LABOR AND BIRTH
Objectives
Five Major Factors Affecting the Labor Process:
Identify and explain the five major factors: Powers, Passageway, Passenger, Psyche, and Position of the mother.
Fetal Head Characteristics During Labor:
Understand how the size and position of the fetal head influence the labor and birth process.
Maternal Adaptations to Labor:
Examine the maternal anatomical and physiological changes that occur during labor.
Onset of Labor Factors:
Describe factors contributing to the onset of labor.
Stages of Labor and Related Care:
Describe the four stages of labor including nursing and medical care associated with each stage.
Mechanism of Spontaneous Vaginal Delivery:
Explain the mechanism of spontaneous vaginal delivery and associated nursing care.
Onset of Labor
Maternal Factors Influencing Onset:
Pressure on the cervix.
Hormonal changes occurring within the body.
Estrogen increases which enhances uterine myometrium to produce contractions and opens cervical os
Uterine muscles stretched leading to release of Prostaglandins which initiate
Contractions initiating labor.
Typical timing for most women: between 38 and 42 weeks of gestation.
Increased excitability of the uterus and cervical softening.
labor by softening cervix and stimulating contractions
Oxytocin soften cervix and stimulates contractions
Progesterone decreases (progesterone was maintaining pregnancy)
Fetal Factors Influencing Onset:
Contributions from the placenta.
Release of prostaglandins.
Production of fetal cortisol affecting uterine contractions.
Signs of Impending Labor
Physical Indicators:
Lightening (engagement of the fetus).
uterus sinks downwards and forward about 2 wks before birth for primips.
Fetal head or presenting part descends into true pelvis. Less pressure on ribcage (breathe more easily), but more pressure on bladder (urinary freq). Multips may occur when labor occurs.
Presence of Braxton Hicks contractions (practice contractions).
frequent, irregular contractions (body getting prepared)
Vaginal mucous more profuse and may pass mucous plug 1-2 wks before delivery, as cervix thins or opens slightly. Bloody show from vessels rupturing as cervix thins and dilates.
Surge in energy often referred to as 'nesting'.
Gastrointestinal changes may occur.
Backaches and discomfort in the sacroiliac region.
Specific Signs to Observe:
Profuse vaginal and cervical mucus.
Bloody show indicating cervical change.
Weight loss of 1-3 lbs, a common occurrence as labor approaches.
Spontaneous rupture of membranes (SROM).
True vs. False Labor:
Understanding the difference and how a nurse might determine which type of labor is occurring.
True labor: contractions get longer, stronger, and closer together. Does not go away with change in activity or hydration.
Onset of Labor
Assessment of Rupture of Membranes (ROM)
SROM- Spontaneous
AROM- Amniotomy
Techniques to Confirm Rupture of Membranes (ROM)
Diagnostic Methods:
Speculum examination to visualize cervical membranes.
Use of Nitrazine paper to test pH.
Ferning test for amniotic fluid.
AmniSure testing kit for further confirmation of ROM.
monoclonal immunoassay that detects placental alph macroglobulin-1 an amniotic protein in vaginal secretions if water broken.
Nursing Actions: Assess amount, color, odor, FHR, Temp q 2 hours after ROM
Factors Affecting Labor
The Five P's of Labor:
Powers:
Contractions and maternal pushing efforts.
Passageway:
Anatomy of the pelvis and birth canal.
Passenger:
Characteristics of the fetus, including size and position.
Psyche:
Psychological aspects influencing the labor experience.
Position:
Maternal position can greatly impact physiological and anatomical adaptation during labor.
Cervical Dilation Chart
Visualization of Cervical Dilation (cm):
1 cm: Cheerios
2 cm: Grape
3 cm: Banana slice
4 cm: Cracker
5 cm: Lime slice
6 cm: Cookie
7 cm: Orange slice
8 cm: Halved apple
9 cm: Donut
10 cm: Cantaloupe melon
Primary Powers:
Action of contractions includes:
contractions originate from pacemaker points in uterine muscle segments, moving downwards in waves.
Effacement: Shortening and thinning of the cervix. normally 2-3cm long and 1cm thick.
Dilation: Enlargement or widening of the cervix.
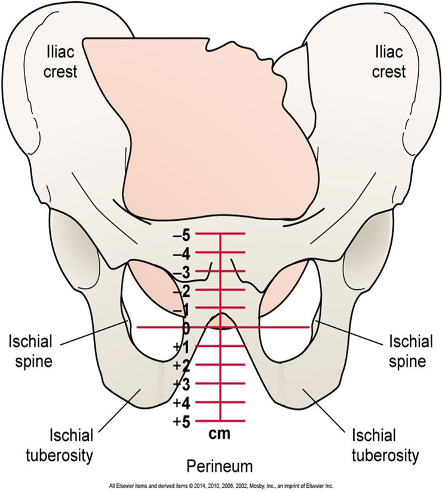
Station: decent of fetus toward introitus
negative is above ischial spines (negative that baby will be delivered soon), zero is at the ischial spines, positives are below ischial spine (positive sign that baby is coming out).
Secondary Powers:
Bearing down and pushing efforts of the mother.
Sterile Vaginal Examination (SVE)
Purpose and Findings:
Status of amniotic membranes. (intact, bulging)
Status of the cervix. (soft, firm, anterior or posterior)
Dilation measurements (0 cm to 10 cm).
Effacement (0% long/thick to 100%).
Fetal station: descent of the presenting part. negative is above ischial spines, zero at spines, and positives are below ischial spines
Fetal presentation: cephalic, breech, or shoulders.
Fetal position: left, right, anterior, posterior, transverse
Engagement of the presenting part.
Cautions and Contraindications:
Caution: Only perform SVE when indicated, as there’s a risk of infection.
Common times for SVE include: Upon admission, before administering medications, significant changes in contractions or FHR, when pressure complaints arise.
Contraindications:
SVE should not be performed in cases of placenta previa, abruptio placentae, and preterm premature rupture of membranes (PPROM).
Passageway (2nd P)
Components of the Passageway:
Bony pelvis. True lies below the pelvic brim, consists of the pelvic inlet, midpelvis, and pelvis outlet
False pelvis- is the shallow portion above the pelvic brim- supports the abdominal viscera, upper portion supports gravid uterus and directs presenting part into true pelvis
True pelvis- lower pelvis outlet, dimensions must be large enough to accommodate fetus for birth.
Midpelvis (narrowest portion) should be at least 11.5cm for positive outcome
Cervix.
Pelvic floor muscles.
Vagina.
Introitus (external opening to the vagina).
Pelvic Classifications
Four categories:
Gynecoid: Ideal for labor. classic female pelvis (round-oval laterally), usually OA position (50%)
Anthropoid: Adequate for labor. oval shaped- wider anteroposterior (oval deep), OP position (24%)
Platypelloid (flat): Not ideal. flat pelvis (flat shallow), transverse and arrest of delivery, fetus usually transverse (3%)
Android: Usually inadequate for labor. classic male pelvis (heart), high risk CPD, laterally more narrow with more bony prominences (23%)
Passenger (3rd P)
Factors Concerning the Passenger:
Size of the fetal head.
Fetal presentation: Cephalic (head first 97%, can include face or brow which are abnormal), breech (buttocks or feet), or shoulder (less than 1%) presentations.
Fetal lie: Relationship of the fetus's long axis to that of the mother (longitudinal: correct vertical position, transverse: across abdomen, horizontal, oblique: diagonal).
Fetal attitude: Degree of flexion or extension of the fetus's limbs and head.
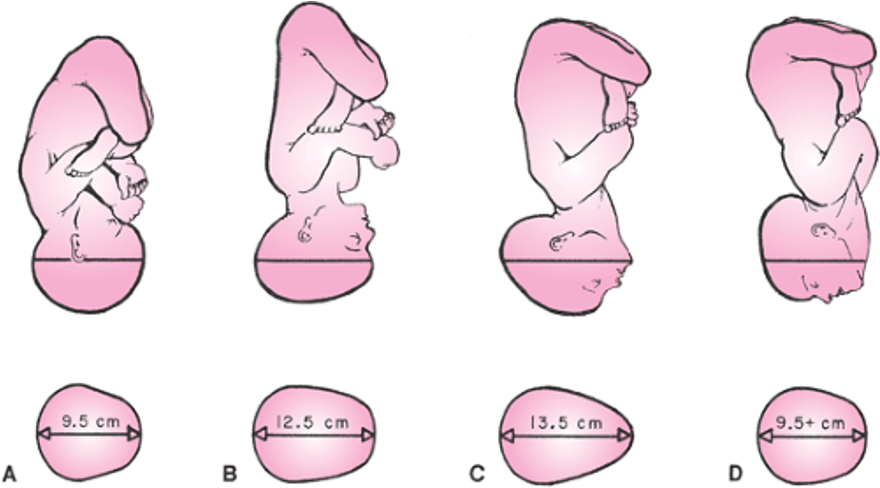
(A) Complete flexion: This is normal attitude in cephalic presentation. There is complete flexion of head with "chin on chest." This allows smallest cephalic diameter to enter pelvis, which gives fewest problems with descent and delivery.
(B) Moderate extension/deflexed: In cephalic presentation, fetal head is not flexed. Gives appearance of military person at attention. A larger diameter of head coming through passageway.
(C) Marked extension: Fetal head is extended or bent backwards. Also called a brow presentation. It is difficult to deliver because widest diameter of head enters pelvis first. May require a C/S if attitude cannot be changed.
(D) Hyperextension: Fetal head is extended all the way back. Also called face presentation. If there is adequate room in pelvis, fetus may be delivered vaginally.
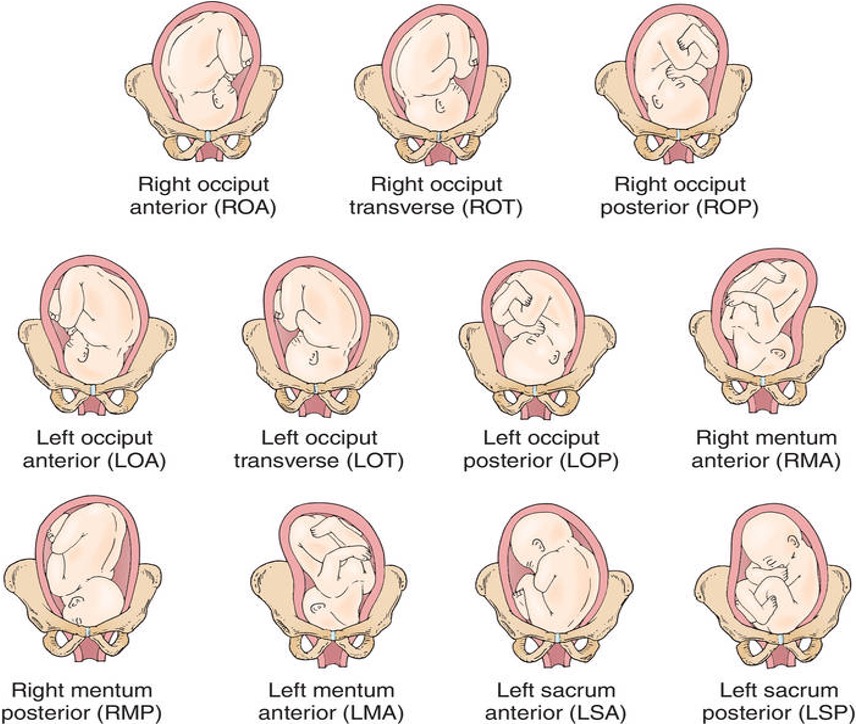
Fetal position: Orientation of the presenting part in relation to the maternal pelvis.
First letter - Right (R) or left (L) side of maternal pelvis
Second Letter- fetal presenting part: occiput (O); mentum (M), sacrum (S), or scapula (Sc)
Third Letter - Anterior (A), posterior (P), or transverse (T )
Psyche (4th P)
Influences on the Labor Process:
Psychosocial aspects of the individual. Anxiety and fear can interfere with labor, perception of pain
Preparation for labor and childbirth.
Coping mechanisms employed by the mother. Self-esteem, self-confidence, relationship to others, general life view
Cultural considerations and equity in care. beliefs, cultural needs, concerns. Equity of care for all cultures, races, and across gender spectrums.
Maternal expectations regarding labor. Past experiences, current pregnancy experience, adolescents
Support systems available to the laboring woman. Information, emotional support, comfort measures, advocacy
Position (5th P)
Influence of Maternal Position:
Affects the mother’s anatomical and physiological adaptations during labor. Frequent position changes during labor enhance maternal comfort and promote optimal fetal positioning.
Frequent changes in position can help:
Relieve fatigue.
Increase comfort.
Improve circulation.
Concerns Requiring Evaluation
Specific conditions that necessitate further evaluation include:
Unusual membrane ruptures.
Intense pain from contractions being longer, stronger, or closer together.
Marked increase in bloody show.
Significant decrease in fetal movement.
Severe headache, blurred vision, epigastric pain, or other drastic changes in maternal condition.
Stages and Phases of Labor
First Stage: 0 to 10 cm dilation
Latent Phase: 0-5 cm dilation, mild to moderate contractions.
Frequency: 2-5 minutes.
Duration: 30-40 seconds progressing to 40-60 seconds.
Average dilation for Nulliparas: 1 cm/hour, for Multiparas: 1.5 cm/hour.
Excited to be in labor, talkative, able to talk & walk through contractions, progressing to apprehensive, anxious, less social, focused on breathing, may need more support
Active Phase: 6-10 cm dilation, 100% effaced.
Contraction strength: Moderate to strong.
Frequency: 2-3 minutes.
Duration: 60-90 seconds.
Change in mood and appearance, irritable, frustrated, restless, want to give up, rectal pressure, nausea/vomiting, shaking
Second Stage: 10 cm to birth
Descent of fetal head with strong contractions occurring every 1-3 minutes, may feel out of control. +2 to +5 station.
Nursing actions: encouragement and assist patient to push with contractions
Ferguson’s reflex may cause involuntary pushing.
Crowning: can see the top of the head
Delivery of infant: nurse notes time
Third Stage: From the birth of the baby to the delivery of the placenta
Duration: Typically 5-10 minutes.
Signs include lengthening of the umbilical cord and descent of the placenta through the vagina.
Schultze mechanism: Shiny, fetal side of placenta presents first
Most common “shiny Schultz”
Duncan mechanism: Placenta separates from outer margin inward, roll up, and presents sideways
Placental surface is rough, commonly called “dirty Duncan”
Fourth Stage: Postpartum recovery
Monitoring and assessments conducted 1-4 hours after birth, including observation of normal blood loss in vaginal delivery (250-500 ml).
Fundus contracted down and firm, at midline
Assess vital signs, fundus, bladder, lochia, perineum every 15 minutes for the 1st hour, 30 min x 2
Lacerations
First degree
Perineal skin and vaginal mucous membrane
Second degree
Skin, mucous membrane, and fascia
Third degree
Skin, mucous membrane, muscle, and extends to rectal sphincter
Fourth degree
Extends into rectal mucosa
Pain Management in Labor
Nonpharmacologic Pain Management Techniques:
Childbirth preparation methods.
Childbirth education: popular in the US (Lamaze- psychoprophylaxis and Bradley- coached method)
Relaxation and breathing techniques including focusing and visualization.
Reduce tension and stress by focusing and relaxation techniques, imagery is focusing attention on pleasant scene or visualizing a favorite place
Breathing can promote oxygenation to mother and fetus as well as relaxation of abdominal muscles, genital muscles relax and do not interfere with descent.
Breathing technique: Cleansing breath: Begin and end contraction with deep cleansing breath. Paced breathing: slow-paced (IN-2-3-4 OUT-2-3-4; 6-8 breaths per min), modified-pace (IN-OUT, IN-OUT, IN-OUT/HEE-HEE-HEE-HEE; 32-40 breaths per min), and patterned pace (pant-blow; HEE-HEE-HEE-HOO).
Massage, effleurage, or counterpressure to provide comfort.
Effleurage: light massage or stroking of abdomen. Rhythmetic and distraction
Counterpressure: steady pressure to sacral area, effective for OP position/back labor. Can use tennis ball or fist of hand.
Applications of heat or cold, acupuncture, or acupressure.
Acupressure with heel of hand, fist, pads of fingers or tennis ball. Acupuncture is insertion of fine needles into specific areas to restore flow of qi (energy) and decrease pain
Hydrotherapy and utilizing different positions.
Water therapy: bathing, showering, whirlpool with warm water. Hydrotherapy- submerge in warm water to decrease anxiety and pain
Water block: injection of small amt of sterile water into lower back to relieve lower back pain
Aromatherapy and labor support.
Aromatherapy: essential oils to promote health, decrease stress, and relieve pain sensation (jasmine, geranium, rose, clary sage, ylang ylang, lavender)
Music: for distraction, increase spirits, and relax
Pharmacologic Pain Management Options:
Sedatives: relieve anxiety and induce sleep. Used mainly for prolonged early phase.
Opioids:
Administered IV or IM to provide sedation and pain relief during early labor.
Caution as opioids can decrease fetal heart rate, blood pressure, and respiratory rate which can affect fetus oxygenation.
VS and EFM should be treatment intervention with use.
Medication Alert: Opioid agonist-antagonist Nalbuphine (Nubain) and opioid antagonist Naloxone (Narcan) should be avoided in opioid-dependent women.
Opioid (narcotic) agonist analgesics: Meperidine hydrochloride (Demerol), Fentanyl citrate (Sublimaze), Butorphanol tartrate (Stadol)
narcotics that stimulate opioid receptors. Feeling of well-being or euphoria to rest between contractions. Should not be used until contractions well established or could inhibit uterine contractions. Can cause CNS and resp depression, hypoventilation, and oxygen desaturation to mother and neonate. Can cause n/v.
Opioid (narcotic) agonist–antagonist analgesics: Nalbuphine hydrochloride (Nubain)
these mixed opioids provide adequate relief without respiratory depression in mother and neonate. Less likely to cause nausea/vomiting. Do not give to opioid dependent woman bc can precipitate withdrawal symptoms in both mother and newborn bc it is opioid antagonist.
Opioid Antagonist: Narcan is reversal for CNS and resp depression in either mother or newborn. Do not give to opioid dependent woman can cause withdrawal.
Opioid (narcotic) antagonists: Naloxone hydrochloride (Narcan)
Narcan is reversal for CNS and resp depression in either mother or newborn. Do not give to opioid dependent woman can cause withdrawal.
Nitrous Oxide:
Intermittent inhalation of nitrous oxide dulls perception of pain & anxiety. Provides quick relief lasting 2-5 minutes; promotes freedom of movement. Safer for woman and fetus.
“laughing gas” inhaled anesthetic gas for labor used in the past and in other countries, gaining interest in U.S. again.
Does not completely relieve pain, but reduces perception, feeling of euphoria and reduces anxiety. Safe for mom and baby, does not affect uterine activity. Can be self-administered with face mask as needed.
Anesthesia Types:
Local Anesthesia:
1% lidocaine SQ for episiotomy or laceration repair.
Pudendal Nerve Block:
Deep injection for anesthesia in lower vagina, vulva, and perineum during forceps or vacuum repair or extensive repair to numb lower vagina, vulva, and perineum.
2nd Stage, Inject 1% lidocaine or marcaine
Spinal Anesthesia:
Typically used for cesarean sections.
local anesthetic or opioid agonist injected into subarachnoid space at 3rd, 4th, or 5th lumbar space to mix medication with spinal fluid. Used for C/S to numb from feet to nipple line.
Disadvantages spinal anesthesia: Marked hypotension (to prevent pre-load with 500-1000ml of LR or NS 15-30 min before), Impaired placental perfusion and fetal hypoxia, Ineffective breathing patterns, spinal headache from puncturing the dura mater (more common with epidurals bc catheter is larger gauge “wet tap”=treatment includes caffeine drip, oral analgesics, autologous epidural blood patch
Epidural Anesthesia:
Administered between L4 or L5 into the epidural space to numb from the abdomen down to the feet, allowing adjustments during C/S as needed.
Advantages: Woman remains alert and awake during labor, does not usually remove sensation of pressure which is helpful to assist with pushing in 2nd stage of labor. Less fetal complications than with narcotic opioids.
Disadvantages: ability to move during labor is greatly restricted, need for more interventions such as IV, f/c, continuous EFM, spinal headache can occur if dura mater is punctured, resp arrest if high spinal accidentally occurs, increased risk for infection, hypotension is common result of sympathetic anesthetic which can result in decreased uteroplacental perfusion and oxygenation to fetus urinary retention is common, increased need for oxytocin and forceps/vacuum delivery.
Combined spinal-epidural anesthesia (walking epidural): epidural needle inserted in epidural space, spinal needle threaded through to give a dose of opioid and local anesthetic intrathecally to rapidly provide analgesia. Epidural catheter inserted to be dosed later.
General Anesthesia:
Involves IV injection or inhalation to induce sleep, used primarily in emergencies or for those unable to receive spinal anesthesia.
Used in about 10% of c/s births. May be used if spinal or epidural contraindicated or not enough time or personnel to place regional block. Pt is unconscious and unaware during the delivery, must be intubated to breathe. Risks: difficulty or inability to intubate, aspiration of gastric contents.
To prepare: IV, NPO, premedicate with sodium citrate/citric acid (Bictra) to neutralize acids and decrease chance of aspiration. H2 receptor blocker like famotidine (Pepcid) or ranitidine (Zantac) to decrease production of gastric acid. Assist with cricoid pressure when intubating. Propofol, thiopental or ketamine IV (unconsciousness) and succinylcholine (muscle relaxer) administered. Nitrous oxide and oxygen are administered after intubated.