Human Physiology and Anatomy
Final Exam Study Guide
Spring 2024
Dr. Kuperschmidt
The majority of the examination is going to be Urinary and Reproductive Systems
Urinary System:
Basic Kidney anatomy, where it’s located, and general function in the U.S.
Renal Cortex and its inclusions
The kidneys lie on either side of the vertebral column in a depression high on the posterior wall of the abdominal cavity. Retroperitoneal. The upper and lower borders of the kidneys are generally at the levels of the twelfth thoracic and third lumbar vertebrae.
Main function of the kidneys is to regulate the volume and composition of body fluids, remove metabolic wastes, excess water, and electrolytes from the blood.
Help control the rate of red blood cell formation by secreting erythropoietin and regulate blood pressure by secreting the enzyme renin.
regulates absorption of calcium ions by activating vitamin D
The renal cortex- forms a shell around the medulla. It dips into the medulla between the renal pyramids creating the renal columns.
Anatomy of a Nephron and Renal Corpuscle
Nephrons- The functional units, about 1 million of them. Each nephron consists of a renal corpuscle and a renal tubule
Renal Corpuscle- part of the nephron that consists of a glomerulus and a glomerular capsule (bowman)
Macula densa- cells that secrete renin
glomerular + capsule= renal corpuscle
FILTRATION, REABSORPTION, SECRETION
Renal Medulla and its inclusions
All physiology that has to do with the pyramids, minor and major calyces, renal pelvis etc.
Renal Medulla- composed of conical masses of tissue called renal pyramids, Their bases orient toward the convex surface of the kidney, and their apexes form the renal papillae. The tissue of the medulla appears striated because it consists of microscopic tubules that lead from the cortex to the renal papillae.
Major calyces- 2-3 tubes that form the renal pelvis.
Minor calyces- 7-20. The minor renal calyces (minor calyx is singular) are described as small chambers of the kidneys, through which urine passes. Specifically, renal filtrate from the renal papilla drain into minor calyces, and into major calyces thereafter.
Renal Pelvis- located mostly inside the renal sinus and directs the urine formed by the kidney toward the ureter.
Pathway that the urine takes to get out of the kidney starting with Bowman’s capsule--------🡪 bladder
Nephron → glomerulus → bowman's capsule → proximal convoluted tubule → loop of henle → distal convoluted tubule → collecting duct → minor calyx → major calyx → renal pelvis → ureter → bladder
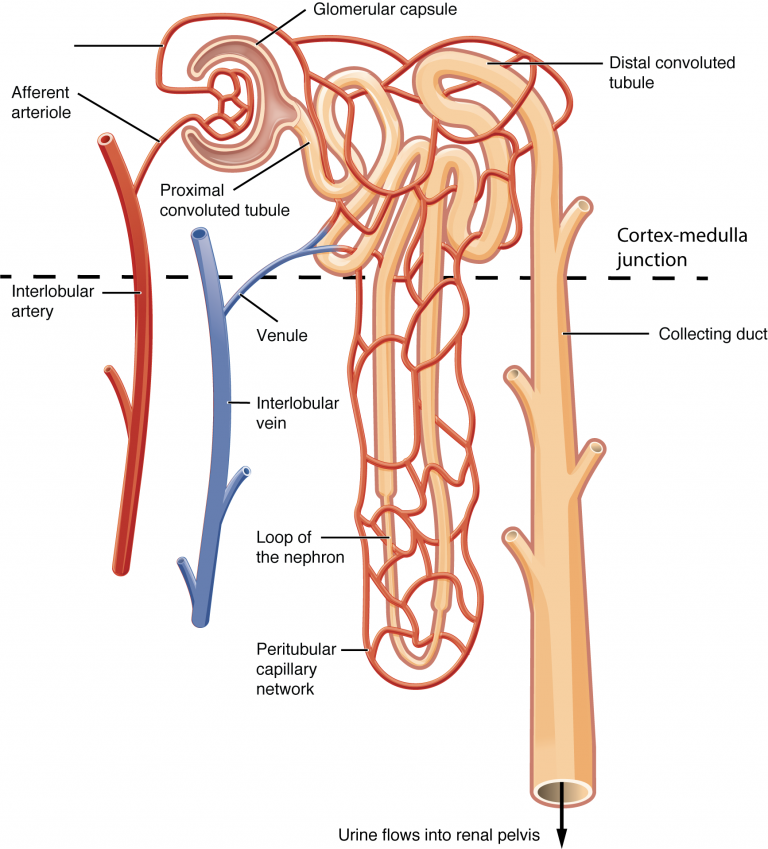
Be able to describe the anatomy of a glomerulus and its surrounding capsule and the pathway of blood through the glomerulus.
glomerulus- A filtering unit of composed tangled cluster of blood capillaries and a surrounding thin- walled, sac like structure called a glomerular capsule.
An afferent arteriole gives rise to these capillaries which then lead to an effective arteriole.
Filtration of fluid from glomerular capillaries is the first step in urine formation. A capsule is an expansion at the end of a renal tubule that receives the fluid filtered at the glomerulus.
Know also the functions of the DCT, Loop of Henle, PCT, collecting ducts, renal papillae and pelvis
DCT- merge in the renal cortex to form a collecting duct, which is technically not part of any one nephron. regulation of potassium, sodium, calcium, and pH. It is the primary site for the kidneys' hormone-based regulation of calcium (Ca).
Loop of Henle- The main function of Henle's loop is to reabsorb water and important nutrients in the filtrate. Through the countercurrent mechanism, it aims to reduce the volume of water and solutes within the urine without any change in its concentration.
PCT- reabsorbing approximately 65% of filtered load and most, if not all, of filtered amino acids, glucose, solutes, and low molecular weight proteins. Proximal tubules also play a key role in regulating acid-base balance by reabsorbing approximately 80% of filtered bicarbonate.
Collecting Ducts- passes into the renal medulla, widening as it is joined by other collecting ducts.
Collecting tubule : This is the pathway that urine exits the nephron and eventually leads
to the renal pelvis
Renal Papillae- project into each minor calyx from the renal medulla, carry renal filtrate from the papillary ducts to the minor calyces of the renal pelvis via papillary ducts.
Renal Pelvis- The kidney pelvis acts like a funnel, collecting the urine produced in the kidney and leading to a central “stem,” the ureter.
Components of Urine… What is included in the filtrate? Please know what is not supposed to be in the urine
glomerular filtration + tubular secretion - tubular reabsorption= urine
Waste- Uric acid, urea, glucose, creatinine
sodium, potassium, calcium, magnesium, chloride, bicarbonate, sulfate, phosphate
Glomerulonephritis- What is it and what would you see with a patient with it?
Renal disorder where plasma proteins enter the urine because of increased permeability of the glomerular membranes.
because glomeruli have been infected by bacteria- holes get bigger and things can escape through blood -proteins and sugar
urine is infection
urinalysis can confirm what you have jaundice and foamy/discolored urine 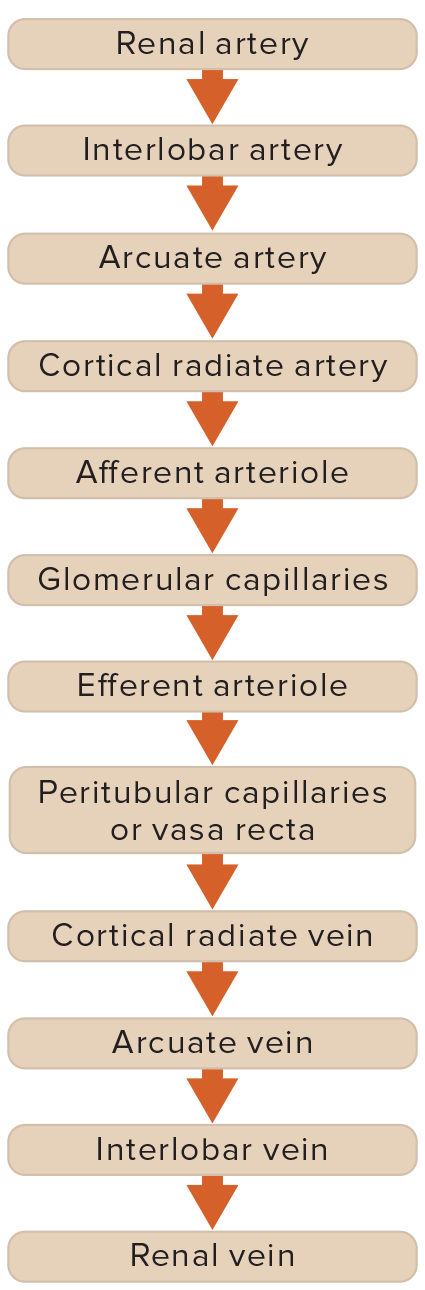
Structure of the Ureters and Urinary Bladder
Renal Calculi
Events of Micturition
Ureters- bring urine to the urinary bladder
Urinary Bladder- where the urine exits the body
Renal calculi- kidney stones
Micturition- fancy term for peeing- dont need to know events
Reproductive System
Female Anatomy
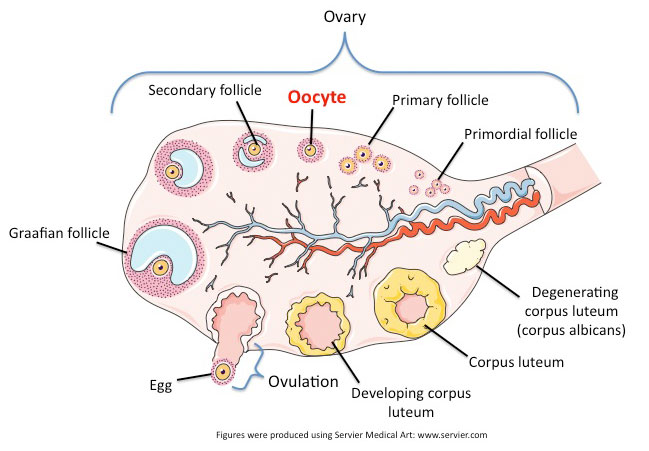
Development of a primordial follicle within the ovary
Know the different stages of follicles, actions of FSH and LH on the ovary
Features of a mature follicle (antrum, zona pellucida, corona radiata)
During prenatal development, small groups of cells in the
outer cortex form millions of primordial follicles
each consists of a single primary oocyte surrounded by
follicular cells
In early development, the primary oocytes undergo
meiosis and it halts until puberty
Of the several million formed originally, only a million or
so remain at the time of birth and 400,000 are present
at puberty
Of those, probably 400 to 500 will be released during the
reproductive life of a female
Fewer than 10 will go on to form a new individual!!!!
Maturation
At puberty, the anterior pituitary gland secretes
follicle stimulating hormone and the ovaries
enlarge
The primordial follicles begin to mature by:
i) oocytes enlarge
ii) a layer of glycoprotein, the zona pellucida
gradually separates the oocyte from the
granulosa cells and it turns into a primary
follicle
Meanwhile, the ovarian cells outside the follicle
become organized into an inner layer called the
theca interna (vascular) and an outer fibrous
layer called the theca externa
Follicle continues to proliferate to many layers and
a fluid filled cavity (antrum) appears between
them and starts to enlarge
Once a certain size, the follicle is called a mature or
Graafian follicle, it will outgrow the others during
a normal ovulation cycle
It will erupt and the others will degenerate/cycle
Follicle is only a follicle until it's ovulated (day 14 is last day of follicle)
starts as a oocyte and then turns into a follicle
each follicle contains an egg and produces estrogen
dominant follicle will grow faster than others, as it grows, estrogen rises → inhibits the secretion of the follicle- stimulating hormone
follicular phase- day 1
estrogen and progesterone are low
inner lining sheds- menstruate
follicle will release its egg and head toward the fallopian tube to uterus
Corona radiata- layer that consists of follicular cells that adhere to the secondary oocytes surface.
Hormone Cycle ( which hormones are causing what events to occur in the ovary and uterus)
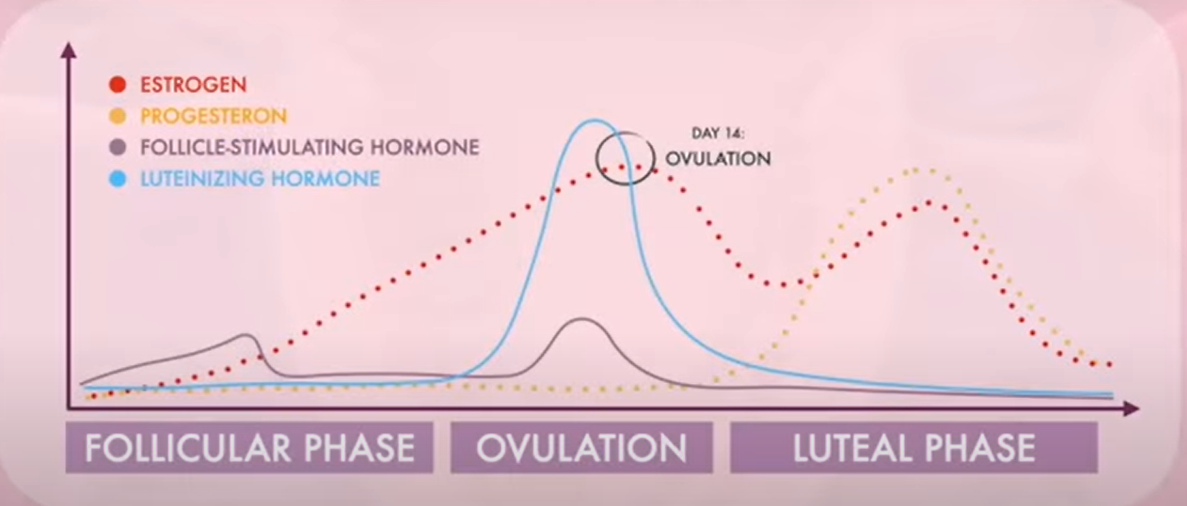
estrogen inhibit LH and FSH during most of the reproductive cycle
granulosa cells secrete estrogens
effects of estrogen
development of breasts and ductile system of the mammary glands
increased adipose tissue in breasts, thighs, and buttocks
increases vascularization of skin
estrogens c ause uterine lining to thicken
FSH stimulates follicle maturation
LH surge released which stimulates ovulation
stimulates the interstitial cells to produce male sex hormones
ovulation occurs when LH and FSH induced interactions which weaken the antral follicle and release the secondary oocyte- completes meiosis 1
Progesterone- secreted by the ovaries, affects cyclical changes in the uterus and mammary glands
Uterine Cycle ( What are the changes that are happening to the lining of the uterus)
Proliferative phase- increasing concentrations of estrogen during the first week or so of a menstrual cycle changes the lining, thickening the glandular endometrium
day 1-14
Secretory phase- Progesterone causes endometrium to become more vascular and glandular. stimulation of the uterine glands secretes more glycogen and lipids
14-28
Ovulation- weakening and rupturing of the bulging follicular wall, this event sends the secondary oocyte and follicular fluid out of the ovary.
14- can last a couple days
(importance of keeping up the corpus luteum?)
Secretes progesterone to thicken the lining for plantation to take place
Menstruation when the corpus luteum ceases to function, concentrations of estrogens and progesterone rapidly decline and in response, blood vessels in the endometrium constrict. this reduces supply of oxygen and nutrients to the thickened endometrium, and the lining slough off,
Begins 28th day of the cycle- lasts about 3-5 days.
****KNOW SPECIFIC DAYS OF THE CYCLES****
Painful menses? (wink)
Endometriosis
-cause of female infertility
- inner lining of the uterus grows in the abdominal cavity- may happen if small pieces of endometrium move up through the uterine tubes during menses and implant in the abdominal cavity.
- when tissue begins to break down at the end of the cycle, it cannot be expelled to the outside, material remains in the cavity where it may irritate the peritoneum and cause pain.
Pathway to fertilization of the secondary oocyte
sperm cell reaches corona radiata of egg
acrosome of sperm cell releases enzymes that helps to break down the zona
pellucida
sperm cell’s membrane fuses with egg cell’s membrane
This union will prevent another sperm from penetrating
Pre-embryonic events of the fertilized egg including the following terminology:
Zygote, cleavage, morula, blastocyst, inner cell mass, trophoblast, primitive streak, blastodisc
zygote: union of egg
and sperm
blastomeres: individual cells formed during cleavage
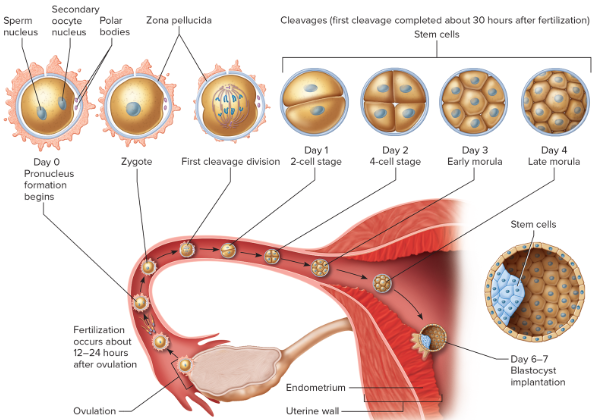
morula: after 3 days, a solid ball of cells is visible
fertilized ovum
12-24 hours after ovulation
zygote forms
cleavage
30 hours to third day
mitosis increases cell number
morula
third to fourth day
solid ball of cells
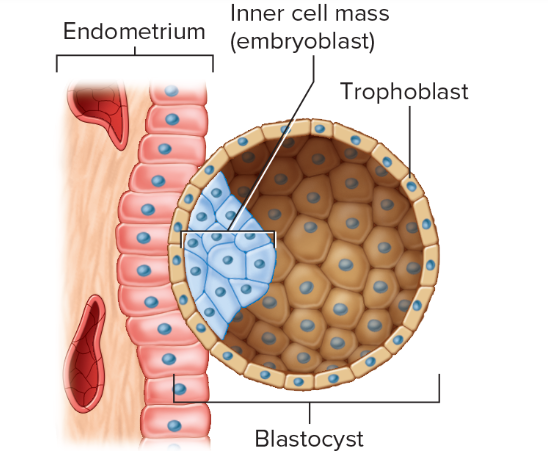
blastocyst- fifth day through second
week
trophoblast and inner cell mass form hollow ball of cells
gastrula- end of second week primary germ layers form’
Inner cell mass- cells in one region group to form an inner cell mass that eventually fives rise to the embryo proper
Primitive streak- lateral spine view
Blastodisc- The blastodisc, also called the germinal disc, is the embryo-forming part on the yolk of the egg of an animal that undergoes discoidal meroblastic cleavage.
Events of Gastrulation: Formation of the 3 embryonic germ layers
Gastrulation- movement of cells within the embryonic disc to form multiple layers, By the end of the second week the embryonic disc consists of two distinct layers: an outer ectoderm and inner endoderm. Through gastrulation, the mesoderm forms between them → these create the primary germ layers of the primordial embryo- at this point the embryo is termed gastrula.
Endoderm- The innermost of the three primary germ layers in the very early embryo.
Mesoderm- the middle developmental layer between the ectoderm and endoderm, which gives rise to the skeleton, muscle, heart and bones.
Ectoderm- The surface ectoderm will give rise to the epidermis, external glands, hair, nails, anterior pituitary, and the apical ectodermal ridge amongst others. The functions of the surface ectoderm include hormone regulation by the adenohypophysis, acting as a barrier against the external involvement, and homeostasis.
What organ systems are derived from all 3 layers? Know em!!!
endoderm- digestive
mesoderm- muscular kidneys and heart
ectoderm- central and peripheral nervous system
endocrine comes from all 3
Know the extraembryonic membranes surrounding the growing embryo and their functions.
Amnion- develops around the embryo proper, appears during the second week
its margin is attached around the edge of the flattened inner cell mass/ embryonic disc
amniotic fluid fills the space between the amnion and the disc
fluid provides a watery environment in which the embryo can grow freely without being compressed by other tissues
protects the embryo from movements, maintains stable temperature and fetal development
amnion envelopes the tissues on the underside of the embryo
Chorion- The chorion and the amnion make up the fetal sac that surrounds and protects a developing embryo. The chorion develops into the fetal placenta and is responsible for the exchange of blood, gasses, and waste products between the maternal and fetal blood.
Yolk sac- Before the placenta forms and can take over, the yolk sac provides nutrition and gas exchange between the mother and the developing embryo. It is also the main organ of embryonic blood cell production via blood islands near the yolk sac.
forms blood cells in the early stages of development and gives rise to the cells that will become sex cells
Allantois- The allantois has two important functions regardless of the embryo that it is a part of. It is responsible for gas exchange - that is, oxygen in, carbon dioxide out. It is also responsible for the liquid waste from the embryo, basically nitrogenous urine waste.
Fetal structures:
Formation of the Placenta ( all that goes into making this structure)
Be able to know how the baby and mommy work together using the connections between them.
Umbilical cord- connects the fetus to the placenta
suspends the embryo in the amniotic cavity
begins to form from structures in the connecting stalk.
Placenta- The placental membrane consists of the epithelial wall of an embryonic capillary
epithelial wall of a chorionic villus
Consists of an embryonic portion and a maternal portion
vasculature inside the cord-
Umbilical arteries 2 arteries (blue) take waste in blood back to mom's heart
Umbilical vein- 1 of them, red, takes blood away from mom's heart and into babies
All other hormones are involved during pregnancy and delivery.
Progesterone- synthesizes cholesterol in the maternal blood
PTH- maintains calcium concentrations in blood
Estrogens- created by corpus luteum, placenta secretes stimulate and maintain uterine lining, inhibit FSH and LH, enlarge reproductive organs.
during pregnancy: stimulates development of alveolar glands
cause ductile systems to grow
Human placental lactogen- initiates milk production, stimulates breast development
Oxytocin- keeps contractions going
Prolactin- prolactin is synthesized from early pregnancy from early pregnancy throughout gestation, peaking at the time of birth.
Relaxin- from corpus luteum inhibits uterine contractions and relaxes pelvic ligaments
FSH- activates menstrual cycle when a woman stops breastfeeding.
LH- maintains the corpus luteum
hCG- helps prevent spontaneous abortion, maintains pregnancy
can be detected in urination
****KNOW THEIR ROLES IN THE BIG PICTURE OF THINGS!
What are the three stages of Labor?
Dilation stage- mom gets first contraction- 10 cm and mom can start pushing
oxytocin will keep the contractions going
expulsion stage- when baby is out
placental stage- birth the placenta
placenta previa- can block the baby if placenta precedes baby
lighting- baby falls into place (head first)
breech birth- feet first birth
Male Reproductive System: Know basic anatomy of the following
Testes and associated structures
gonads are outside
testes produce sperm cells
can produce until 70-80 years old
tiny tubes- seminiferous tubules
Sperm production and the associated glands that enhance/nourish spermatozoa ( prostate, bulbourethral glands, seminal vesicle, ejaculatory duct, epididymis)
sperm has 3 parts to it - head body and tail
acrosome- head has an enzyme (hyaluronidase) that breaks down the zona pellucida and fuses with the egg
Have mitochondria - powers themselves
2 tailed sperm- baby will not survive
journey out of male and into female
epididymis- coiled tube, connection to the outside, place where sperm will mature
where the maturation of the sperm happens, tightly coiled tubes connected to ducts within the testis
vas deferens- sperm cell will come out of testes and into the prostate gland
prostate gland- sits near urethra
secretes acidic for movement (where its hard to get through)
seminal vesicle- secretes slightly alkaline fluid that helps regulate ph
i) also secretes fructose for energy
ii) prostaglandins: which stimulates muscular contractions within the female, aiding movement of sperm
sperm start out handicapped- capacitation will make non motile sperm to motile- vas deferens
Bulbourethral glands- bulbourethral glands (Cowper’s glands): secrete a
mucus-like fluid in response to sexual stimulation and
lubricates the penis for coitus
Extra notes-
corona radiata- small surface layer that consists of follicular cells on the secondary oocyte
Corona pellucida- the membrane of secondary oocyte rich in glyco proteins and the layer closest to the oocytes cell membrane
cleavage- divisions of the zygote into a ball of progressively smaller cells
resulting cells are blastomeres
morula- about 16 cells that have moved down to the uterine tubes to the uterine cavity
remains unattached for 3 days
THEN
cell division continues and ball of cells hollow out → zona pellucida of secondary oocyte degenerates → hollow structure is now called a blastocyst (early stage of prenatal development when the embryo is a hollow ball of cells)
THEN
the blastocyst implants intself and the trophoblast will invade the endometrium
inner cell mass will eventually give rise to the embryo proper - the body of the developing offspring
trophoblast develops into structures that assist the development of the embryo proper
secretes hCG which maintains the corpus lithium during the early strages of pregnancy and keeps immune system from rejecting the blastocyt
THEN
a second layer of cells begins to line the trophoblast, and together these two layers form a structure called the chorion, the outermost extraembryonic membrane,
→ projections form out called chorionic villi which erode their way into the endometrium
lacunae- continued secretion of proteolytic enzymes (the ones thar help implantation) form irregular spaces around and between the villi. , these spaces fill with maternal blood- allow nutrient exchange from cappilaries to mother to baby
\THEN
a second membrane (amnion) devekops around the embryo proper (appears 2nd week)
its margin is attached around the edge of the flattened inner cell mass (Embryonic disc)
amniotic fluid then fills the cavity and provides watery environment
menstruation- 28-4
proliferative 1-14- follicle is maturing
secretory- 14-28 - lining is getting very thick