[LEC] Lec 5.2 - Neuroana 3.docx
CRANIAL NERVES
- Damage: ipsilateral
- Spinal nerve damage: contralateral
- CN Name: Oh Oh Oh To Touch And Feel A Girl’s Vagina Ahh Heaven
- CN Function: Some Say Marry Money But My Brother Says Big Brain Matters More
Introduction
CN 1: Olfactory
- Smell / olfaction
- Function: Purely sensory
- Lesion/impairment: Anosmia (loss of smell)
| Q: TBI with loss of appetiteA: CN 1 (Closely connected senses are taste and smell)Anomia: inability to name (aphasia) |
|---|
CN 2: Optic
- Vision
- Function: Purely sensory
- Lesion/impairment: anopsia (loss of vision)
| Homonymous hemianopsia: most commonArteries affected: MCA & PCA |
|---|
CN 3: Oculomotor
- Function: Purely motor
- PERRLA
CN 4: Trochlear
- Function: Purely motor
- Innervates superior oblique (SO4)
- Down
- In
- Causes in-torsion: inward rotation of eyes
CN 5: Trigeminal
- Mastication
- MMT: closure of mouth
- Biting a burger: closure
- L: opens mouth
- Masseter: strongest muscle in the body
- “TriCHEWminal”
- Function: Motor & Sensory
- Lesion/Impairment: trigeminal neuralgia 🡪 Tic Doloureux
3 divisions
- V1: Ophthalmic
- V2: Maxillary
- V3: Mandible
CN 6: Abducens
- Function: Purely motor
- Innervates lateral rectus (LR6): abducts eyes
- Lesion/Impairment: diplopia (double vision; horizontal – most common)
CN 7: Facial
- Lesion/Impairment: Bell’s Palsy / Prosopoplegia (paralysis of the face)
| Prosopagnosia: agnosia of face (familiar)Differential diagnosisStroke (1/4): contralateral lower quadrant of face (corticobulbar: brainstem)Bell’s palsy (1/2): entire half of the face |
|---|
CN 8: Vestibulocochlear
- Auditory (cochlea) & Balance (vestibulo)
- Lesion/impairment: Meniere’s disease
- Vertigo: umiikot vision
- Tinnitus: ringing in the ear
- Sense of fullness dt high pressure
CN 9: Glossopharyngeal
- Taste & swallowing
- 9 & 10
- Innervates pharynx
- Gag / swallowing reflex
- Dysphagia
CN 10: Vagus
- Chin-tuck: facilitate swallowing
CN 11: Spinal Accessory
- Innervates SCM & Trapezius muscles
CN 12: Hypoglossal
- Tongue movements
- Tongue deviation:
- contralateral to lesion (CVA)
- ipsilateral to lesion (PNS/LMNL)
- Innervates most tongue muscles except for palatoglossal
Location of the Cranial Nerves
- Brainstem
- Except:
- CN 1: Telencephalon (cerebrum & basal ganglia)
- CN 2: Diencephalon (SHET - Subthalamus, Hypothalamus*, Epithalamus, Thalamus)
- Supplied by Posterior Circulation (Vertebrobasilar artery)
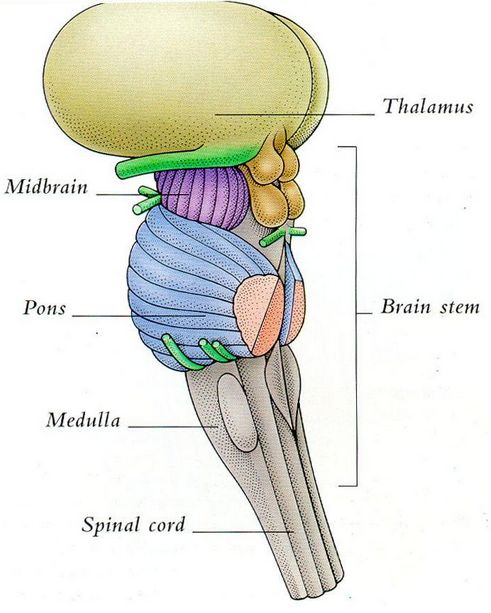
- Midbrain
- proprioception
- CN 3 & 4
- Pons
- Bridge
- CN 5, 6, 7 (motor), 8
- Medulla
- CN 7 (sensory: nervus intermedius), 8, 9, 10, 11, 12
| Increased Intracranial Pressure = ruptured blood vessels 🡪 herniate brain down to foramen magnum 🡪 nausea |
|---|
Brainstem Stroke Syndrome
- Cerebrum: Anterior circulation
- Brainstem: Posterior circulation
- Weber
- Medial basal of the Midbrain
- CN 3
- Benedikt
- Tegmentum of the midbrain
- CN 3
- Locked-in
- Vertical eye movements are spared
- Bilateral Basal of the Pons
- All CNs
- Millard-Gubler
- Lateral Pons
- CN 6, 7
- Wallenberg / Pica Syndrome
- PICA: Posterior-inferior cerebellar artery
- Lateral medulla: spinal nucleus only
- CN 5 (sensation of pain & temperature)
- Dysphagia
- (+) Horner’s syndrome
- Crossed hemianesthesia
- Loss of pain & temperature sense in
- Face: ipsilateral
- Body: contralateral
*evan’s part*
CN 2: Optic
- *evan’s part*
Amaurosis Fugax (Monocular Blindness)
- Anterior Circulation
- Involved Internal Carotid Artery (ophthalmic A.)
Tests
- Snellen’s Chart
- 20 ft distance
- central visual acuity
- N = 20/20 acuity
- Confrontation Test
- Peripheral Visual Acuity
Additional Tests
- Ishihara: color vision testing
- Tonometry: intra-pressure measurement
- Glaucoma = ↑ Intraocular pressure
- Retinoscopy: refraction error
Visual Pathway
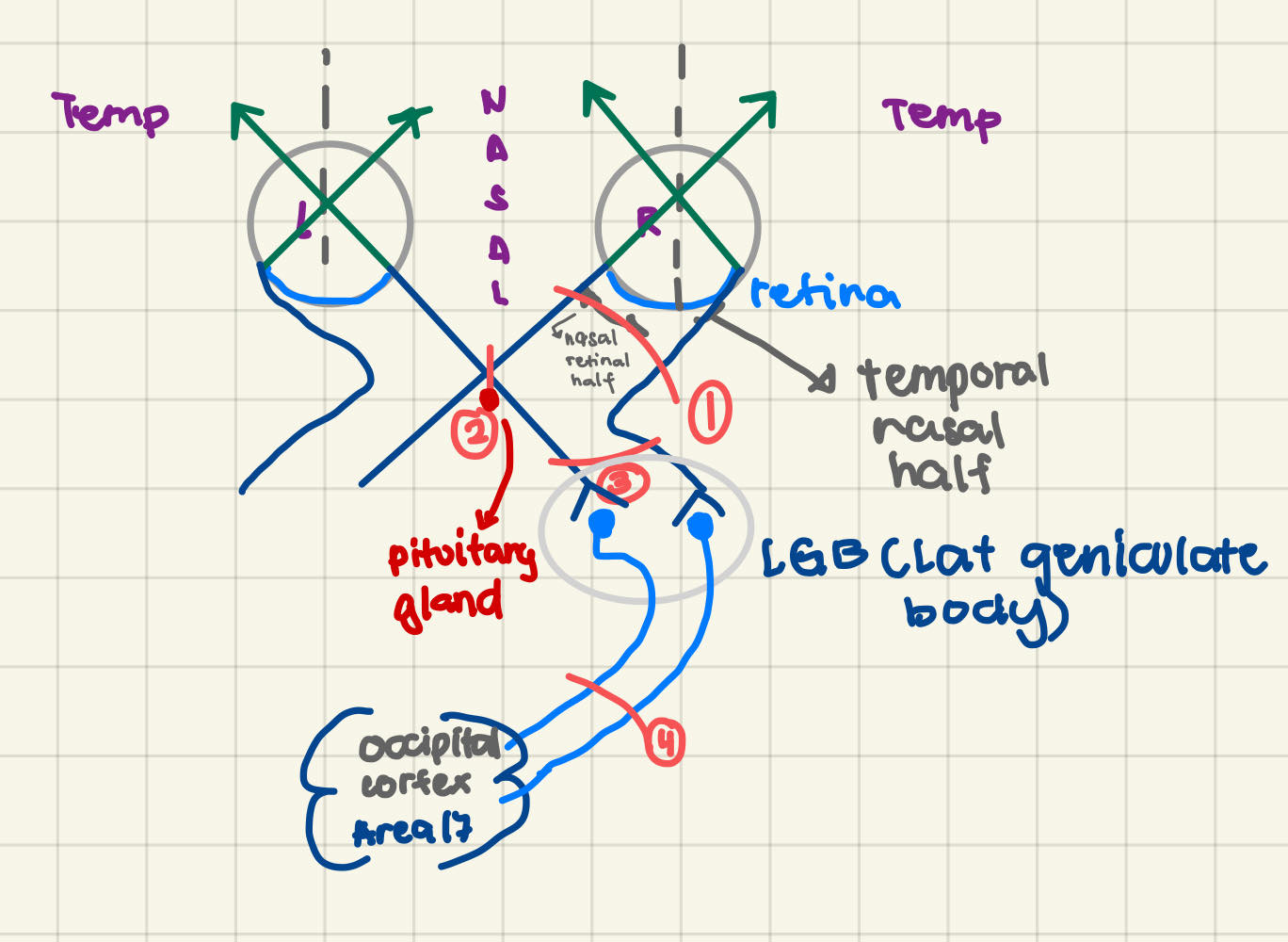
- Parts
- Optic Nerve
- Optic Chiasm
- Optic Tract
- Optic Radiation
- Occipital Cortex: Brodmann 17
| Lesion | Manifestation | |
|---|---|---|
| Optic Nerve | Monocular Blindness (IPSI) |  |
| Optic Chiasm | Bitemporal Hemianopsia - loss of peripheral vision |  |
| Optic Tract/ Optic Radiation/ Occipital Cortex | Homonymous Hemianopsia: contralat fr visual field |  |
| Optic Radiation: Upper fibers (parietal lobe) | Quadrantanopiacontralat |  |
| Optic Radiation: Lower fibers(temporal lobe) |  |
| Px has L homonymous hemianopsia?L Optic NerveOptic ChiasmR Optic NerveR Optic Tract Lesion to L Optic Tract will manifest~~R Nasal + R Temporal VFLL Nasal + L temporal VFL~~R nasal + L Temporal VFLL Nasal + R Temporal VFL Px has R CVA with L Homonymous Hemianopsia. Initially in bed. Where will you put the trayR side of bed → intactL side of bedLesion to upper fibers of L Optic Radiation → (R) Lower Quadrantanopia Lesion to Parietal fibers of R Optic Radiation → (L) Lower Quadrantanopia |
|---|
Pupillary Light Reflex
- Direct: constrict
- Consensual: constrict even if there's no light
- Afferent: CN2 (Direct)
- Efferent: CN3 (Consensual)
- Normal Reaction
- (+) Direct Light Reflex
- (+) Consensual Light Reflex
- pretectal area
- superior colliculi
- visual reflex
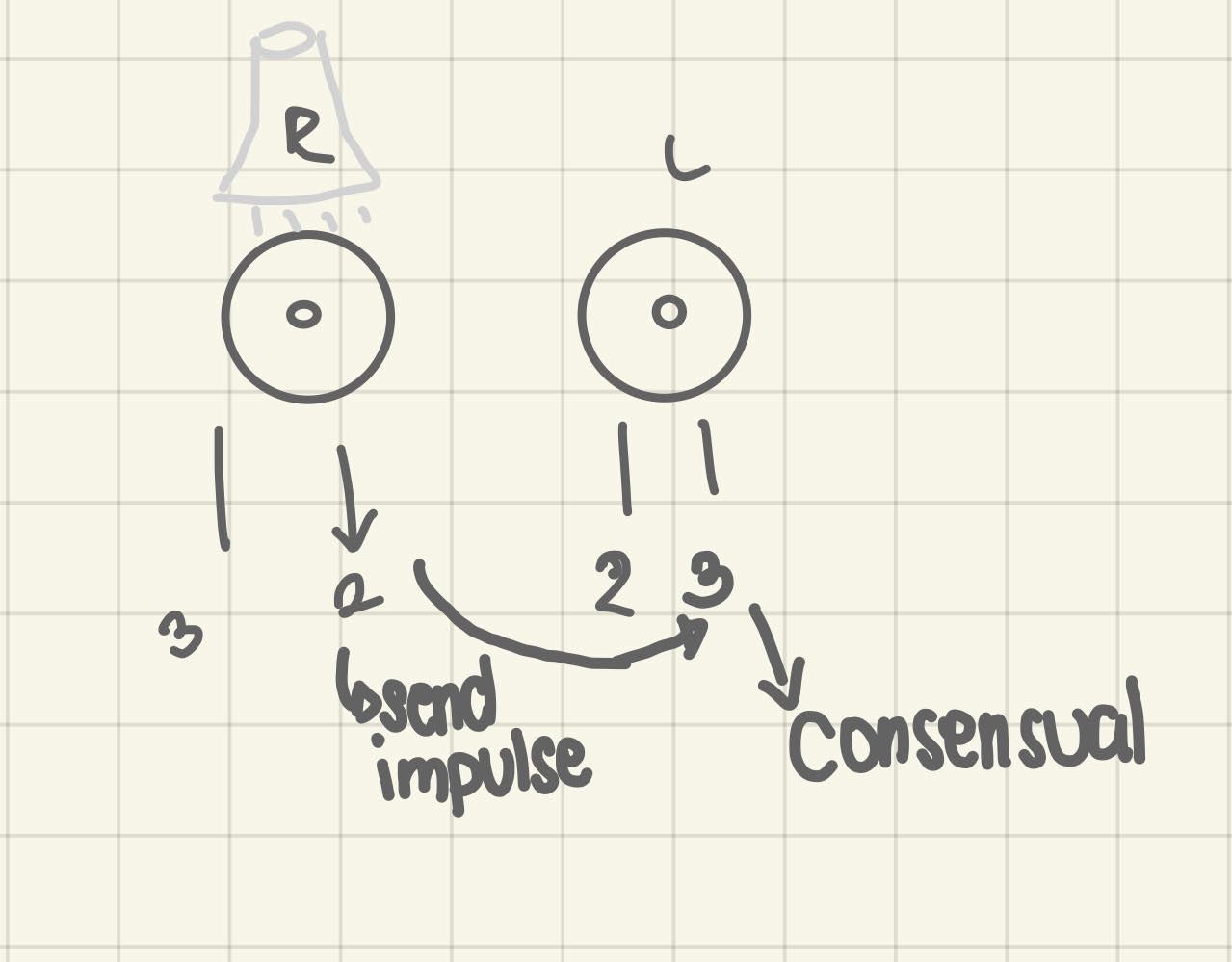
| Case 1. Light was shone on the R eye. What CN is affected?(-) Direct Light Reflex(+) Consensual Light ReflexR CN 2R CN 3L CN 2L CN 2Case 2. Light was shone on the R eye(-) Direct Light Reflex(-) Consensual Light ReflexWhen light was shone on the L eye(+) Direct and Consensual ReflexR CN 2R CN 3L CN 2L CN 2Anisocoria23both - unequal size of pupilsneither |
|---|
CN 3: Oculomotor
- Edinger-Westphal Nucleus
- PERRLA -> pupils equally round, reacted to light accommodation
- Ptosis may happen in
- Myasthenia Gravis
- CN3 palsy
- Horner’s Syndrome
- Edema d/t Inferior flexion
- Damage causes: Mydriasis (Dilated Pupil) → Sympathetic
- CN3: constrict damage pupil
CN 3, 4, 6
- Formula: EOM3LR6SO4
| Lateral Rectus | CN 6 |
|---|---|
| Superior oblique | CN4 |
| Medial Rectus | CN 3 |
| Inferior Oblique | |
| Superior Rectus | |
| Inferior Rectus |
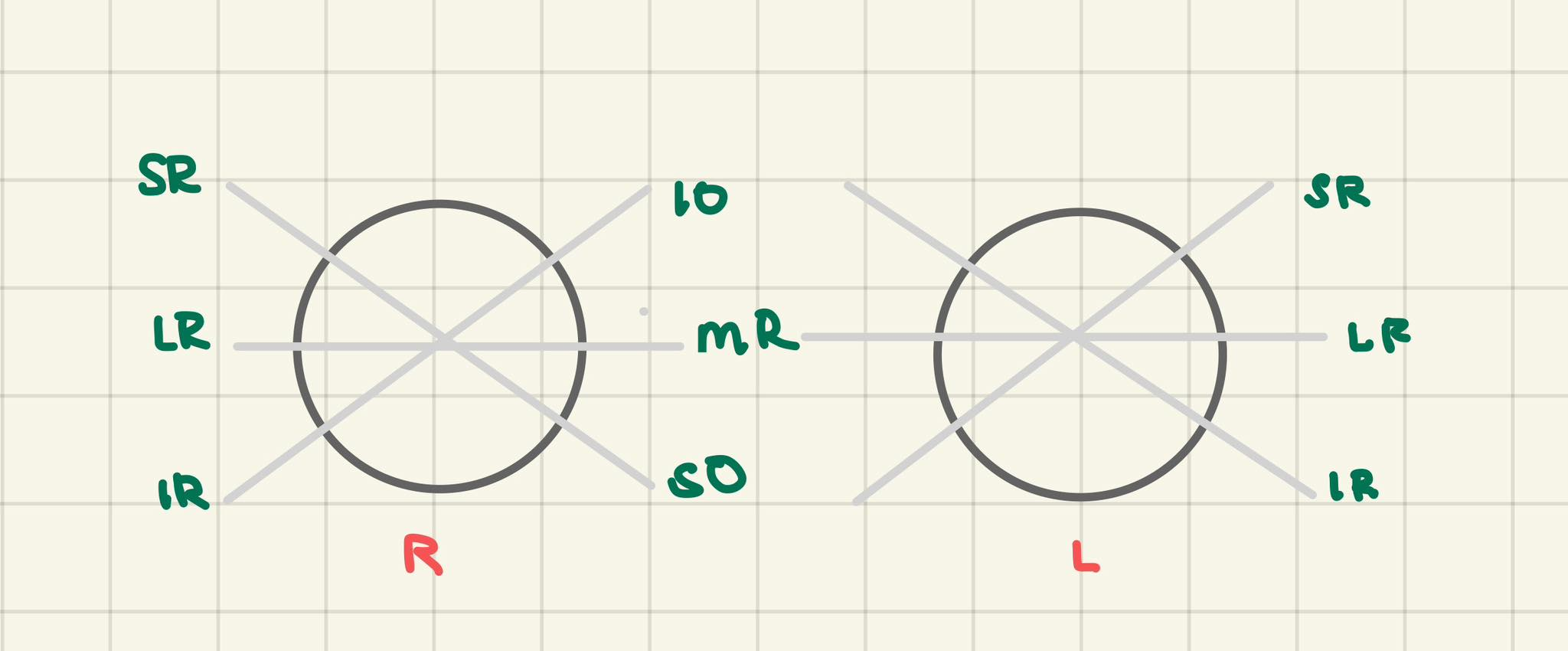
| ACTION | MUSCLES |
|---|---|
| look upward | R |
| L | Inferior ObliqueSuperior Rectus |
| look downward | R |
| L | Superior obliqueInferior rectus |
| looking to the right | R |
| L | medial rectus |
| looking to the left | R |
| L | lateral rectus |
| looking up to the right | R |
| L | Inferior oblique |
| looking up to the left | R |
| L | Superior rectus |
| looking down to the R | R |
| L | Superior Oblique |
| looking down to the L | R |
| L | Inferior Rectus |
Clinical Correlation
| Diplopia (CN 4 & 6) | Vertical 4Difficulty in descending stairshorizontal 6 (MC) IPSIX |
|---|---|
| Strabismus (CN 3 & 6) | Internal (Esotropia) - SixExternal (Exotropia) - Three |
| Patient complains of diplopia on looking to the rightR 4L 4R 6L 62. Pt complains of diplopia upon looking to the right and downR 4L 4R 6L 6Compensation to correct DiplopiaTilt: CN 4 (4 letters)Rotate CN 6 (6 letters |
|---|
CN 5: Trigeminal
- largest
- Gasserian/Semilunar Ganglion
- Tic Douloureux (Trigeminal Neuralgia)
- Mixed
Motor
- Muscles of Mastication
| Masseter | Closure of mouth |
|---|---|
| Medial Pterygoid | |
| Temporalis | |
| Lateral Pterygoid*2 heads pterygoids | opening of mouth |
- Additional muscles
- Digastric (Ant)
- Mylohyoid (belong to suprahyoid
- Tensor Tympani - Dampens sound
- Tensor Veli palatini
Sensory
- Facial Sensation
- 3 divisions
- V1 - Ophthalmic (most popular): sensory supply of eyeball
- V2 - Maxillary
- V3 - Mandibular
| Corneal Reflex: napuwingBlink ReflexAfferent 5V1Efferent 7Eye closure: CN 7Eye opening CN3*Bell’s palsy inability to close the affected eyeSneeze Reflexafferent 5V1efferent 9-10Sneeze reflex15910 |
|---|
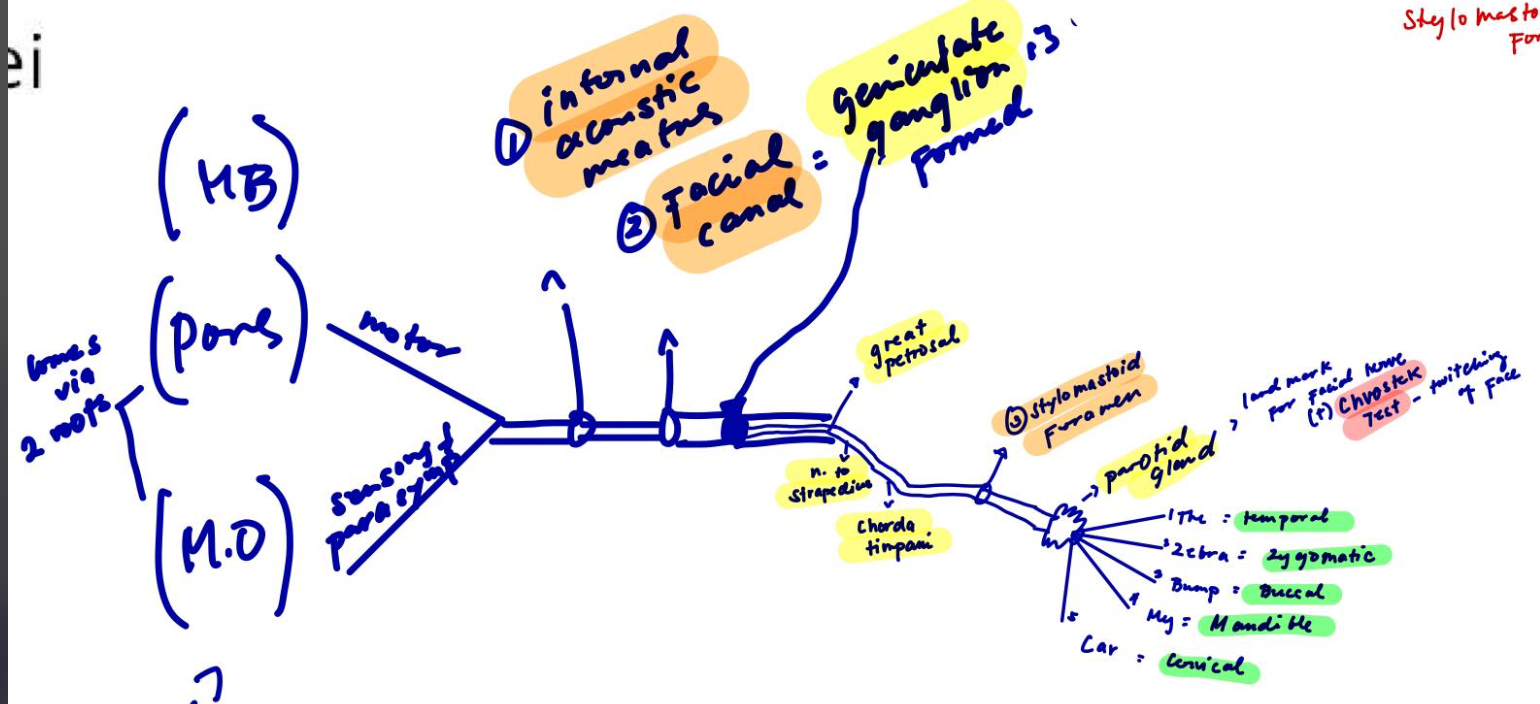
CN 7 - Facial Nerve
- Bell’s Palsy
- aka: Prosopoplegia refrigeration palsy
- Geniculate Ganglion
- genu = tuhod
- part of 1973, 1975, 1971 (vagal system)
- Mixed
MOTOR
- Ms of the facial expression
- Other ms:
- Digastric (posterior belly)
- Stylohyoid
- Stapedius
- smallest ms in the body (found in the ear)
- affected in “Hyperacusis” (↑’d sensitivity to sound; paralysis of stapedius ms)
Muscles of the Face
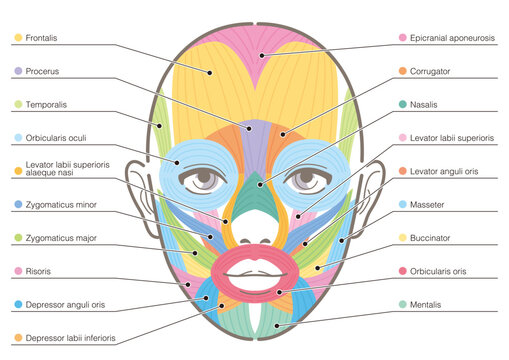
| Frowning | Corrugator Supercilli |
|---|---|
| Surprise | Occipito Frontalis |
| Smile | Zygomaticus Major |
| Grimace | Risorius |
| Doubt | Mentalis |
| Distaste | Procerus |
| Kissing | Orbicularis Oris |
| Winking | Orbicularis Oris |
| Sucking & Blowing | Buccinator |
| Sneering | Levator Anguli Oris |
| EGAD | Platysma |
EXIT POINTS:
SENSORY
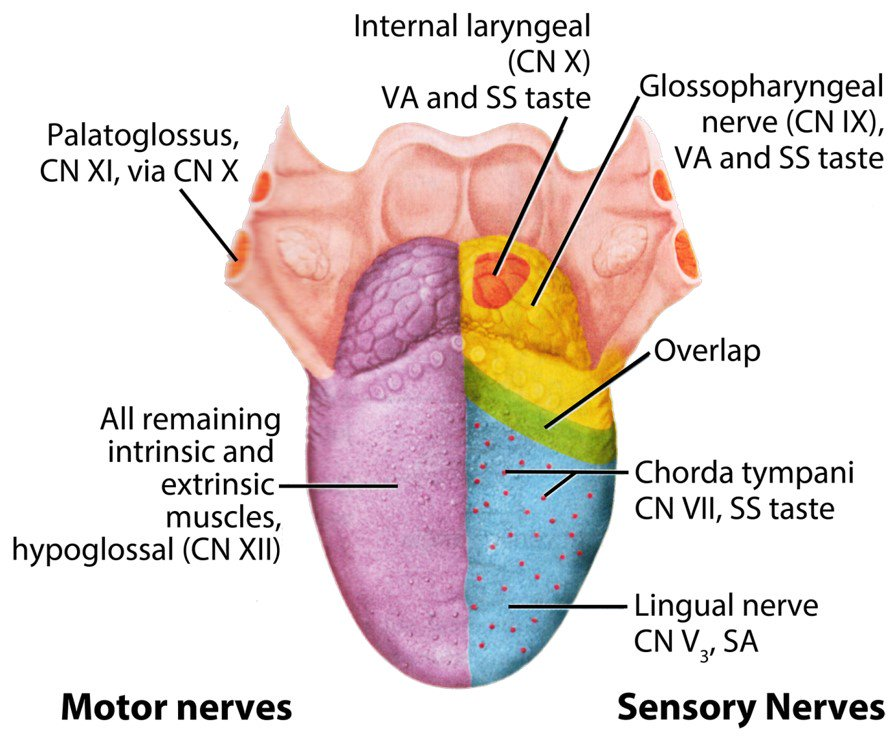
- C7: taste anterior ⅔ of tongue
- Chorda Timpani - fibers that provide taste sensation
- Ageusia - loss of taste sensation
- C9: general sensation & taste posterior ⅔ of tongue
- C5: general sensation (pain) anterior ⅔ of tongue
AUTONOMIC
- Salivary Glands
- Sublingual
- Submandibular
- Superior Salivary Mucus
- Lacrimal Glands
- Great Petrosal Branch
- Crocodile tears (during mouth movements)
Q1: Lesion CN 7 at the Stylomastoid Foramen will result to which of the following:Ans: Facial PalsyQ2: Bell’s Palsy vs. StrokeIpsilateral Facial Paralysis - Bell’s PalsyContralateral Lower Quadrant Facial Palsy - StrokeCorticobulbar Tract Involvement 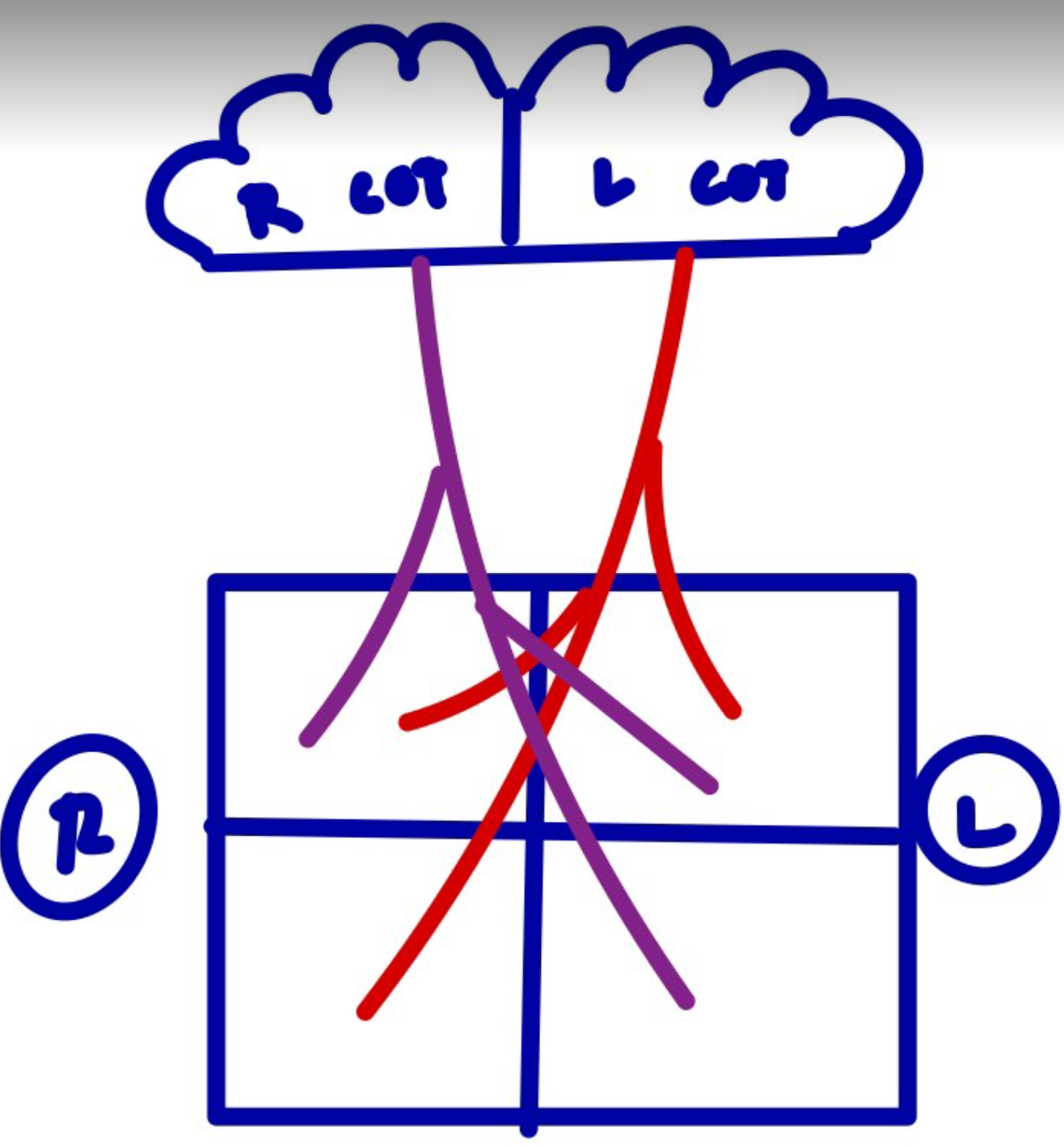 |
|---|
CN 8: VESTIBULOCOCHLEAR NERVE
- Meiner’s Disease
- 2 Parts:
- Vestibular
- Balance -> Vestibular apparatus
- Dysequilibrium
- Vertigo -> BPPV (Benign Paroxysmal Positional Vertigo)
- Cochlear
- Hearing -> Organ of Corti (true organ of hearing )
- Deafness
3 Types of Deafness
- Conduction - sound waves is impaired (outer & inner ear problem)
- Sensorineural - sensory fibers of CN 8 is involved (inner ear problem)
- Cortical - affected Brodmann’s Area 41
- primary area for hearing
- Heschl’s gyrus
Tuning Fork Test
- test for auditory acuity
- Weber’s Test
- tuning fork on vertex
- test for lateralization
- Rinne Test
- tuning fork on mastoid process
- compared tone conduction vs. air conduction
CN 9: GLOSSOPHARYNGEAL NERVE
- Mixed
MOTOR
- Stylophrayngeus muscle
SENSORY
- Taste & general sensation on posterior ⅓ of the tongue
AUTONOMIC
- Parotid Gland - interior salivatory glands
- Monitors carotid body & sinus
CN 10: VAGUS NERVE
- Longest cranial nerve
- 9 & 10 laging magkasama
MOTOR
- Muscles of pharynx
- Muscles of larynx
- voice box
- vocal cords
- phonation (phonaten)
- Dysphonia - different in sound production
- Aphonia - absence of sound production (pt with hoarse voice)
SENSORY
- Skin of pinna of external ear
- Sensation to pharynx, larynx, and epiglottis
AUTONOMIC
- Innervates visceral organs of the thorax & abdomen
- Thorax: heart (↓’d HR) & lungs (bronchodilation)
- Abdomen: stomach, liver, pancreas, small & large intestine
- 75% of parasympathetic nervous system
- GAG REFLEX
- swallowing reflex
- AFF: CAN 9
- EFF: CN 10
- absence results to dysphagia
- Put tongue depressor at the back of the tongue
| Q1: Innervates muscle of the pharynx:910bothNOTAQ2: Pt. has dysphagia. What CN is affected?910bothNOTAQ3: Pt. has dysphagia & dysphonia. What CN is affected?910bothNOTAQ4: You asked the px to say AHHH, the uvula deviated to the right. Where is the lesion?Ans: Right CN 10ST: AHH -. look at the movement of uvula (pull will always be on the stringer side) |
|---|
CN 11: SPINAL ACCESSORY
- Only CN through foramen magnum
- Affected in lateral winging of the scapula (sliding door paralysis)
- Affected in radical neck dissection (CN 11 is cut)
- 2 parts:
- Cranial Part
- part of vagal system
- innervates pharynx & larynx
- Spinal Part
- Innervates
- SCM (C2, C3)
- C3 = Side Flexion (ipsilateral side) & Rotation (contralateral)
- Trapezius (C3, C4)
- C4 = shoulder shrug
CN 12: HYPOGLOSSAL
- Innervates tongue ms (motor component)
- Dysarthria - difficulty in articulation (may affect CN 5, 7, 10)
Tongue Muscles
- Palatoglossus - tongue elevation
- supplied by the pharyngeal plexus (CN 9 & 10)
- Genioglossus - protrudes tongue forward
- Hyoglossus - tongue depression
- Styloglossus - curls tongue upward & backward
**Only genioglossus, hyoglossus, and styloglossus are innervated by CN 12
| Q: Upon tongue protrusion the tongue deviated to the right. Where is the lesion?Right CN 12Left CN 12**Tongue Deviation:**Upon tongue protrusion, tongue deviates to the R (affected CN 12)Rule:UMNL: C/L deviation LMNL: I/L deviationEx:R CVA = tongue deviates to RL Hemiplegia = tongue deviates to LNote: Tongue always deviate towards the weak side |
|---|