what-is-a-cda/):
To ensure competence and adherence to professional standards, it is recommended that individuals using the title "CDA" have completed a program accredited or recognized by associations like the Communicative Disorders Assistant Association of Canada (CDAAC).
Must be supervised by a Speech-Language Pathologist (SLP) or Audiologist: This is a critical legal and ethical requirement.
CDAs work under the direct or indirect supervision of a regulated health professional who bears primary responsibility for patient care, ensuring that services provided are appropriate, ethical, and safe.
Supportive personnel duties include: direct assignment of clinical tasks and related work to assist in intervention; involvement in assessment, therapy, consultation, professional development, and programming. These duties are crucial for enhancing service delivery. Examples include:
Direct assignment of clinical tasks: Implementing therapy plans developed by an SLP/Audiologist.
Assistance in intervention: Facilitating exercises, using communication aids, working on articulation, language, or auditory training goals.
Involvement in assessment: Preparing materials, transcribing patient responses, observing and documenting client behavior during assessments (but not interpreting results).
Therapy: Delivering prescribed therapy activities, providing feedback to clients, and collecting data on client performance.
Consultation: Participating in team meetings and providing observations to the supervising clinician.
Professional development: Engaging in continuous learning as directed or independently relevant to the scope of practice.
Programming: Assisting in the development or adaptation of therapy materials and programs under supervision.
What do CDAs actually do?
Considerations for practice: A CDA's specific daily tasks are highly variable, influenced by several key factors:
Setting (clinic, school, hospital, etc.): In a school, a CDA might work on literacy or social communication goals with children, while in a hospital, they might assist with dysphagia exercises for adults. A private clinic might focus on individual therapy sessions.
Population (age, communication disorders, etc.): Tasks will differ significantly between working with a young child with a speech sound disorder (e.g., using play-based therapy) and an elderly adult with aphasia (e.g., working on word retrieval strategies).
Format (individual, group, telepractice): Individual sessions allow for intensive, one-on-one focus. Group therapy requires different management and facilitation skills. Telepractice involves using virtual platforms and adapting materials for remote delivery.
Service model (direct service, consultative, educational): Direct service involves direct interaction with the client. Consultative involves providing support to caregivers or educators. Educational might involve contributing to workshops or resource creation.
Team dynamics and roles in the care team: CDAs must collaborate effectively with SLPs, Audiologists, educators, occupational therapists, physiotherapists, and other healthcare professionals, understanding their own defined role within the interdisciplinary or multidisciplinary team.
Core questions: What is therapy? (Encompasses the planned, evidence-informed interventions to address communication or auditory challenges). What is the typical day in the life of a CDA? (Highly varied, including direct client interaction, documentation, material preparation, team meetings, and administrative tasks). How do roles interact within a team? (Emphasizes collaboration, clear communication, and respecting professional boundaries and scopes of practice).
Organizations and their roles
CDAAC (Communicative Disorders Assistant Association of Canada)
National professional association: Represents the interests of CDAs across Canada.
Functions: advocacy (for the profession and its members), benefits (e.g., insurance, discounts), professional development (e.g., workshops, conferences, online courses).
Provides standards of practice and code of ethics: Essential guidelines for ethical and competent service delivery, helping to regulate the quality of CDA services despite the title not being provincially regulated.
Optional membership; open to CDA program graduates/students: Membership is a personal choice but offers significant professional advantages and recognition.
CASLPO (College of Audiologists and Speech-Language Pathologists of Ontario)
Provincial regulatory body for SLPs and Audiologists: Legally mandated to oversee and govern the professions of audiology and speech-language pathology in Ontario.
Protects the public and promotes public awareness: This is achieved by setting entry-to-practice requirements, developing and enforcing standards of practice, operating a complaints and discipline process, and ensuring only qualified individuals practice.
Mandatory for SLPs and Audiologists in Ontario: Practicing these professions in Ontario requires registration with CASLPO.
SAC (Speech-Language & Audiology Canada)
National professional association: Represents and supports SLPs, Audiologists, and communication health assistants across Canada.
Advocacy, benefits, professional development: Similar to CDAAC, it offers these services to its members at a national level.
Optional membership for SLPs, Audiologists, and "Communication Health Assistants": This includes CDAs, recognizing their role in supporting communication health services.
ASHA (American Speech-Language-Hearing Association)
National professional and credentialing association (US-centric): The primary professional and scientific credentialing association for audiologists, speech-language pathologists, and speech, language, and hearing scientists in the United States.
CCC: Certificate of Clinical Competence as a recognized credential (voluntary): While voluntary, attaining the CCC-A (Audiology) or CCC-SLP (Speech-Language Pathology) signifies a high level of competency and is widely recognized and respected in the US.
Regulated health professionals and public protection
Professionals are legally obligated to deliver competent, ethical, and professional services: This includes maintaining current knowledge, adhering to professional boundaries, and acting in the best interest of the client.
Regulators (like CASLPO) govern members to protect the public, under acts such as:
Regulated Health Professions Act, 1991 (RHPA): The overarching legislation for 26 self-regulated health professions in Ontario, establishing a framework for their governance and accountability.
Audiology and Speech-Language Pathology Act, 1991: Specific legislation detailing the scope of practice, controlled acts, and professional obligations for SLPs and Audiologists within Ontario.
Related regulations and by-laws: These provide detailed rules and procedures for specific aspects of practice, ethical conduct, quality assurance, and disciplinary processes.
Public-protection context: accountability to the public through the college; CASLPO administers regulatory oversight for audiology and SLP in Ontario. This accountability means that members are answerable to the College and, by extension, to the public for their professional conduct and quality of care.
Reference for regulation and public protection: HealthForceOntario.gov links (regulatory context for Ontario health professions). This resource provides comprehensive information on the regulatory landscape for healthcare professions in Ontario.
Legislation and acts overview**** ON tests
Relevant Ontario acts commonly referenced in practice: These acts establish the legal boundaries and responsibilities for healthcare providers and CDAs supporting them.
***Audiology and Speech-Language Pathology Act, 1991: Defines the professions' scopes and authorized acts.
Defines scope of practice for each profession:
Audiology is the assessment of auditory function and the
treatment and prevention of auditory dysfunction to develop,
maintain, rehabilitate or augment auditory and communicative
functions.
Speech-language pathology is the assessment of speech and language functions and the treatment and prevention of speech and language dysfunctions or disorders to develop, maintain, rehabilitate or augment oral motor or communicative functions.
● Authorized acts:
○ Audiologist can prescribe hearing aids, as an example
***Child, Youth and Family Services Act: Governs services for children and youth, including child protection, and outlines rights for young persons receiving services.
Rights of children and young persons receiving services
○ Corporal punishment prohibited
○ Physical restraint limited
● Parental consent:
○ To direct the child’s or young person’s education and upbringing, according to creed, community identity and cultural identity
○ Consent to, decline or defer services on behalf of their child
● Service providers must ensure that children and young persons and their parents have an opportunity to be heard and represented when decisions affecting their interests are made and when they have concerns about the services they are receiving.
● Duty to report a child in need of protection: reasonable grounds to suspect harm, abuse, neglect has happened or will likely happe
Education Act: Pertains to educational settings, influencing how services are delivered in schools.
Freedom of Information and Protection of Privacy Act: General privacy legislation for public institutions.
Health Care Consent Act, 1996: Outlines the requirements for obtaining informed consent for treatment decisions.
Valid and informed consent must be obtained
○ Prior to services starting
○ Whenever there is a change in the treatment plan
○ Written signature is not sufficient
● Describes what is informed consent: discussion involving the nature of service, expected benefits/risks, likely consequences of not receiving services, alternatives, and an opportunity to have questions answered
● Capacity
○ If the person is able to understand the information that is relevant to making a decision and able to appreciate the reasonably foreseeable consequences of a decision or lack of decision
○ No set age
○ When incapable: substitute decision make
Municipal Freedom of Information and Protection of Privacy Act: Privacy legislation for municipal bodies.
Personal Health Information Protection Act, 2004 (PHIPA): Specifically regulates the collection, use, and disclosure of personal health information (PHI).
Public Hospitals Act: Governs the operation of public hospitals in Ontario, impacting services delivered in these settings.
Regulated Health Professions Act, 1991 and the Health Professions Procedural Code: The foundational legislation for regulated health professions in Ontario.
Purpose: establish the legal framework for practices, consent, privacy, and accountability. These acts collectively ensure that healthcare services are provided legally, ethically, and with appropriate safeguards for individuals' rights and information.
Scope of practice: what the two professions cover
Audiology: The profession focuses on the auditory system.
Definition: assessment of auditory function (e.g., hearing tests, balance assessments) and the treatment and prevention of auditory dysfunction (e.g., providing hearing aids, audiological rehabilitation, tinnitus management) to develop, maintain, rehabilitate, or augment auditory and communicative functions.
Speech-Language Pathology (SLP): The profession focuses on communication and swallowing.
Definition: assessment of speech and language functions (e.g., articulation, fluency, voice, expressive/receptive language, cognitive-communication) and the treatment and prevention of speech and language dysfunctions (e.g., therapy for speech sound disorders, language delays, aphasia, voice disorders, stuttering, dysphagia) to develop, maintain, rehabilitate, or augment oral motor or communicative functions.
Authorized acts (example): An Audiologist can prescribe hearing aids in appropriate contexts. These are specific actions that, by law, can only be performed by a regulated professional (Audiologist or SLP) because they involve a significant risk of harm if performed by an unqualified individual.
These scopes are defined by the Audiology & Speech-Language Pathology Act (1991): This act legally delineates what Audiologists and SLPs are permitted to do in Ontario, and importantly, what is considered a "controlled act."
Children, youth, and family services context
CYFSA rights: protection of children and young persons receiving services. The Child, Youth and Family Services Act (CYFSA) outlines specific rights for children and youth, ensuring their safety, well-being, and participation in decisions affecting them.
Corporal punishment prohibited; physical restraints limited: Safeguards against physical harm and ensures that any necessary restraints are used only under specific, protective conditions.
Parental consent: parents/directors can consent to education/upbringing; consent for services (accept/decline/defer) for the child. Parents or legal guardians typically provide consent for minors for various services, including healthcare, and have the right to accept, decline, or postpone interventions.
Service providers must ensure that children, youth, and parents have opportunities to be heard and represented in decisions that affect their interests: This emphasizes child-centered practice and family involvement in care planning.
Duty to report: reasonable grounds to suspect harm, abuse, or neglect. All professionals, including CDAs, have a legal and ethical obligation to report to Children's Aid Society if there are reasonable grounds to suspect a child is in need of protection, even without definitive proof.
Health care consent and capacity
Health Care Consent Act: informed consent is required and ongoing. Consent for any healthcare treatment must be informed, meaning the person understands what they are agreeing to, and it is a continuous process, not a one-time event, especially if the treatment plan changes.
Informed consent includes:
Nature of the service: A clear explanation of what the intervention or assessment entails (, , ).
Expected benefits and risks: A realistic discussion of the potential positive outcomes and any possible negative effects or side effects.
Likely consequences of not receiving services: An explanation of what might happen if the individual declines the proposed intervention.
Alternatives: A description of other available treatment options, including the option of no treatment.
Opportunity to ask questions: The individual must be given ample opportunity to clarify any uncertainties and feel comfortable with their decision.
Capacity: ability to understand relevant information and foresee consequences of decisions. A person is considered capable if they can appreciate the information required for consent and understand the potential outcomes of their choices.
No fixed age; if incapable, substitute decision maker applies: Capacity is assessed on a case-by-case basis, not just by age. If a person is found to be incapable, a substitute decision-maker (e.g., parent, legal guardian, power of attorney for personal care) will provide consent on their behalf.
RHPA and controlled acts
RHPA applies to 26 colleges; aims to protect the public, ensure high-quality care, and hold regulated professions accountable: The Regulated Health Professions Act (RHPA) is the framework for all self-regulated healthcare professions in Ontario, establishing consistent principles for public protection.
There are 14 controlled acts under RHPA; these involve substantial risk and can only be performed by qualified regulated health professionals: Controlled acts are specific, high-risk procedures that only authorized regulated health professionals are legally permitted to perform, due to the potential for harm if done by an unqualified individual.
Examples of controlled acts include: diagnosing (identifying a disease or condition), performing procedures on tissue under the dermis (e.g., injections), setting fractures, prescribing drugs, and certain psychotherapy interventions. For SLPs/Audiologists, prescribing hearing aids (Audiology) and certain types of dysphagia assessments may involve components of controlled acts.
PHIPA: privacy and information handling
Rules for collection, use, disclosure, disposal, and retention of personal health information (PHI): The Personal Health Information Protection Act (PHIPA) sets out stringent rules governing every stage of handling confidential health data.
Individuals have the right to access their health records: Clients can request to view or obtain copies of their personal health information, with certain legal exceptions.
Organizations must implement secure practices and mitigate privacy risks: This includes technical safeguards (e.g., encryption, password protection) and administrative measures (e.g., staff training, clear privacy policies) to protect PHI from unauthorized access or breaches.
Breach protocol: notify the affected person and the privacy commissioner if a breach occurs. In the event of a privacy breach (e.g., lost files, unauthorized access), organizations are legally obligated to promptly notify the individuals whose PHI has been compromised and, in significant cases, the Information and Privacy Commissioner of Ontario.
Support personnel: use by audiologists and SLPs
General approach: Supportive personnel are used to enhance service delivery, not replace clinician judgment. CDAs extend the reach of SLPs and Audiologists by carrying out specific tasks, but they do not make independent clinical decisions or diagnoses.
Shared responsibilities and accountability:
Supervising clinician bears legal and ethical responsibility for all services provided/omitted: The SLP or Audiologist remains ultimately accountable for the quality and safety of care, even when tasks are delegated.
Onus is on the registrant for supervision quality and patient safety: The regulated professional must ensure their supervision is adequate and that the client's safety is prioritized at all times.
Supervision requirements (common to both professions): These ensure effective oversight and professional development.
CASLPO membership in good standing: The supervising professional must be a currently registered and compliant member of CASLPO.
Demonstrated supervision competency: The supervisor must possess the skills and knowledge to effectively supervise, which may require specific training.
Informed consent for supportive personnel involvement: Clients must be informed that a CDA will be involved in their care and provide explicit consent for this arrangement.
Clear assignments and roles for support personnel: Tasks delegated must be clearly defined, within the CDA's competency, and aligned with therapy goals.
Ensure support personnel understand assigned tasks and competencies: The supervisor must verify the CDA's understanding and ability to perform the task safely and effectively.
Appropriate completion and documentation of tasks: The CDA is responsible for accurately completing assigned tasks and maintaining thorough records, which the supervisor reviews.
Sufficient ongoing direct contact with clients: The supervising clinician must have enough direct interaction with the client to maintain awareness of their progress and make clinical judgments.
Maintain strong working relationships to support growth/learning of support personnel: A collaborative and supportive environment fosters professional development for the CDA.
Be readily available for support and discussion: The supervisor must be accessible for questions, concerns, and debriefing.
Mitigate risks and establish a supervision model: Proactive identification and management of potential risks, coupled with a clearly defined supervision plan.
Model of supervision: balance of direct and indirect supervision; the amount/type depends on: The intensity and format of supervision are dynamic and adapted based on several factors:
Complexity of patient profile: Clients with complex needs (e.g., multiple diagnoses, severe impairments) typically require more direct supervision.
Risk of harm associated with the task: Tasks carrying higher risk to the client necessitate more direct oversight.
Competence, experience, and comfort of the support personnel: A less experienced CDA or one new to a specific task will require closer supervision.
Clinician comfort and experience with the task: A supervisor unfamiliar with a specific intervention may require closer observation of the CDA's execution.
New tasks or new supervisory relationships: More direct and frequent supervision is needed during initial phases.
Direct vs indirect supervision
Direct supervision:
In-view observation and real-time guidance during patient interaction: This is the most intensive form of supervision, where the supervisor is physically present or observing remotely in real-time.
In person, real-time video, or as close to the session as possible: Examples include the SLP sitting in on a therapy session, or observing via a live video feed, providing immediate feedback.
Indirect supervision:
Record review, clinical discussions/meetings: This involves reviewing documentation (e.g., progress notes, data sheets) and discussing client progress or challenges in scheduled meetings.
Evaluation of audio/video recordings of sessions: The supervisor reviews recorded sessions after they have occurred, providing retrospective feedback and analysis.
When assigned tasks are not performed as directed
The supervising clinician must determine and direct an appropriate course of action, which may include: This ensures client safety and continuous quality improvement.
Further training: Providing additional instruction, resources, or mentorship to address skill deficits.
Increased supervision: Temporarily increasing the frequency or intensity of direct supervision.
Reassignment: Modifying the delegated tasks or reassigning them if the CDA lacks the necessary competency or if the task poses a risk to the client.
Observation requirements for support personnel
All support personnel must be directly observed providing patient intervention on a regular basis: This ensures that the CDA is consistently meeting professional standards and that their skills are being maintained and developed. "Regular basis" means frequent enough to ensure proper oversight of clinical quality.
However, not every patient needs direct observation every time: Supervision is risk-informed; less complex cases or highly competent CDAs may require less frequent direct observation, allowing for a more balanced supervision model.
CDA competencies: general, screening, therapy
General:
Knowledge of legislation, regulations, by-laws, standards (e.g., confidentiality of client information, maintaining professional boundaries, adhering to safety protocols, appropriate documentation practices): CDAs must understand the legal and ethical framework governing their practice.
Seek clarification/support from SLP as needed: Recognizing one's limitations and knowing when to ask for help from the supervisor is a critical competency.
Engage in continued professional development: Staying current with best practices, new research, and relevant skills is essential for effective practice.
Screening:
Follow established protocols: CDAs can administer screenings using standardized procedures, but they do not make diagnostic interpretations.
Therapy:
Develop materials (e.g., tech skills): Creating or adapting therapy aids, visual supports, or using technology (e.g., specific apps, telepractice platforms) to support intervention.
Carry out treatment based on therapy goals: Implementing therapy plans as designed by the SLP/Audiologist.
Elicit/record patient response data: Systematically collecting and documenting client performance during therapy sessions (e.g., percentage correct, number of trials).
Plan/Explain carryover activities (home practice): Providing clear instructions and demonstrations to clients and caregivers on how to practice skills between sessions.
Assist with education/training sessions: Supporting the SLP/Audiologist in delivering information or training to clients, families, or other professionals.
Activity: what you can and cannot do (CDA context)
Can do/Can’t do examples (typical tasks for screening, assessment, and therapy support):
Can do: Collect information (e.g., case history forms, developmental milestones checklist), Chart review (to gather background information), Assist during an assessment (e.g., transcribing client responses, managing materials, interacting with the client under direct supervision), Conduct a screening and indicate results: “pass”, “fail” (based on objective criteria), Participate in interdisciplinary rounds (to report observations).
Can’t do: Admit, discharge or refer (these are clinical decisions made by a regulated professional), Selection of assessment tools/procedures (requires diagnostic expertise), Interpret screening results: “you have a hearing problem” (this is a diagnosis), Communicate examination results: “moderate hearing loss” (this constitutes conveying a diagnosis).
Other responsibilities may include: making clinical recommendations (cannot, only observe), providing home practice suggestions (can, if pre-approved by supervisor), adjusting goals (cannot, based on clinical judgment), supervising other support personnel (cannot, requires regulated status), training (can assist), report writing (can contribute data), administrative tasks (ordering devices, scheduling - generally can), running parent/educator workshops (can assist).
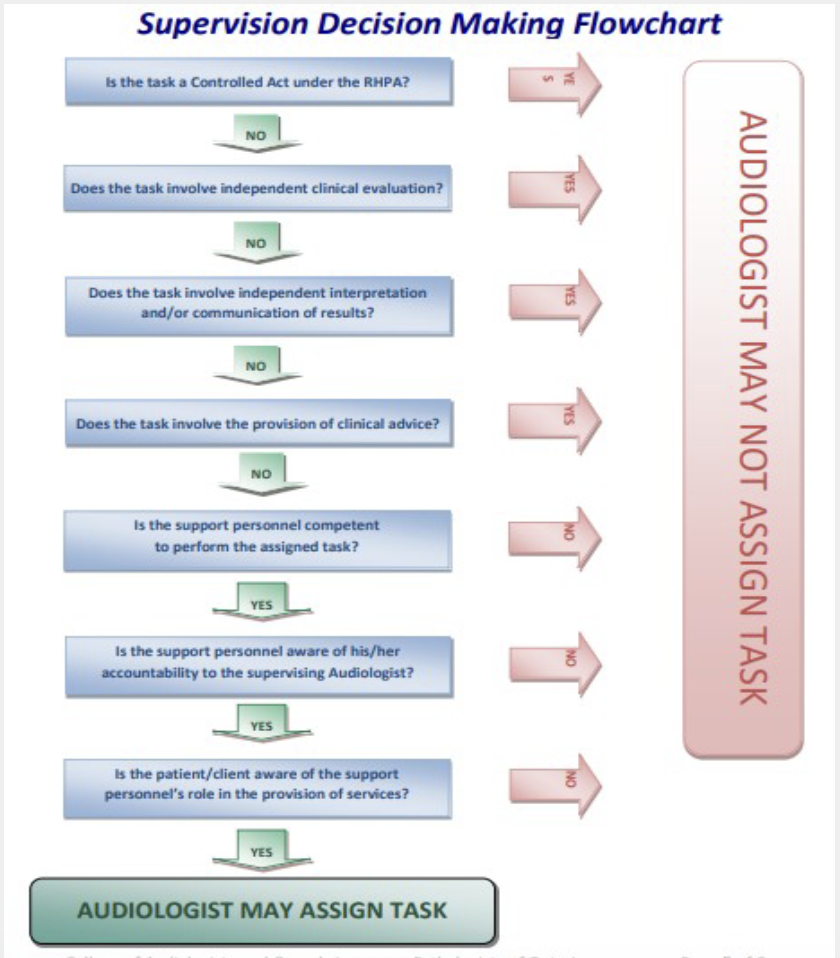
Supervision decision-making flowchart (Ontario CASLPO guidance)
Key decision steps to determine if a task can be assigned: This systematic process ensures that delegation is safe and appropriate.
Is the task a Controlled Act under RHPA? If yes, proceed with nurse/clinician oversight per regulations: If the task is a controlled act, it cannot be delegated to a CDA directly (unless it falls under specific exemptions for regulated professionals).
Does the task involve independent clinical evaluation? If yes, primary clinician must authorize: Independent judgment and evaluation are the domain of the regulated professional.
Does the task involve independent interpretation and/or communication of results? If yes, require higher level supervision: Interpreting findings or communicating diagnoses falls outside the CDA's scope.
Does the task involve the provision of clinical advice? If yes, ensure competency and oversight: Providing advice often requires clinical judgment, necessitating close supervision if delegated.
Is the support personnel competent to perform the task? If no, assignment is not appropriate: The CDA must have the necessary skills and knowledge.
Is the support personnel aware of accountability to the supervising Audiologist? If yes, proceed; if no, do not assign: The CDA must understand that their actions ultimately fall under the supervisor's responsibility.
Is the patient/client aware of the support personnel's role? If yes, proceed; if no, do not assign: Informed consent is crucial; clients must know who is providing care.
Outcome: Audiologist may assign the task if all criteria are satisfied; otherwise, task cannot be assigned. If any of these questions yield a negative or uncertain answer, the task should not be delegated.
Source: Position Statement - Use of Support Personnel by Audiologists (CASLPO). This document provides official guidance.
Professional misconduct by registrants
Examples of professional misconduct include: These actions can lead to disciplinary proceedings against the regulated professional.
Failing to appropriately supervise a person whom the member is obligated to supervise: This directly relates to the safe and legal use of CDAs; inadequate supervision constitutes misconduct.
Permitting or helping a non-member to represent themselves as a member: Allowing a CDA to imply they are an SLP or Audiologist.
Inappropriately using a term, title, or designation in respect of the member’s practice (e.g., indicating a non-accurate specialization): Misrepresenting one's own qualifications or areas of expertise.
Summary and reflections
The unit covers: roles of CDAs, SLPs, and Audiologists; regulatory framework (e.g., RHPA, Audiology and Speech-Language Pathology Act); the purpose of professional organizations (e.g., CDAAC, CASLPO, SAC, ASHA); the scope of practice for SLPs and Audiologists; principles of consent and capacity; the appropriate use of support personnel; effective supervision models (direct vs. indirect); and expectations for professional conduct (e.g., related to PHIPA and misconduct).
Reflection prompts (from class):
What is the most important organization discussed today and why?: This encourages students to synthesize information and prioritize based on impact (e.g., regulatory body for public protection, professional association for member support).
What are key takeaways about licensing, supervision, and professional responsibilities?: Prompts students to identify core concepts.
What are questions or areas needing further clarification?: Encourages critical thinking and self-assessment of understanding.
Connections to real-world practice and ethics
Public protection and accountability are central to regulatory bodies (CASLPO) and professional associations (CDAAC, SAC, ASHA): These organizations, through their various functions, ensure that the public receives safe and ethical care.
Informed consent and capacity are ongoing obligations in clinical work with children and adults: Every clinical interaction requires continuous attention to these principles.
Privacy laws (PHIPA) govern how PHI is collected, stored, disclosed, and protected: Adherence to PHIPA is non-negotiable for all healthcare providers and support personnel.
The use of support personnel requires careful supervision planning to ensure patient safety, quality of care, and continued professional development for all team members: Effective supervision is dynamic and essential for leveraging CDAs' skills while maintaining high standards.
Ethical practice includes avoiding misrepresentation of credentials, maintaining confidentiality, and ensuring competency before delegating tasks: These are fundamental principles for all professionals and those working under their supervision.
On the test: professional misconduct
What are the important skills you need as a clinician