lecture 12
noninvasive
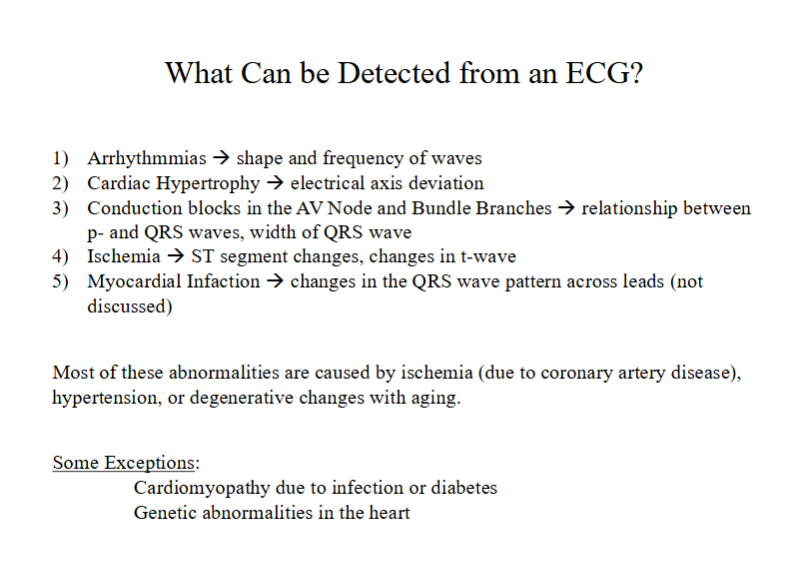
irregular rhythm
enlargment of the ventricles (right or left)
blocks in the conduction system
if the heart is getting enough oxygen
going through heart attack or had one in the past
whats the underlying cause of most abnormalities in the heart?
ischemia (#1) - usually caused by coronary artery disease, also blood clot
hypertension - causes remodeling of the heart bc the heart is not working as well
degenerative changes with aging - fibrosis (inteferes with conduction system)
exceptions
cardiomyopathy (heart not pumping adequetly) - infection, diabetes
genetic abnormalities
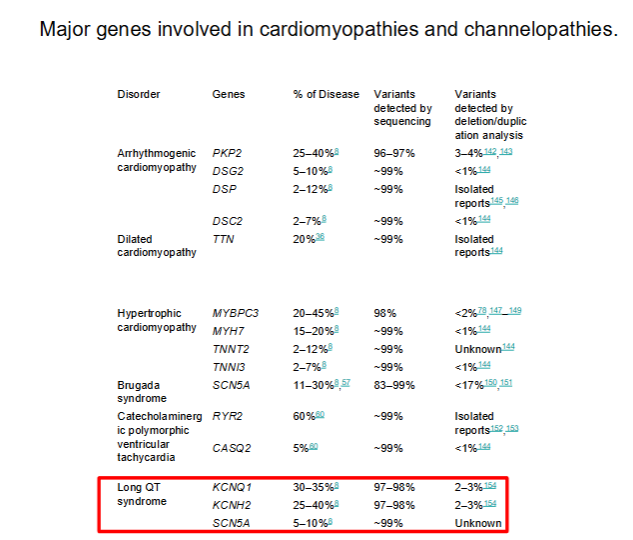
dilated cardiomyopathy - heart is expanded and doesnt contract properly
gene affected is called titin (TTN) - holds myosin molecules to the z lines in sarcomeres
impaired sarcomere structure
brugada syndrome - irregular rhythm due to mutations in the fast sodium channel (SCN5A)
long QT syndrome - due to mutations in the fast sodium channel or one of the delayed rectifier potassium channels
one of the most common heart abnormalities
common in young people
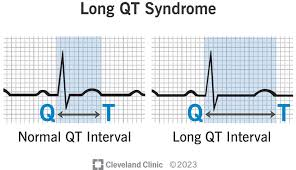
delayed repolarization
v tach - fast irregular ventricular contraction - pvcs in a row
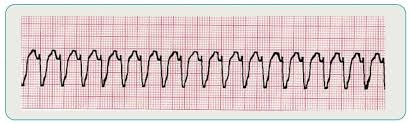
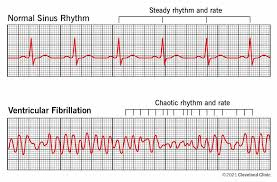
ventricles are just twitching - not pumping (dangerous) → fainting → death
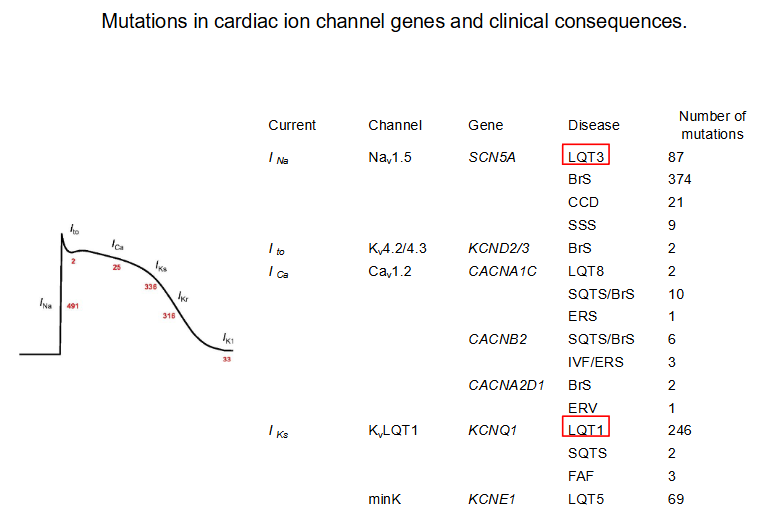
SCN5A - fast Na+ channel, KCNQ1 - delayed rectifier K+ channels
491 = 491 mutations of fast sodium channels in humans
LQT1 and LGT3 bot have a number of mutations
1 is the most common
and most common cause of sudden death in young people
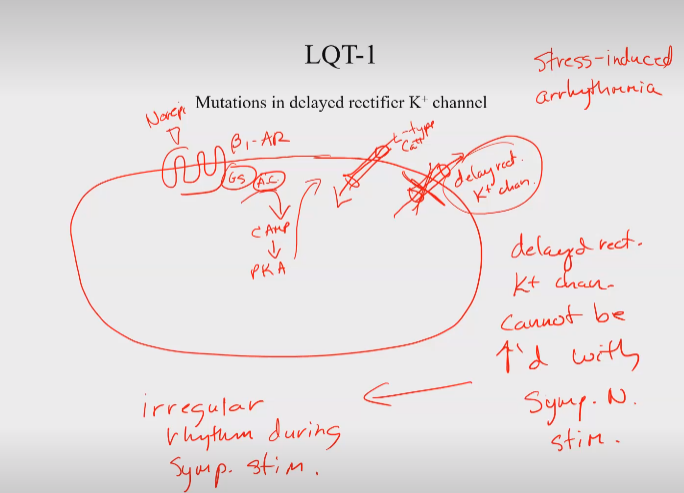
beta 1 adrenargic receptor on myocyte
NE binds to it → → adenylyl cyclase → cAMP → PKA
L type calcium channel and delayed rectifier potassium channels
both must be activated in coordinated way
more ca coming in during plateau, more K+ leaving during repolarization
activate SNS → activate both channels (in coordinated way)
if the delayed rect K+ channel cannot be increased with the sympathetic nerve stimulation → myocytes uncoordinated → irregular rhythym
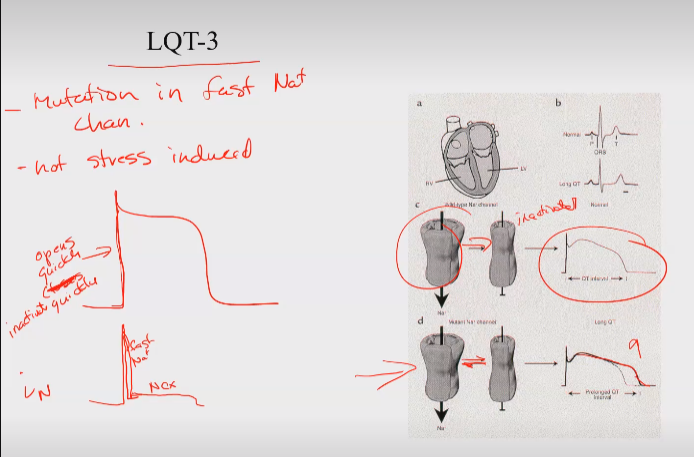
fast na+ channel
normal: opens quickly then inactivates quickly
LQT-3: flickers between open and inactivates state → delays repolarization
HR controlled by the SNS and PNS
average pressure in the
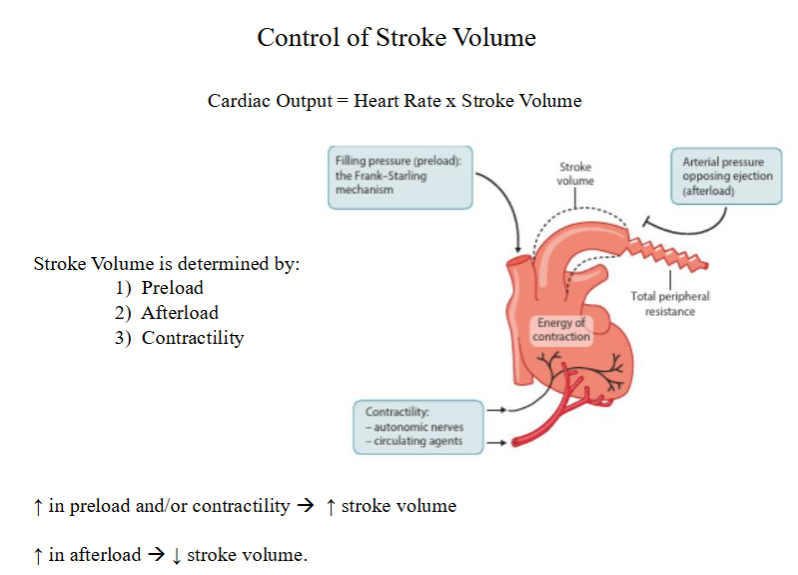
preload is the amount of blood in the ventricles before contraction, essentially the stretch of the heart muscle, while afterload is the resistance the heart must overcome to pump blood out, influenced by factors like arterial pressure and vascular tone.
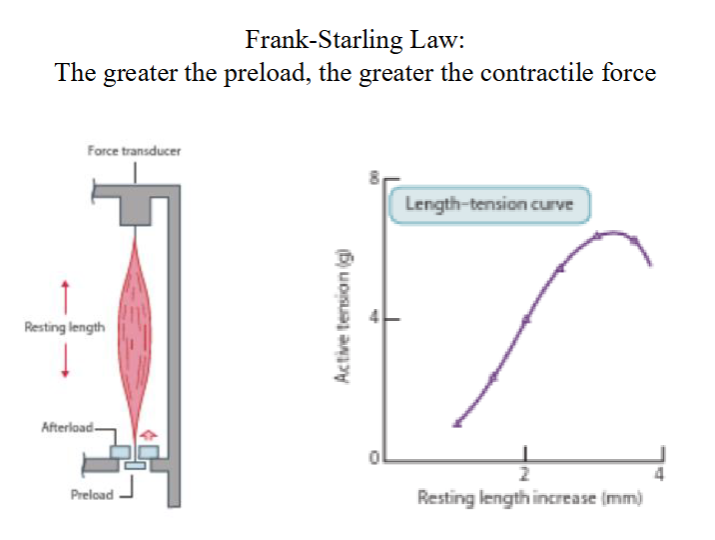
test on single myocyte
different preloads = different stretch
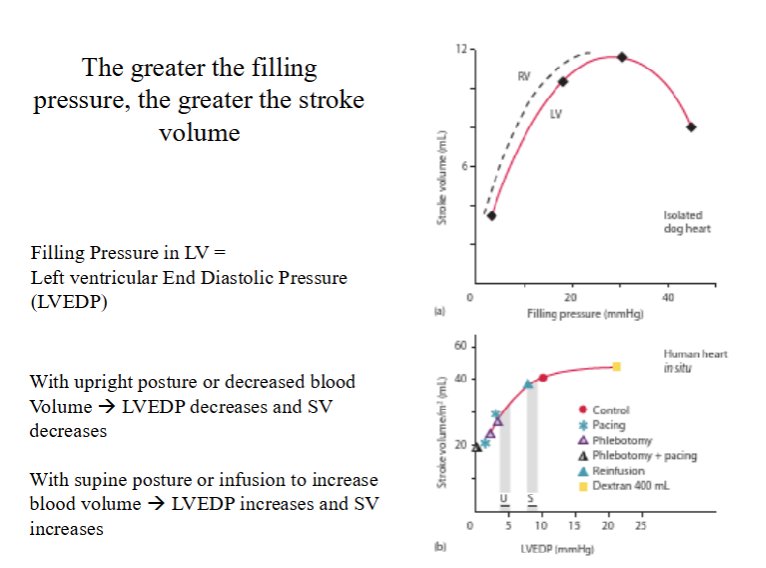
isolated dog heart
actually in viva in human
muscle pump exerts more pressure on venus
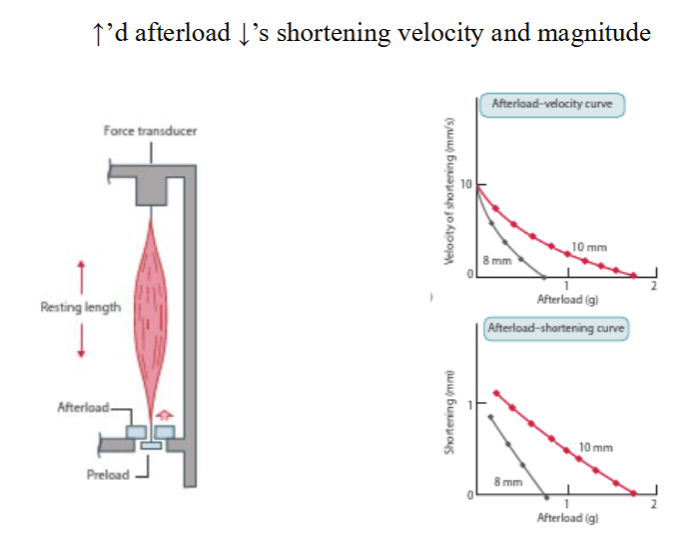
afterload is like the weight it has to overcome to contract or something
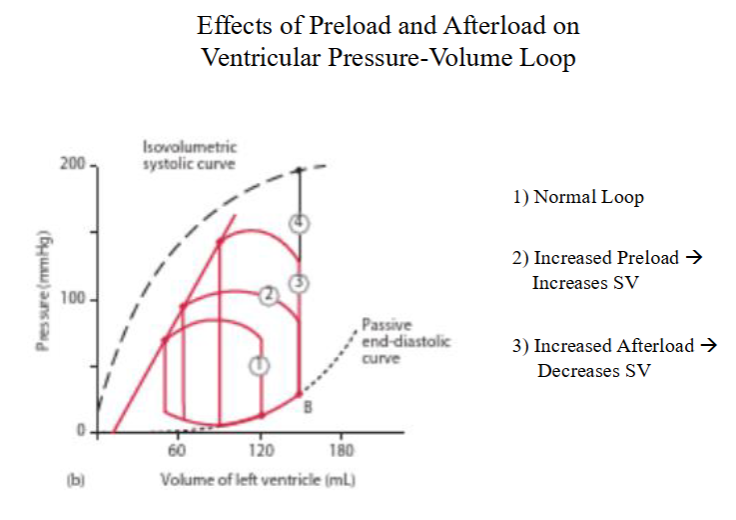
left to right line is SV